
Abstract
Background
Chordoma is a rare and aggressive primary bone sarcoma. En-block resection remains the primary treatment, but some patients are unable to undergo it due to the location and potential complications. Currently, there is no direct comparison of the effects of radiotherapy (RTH) and surgical treatment. However, retrospective analyses indicate the potential benefits of using RTH.
Methods
A retrospective analysis was conducted on 48 patients with sacral chordoma who were treated with surgery and/or radiotherapy between 2001-2020. Among those, 22 were initially treated with surgery, 19 with definitive radiotherapy, and 7 received combined treatment. The outcomes of the treatment of recurrence in 16 patients were considered. The resection margins were defined according to R classification, and the Kaplan-Meier method was employed to calculate disease-free survival (DFS) and overall survival (OS).
Results
The median (mOS) for the entire cohort was 80.6 months (95% CI: 62.3-NA), and the median (mDFS) was 40.4 months (95% CI: 35-69.5). Patients who underwent radical surgery of the primary tumor did not achieve the mOS (mean 68), while patients treated only with RTH for the primary tumor achieved an mOS of 62.3 months (95% CI: 52.1-NA). This resulted in a significant advantage of surgery over RTH in terms of OS (P = 0.01). This was not observed for DFS. The 3-year DFS rates were 65% in the surgical treatment group and 53.3% in the RTH group. The 3-year OS rates were 96% in the surgery group and 88.9% in the RTH group. In the treatment of recurrence, there were no statistically significant differences between RTH and surgery, for OS (P = 0.76).
Conclusions
Radical surgery remains the optimal treatment for sacral chordoma. For patients who are not candidates for surgical intervention, RTH offers excellent long-term outcomes. The treatment of recurrence remains a significant challenge. Comparing modern RTH techniques and surgical procedures could provide further insights.
Introduction
Chordomas were originally described in 1857 by Virchow as an extremely rare subtype of bone sarcoma. 1 The incidence of this disease is estimated at 1%–4% of all primary bone tumors, with the reported annual incidence being approximately 0.05-0.08/100 000 people.2,3 Chordomas originate from a specific tissue subtype, notochord, a rod of mesoderm that plays a crucial role in dorsal-ventral and left-right patterning within the chordate embryo. 4 Despite their differences from other bone tumors and their rare general occurrence, they are 1 of the most common subtypes of tumors developing in the axial skeleton, mainly in the area of the sacrum, mobile spine, and skull base.5-7 Initially, classified as having low malignant potential chordomas were found to present a therapeutic challenge and clinically be malignant, slow-growing, and locally aggressive tumors. 8 Due to non-specific symptoms dependent on the location of the tumor, chordomas are usually diagnosed at a significant stage of advancement. 9 Furthermore, the direct proximity and involvement of neural structures present additional challenges to treatment. 10
At present, broad en-bloc surgical resection for sacral tumors including all invaded structures, with free surgical margins, is a mainstay in the surgical treatment of sacral chordomas.11,12 The implementation of radical surgical techniques and the expansion of surgical margins have led to a notable improvement in the local control (LC) of disease recurrence in chordomas.13-15 Broad resections can be technically difficult, often necessitating the removal of nerve roots, bone, muscle, skin, and/or organs, demanding careful preoperative planning. Insufficient anterior margins might necessitate rectal resection, and because anterolateral margins lack anatomical structures that warrant extensive resection, they are thinner. 16 The efficacy of adjuvant radiotherapy (RTH) remains a subject of investigation. Some studies have indicated that adjuvant RTH does not significantly impact the survival of patients undergoing such treatment. 17 Nevertheless, patients who have undergone non-radical tumor resection may potentially benefit from the addition of RTH to improve disease control. 18 Conventional radiation therapy in old studies at doses between 40-60 Gy has only achieved a 5-year LC rate of 10%-40%, which shows that doses <60 Gy seem to be inadequate in these radioresistant tumors to achieve LC.19,20 Given the evolution of RTH strategies over time,21-26 high-dose (60-80 Gy) definitive RTH may be a beneficial treatment option, particularly for non-operative tumors. 27 Techniques like image-guided intensity-modulated conformal radiotherapy or proton therapy are recommended. Carbon ion radiotherapy has demonstrated promising outcomes for patients with inoperable sacral chordomas. A Japanese retrospective study involving 219 patients with inoperable conditions treated with hadron therapy, delivering an average of 67.2 Gy over 16 sessions, reported a 5-year LC rate of 77% and a 5-year survival rate of 84%. 28 Nevertheless, the availability of carbon ion therapy is constrained by the limited number of equipped facilities. Consequently, patients continue to receive conventional radiotherapy with stable responses. 29
Despite those advances in the treatment of sarcomas, chordomas have a high risk of recurrence, and their local growth results in serious complications and a significant deterioration of the patient’s quality of life. The reported local recurrence (LR) rate is 30%-75%. 30 The five- and 10-year overall survival (OS) rates are 70%-86% and 35%-59%, respectively.3,31,32 Moreover, approximately 30% of patients develop distant metastases, predominantly in the lungs and liver. 33 Treatment of this advanced disease is challenging, primarily due to the limited surgical options, the maximum doses of radiotherapy that can be administered, and the lack of responsiveness of the chordoma to conventional chemotherapy. 34 Currently, tyrosine kinase inhibitors represent the standard treatment for metastatic disease.35,36 Furthermore, research into the use of immunotherapy is ongoing as part of clinical trials.37,38 However, due to the rarity of the disease and the particular difficulty in treating the primary tumor and recurrence, the exact procedure remains unknown. Consequently, the pivotal issue remains the selection between radical surgery or radical radiotherapy, and the long-term survival of patients.
Consequently, a retrospective, analysis of patients with sacral chordoma treated with surgery and/or radiotherapy was conducted with the objective of evaluating survival outcomes and comparing long-term treatment outcomes between these methods. Additionally, the recurrence rate and the potential benefits of treatment in this case were analyzed.
Methods
Characteristics of the Patients
A retrospective analysis of 48 patients diagnosed with primary chordoma of the sacrum from 2001 to 2020 was conducted. All patients included at the beginning of treatment provided routine informed consent for the use of their treatment and data processing. The patients included in the analysis had undergone surgical and/or RTH treatment at the 2 referral centers. The patients underwent resection or RTH as their primary treatment. In cases where patients were not eligible for surgical intervention or if surgical intervention was anticipated to result in a substantial decline in their quality of life, RTH was the preferred treatment modality. Adjuvant RTH was employed in marginally resectable cases to facilitate the acquisition of clean resection margins. All surgical procedures were conducted following musculoskeletal tumor surgery standards and were performed by the same surgical team, to achieve clean surgical margins. The definition of R0 margins was based on the commonly used American Joint Committee on Cancer (AJCC) classification.
39
Obtaining a clean surgical margin in the sacral chordoma is difficult due to its location and proximity to key anatomical structures. Therefore, special attention was paid to classifying patients into appropriate resection groups. (Figure 1). Intraoperative photograph of the radically removed tumor with part of the sacrum. (illustrative example of a patient who was analyzed at our center).
Characteristics of Patients Included in the Analysis.
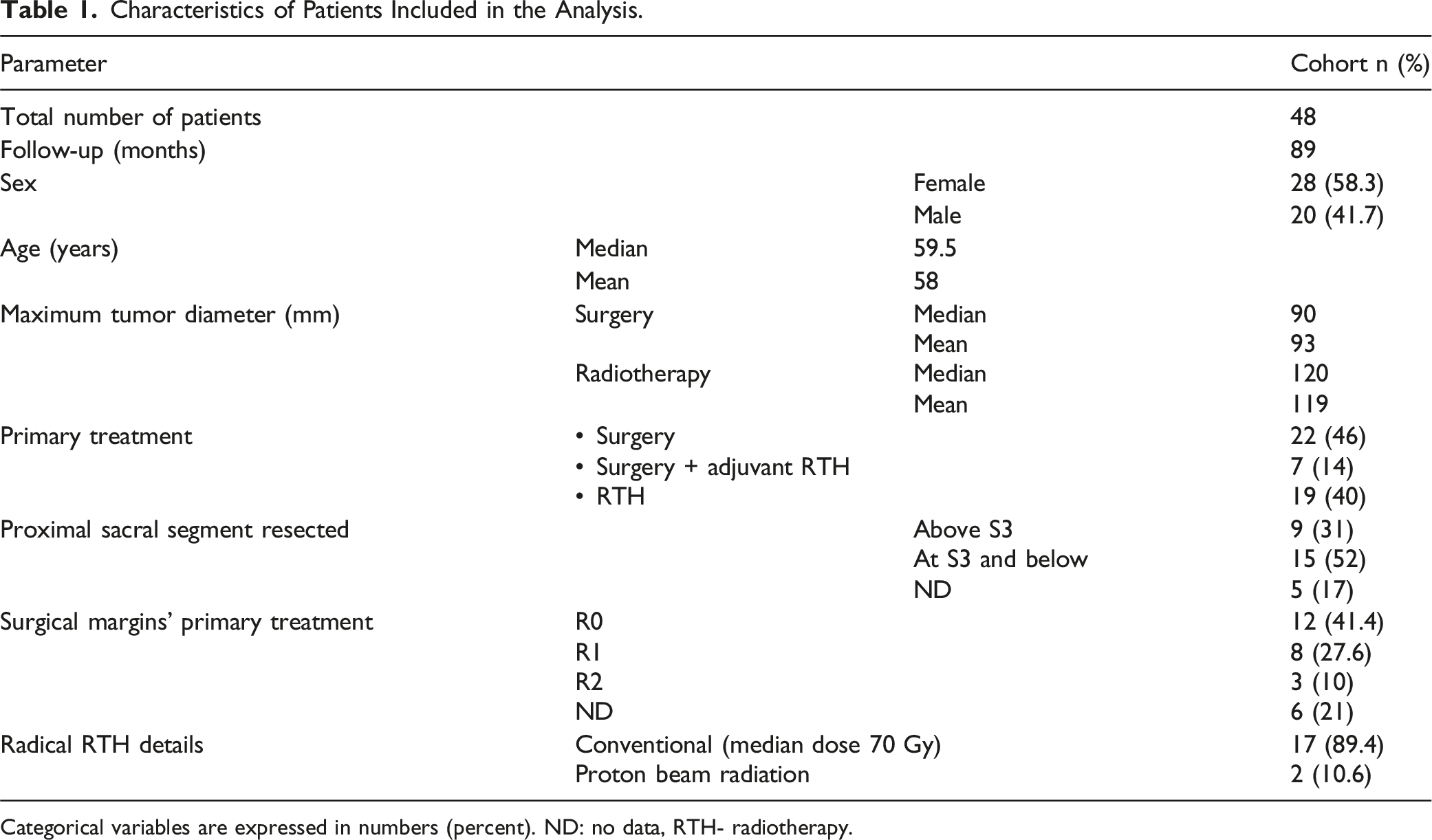
Categorical variables are expressed in numbers (percent). ND: no data, RTH- radiotherapy.
Data Collection
Patient demographics, information on therapies, tumor pathology, and diameter, as well as detailed descriptions of surgical techniques and postoperative outcomes, were collected retrospectively from medical records. Surgical margins were classified following the R classification system. 16 The reporting of this study conforms to the STROBE statement. 40
Statistical Analysis
The Kaplan-Meier method was utilized to calculate both OS and disease-free survival (DFS) rates. The period of OS was measured from the date of diagnosis to the date of death or the last follow-up, whereas the DFS period was determined from the date of diagnosis to the date of either local or distant disease recurrence. Survival curves were analyzed and compared using the log-rank test. A P-value less than 0.05 was considered statistically significant. All statistical analyses were carried out using R project Software. 41
Results
The average follow-up was 89 months (13-256 months). Twenty-nine patients (60%) underwent initial surgery. The team offered conventional adjuvant RTH to 7 patients with inadequate resection ( R1 resection in 4 cases, R2 in 2 cases, and R0 in 1 case). RTH was the primary treatment (dose range 50-70 Gy) in the remaining 19 patients (40%). All patients were followed closely after surgery, and none were lost to follow-up. One patient developed metastatic disease during the follow-up period. After primary treatment, recurrence was diagnosed in 16 patients (33.3%), and treated by RTH alone in 9 patients, resection alone in 4 patients, and RTH and resection in 3 patients.
Primary Treatment Outcomes
The median (mOS) for the entire cohort was 80.6 months (95% CI: 62.3-NA months) and the median (mDFS) was 40.4 months (95%CI: 35-69.5 months) (Figure 2). Patients who underwent radical surgical treatment of the primary tumor did not achieve the mOS (mean 68 months), while patients treated only with RTH for the primary tumor achieved an mOS of 62.3 months (95% CI: 52.1-NA months). This is associated with a statistically significant benefit in terms of OS for patients undergoing surgery (P = 0.01) (Figure 3A). However, this trend did not persist for mDFS. Patients initially undergoing surgery achieved mDFS of 50.9 months (95% CI: 32.4-NA months), while patients who underwent RTH achieved 40.4 months (95% CI: 30.2-NA months) (P = 0.77) (Figure 3B). (A) Overall survival (OS) of all patients treated for sacral chordoma. (B) Disease-free survival (DFS) of all patients treated for sacral chordoma. (A) Overall survival (OS) in patients treated for chordoma with surgery or radiotherapy. (B) Disease-free survival (DFS) in patients treated for chordoma with surgery or radiotherapy.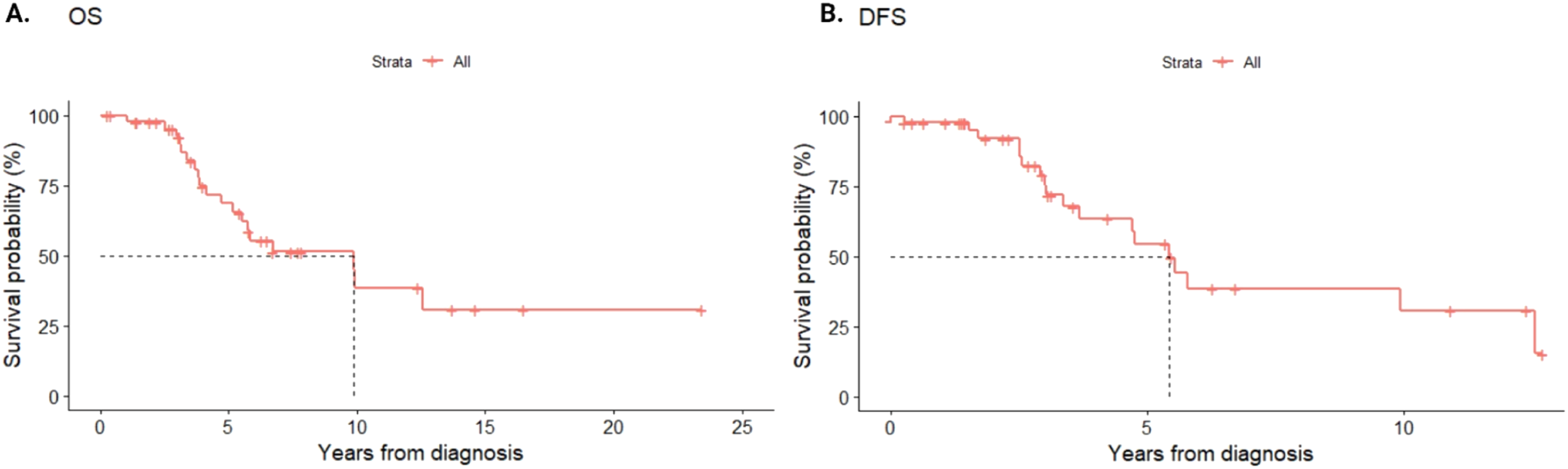

1,3,5-Year Disease-free Survival (DFS) and Overall Survival (OS) Rates Depending on the Treatment Strategy Used in Patients With Primary Chordoma.

As anticipated, the median size of lesions in the RTH group was larger than in the surgery group, with a median size of 12 cm vs 9 cm, respectively. Nevertheless, there were no significant differences in survival (P = 0.25) nor local progression (P = 0.61) between lesion sizes of <10 cm vs >=10 cm (Figure 4). (A) Overall survival (OS) in patients treated for chordoma depending on the tumor size. (B) Disease-free survival (DFS) in patients treated for chordoma depending on the tumor size.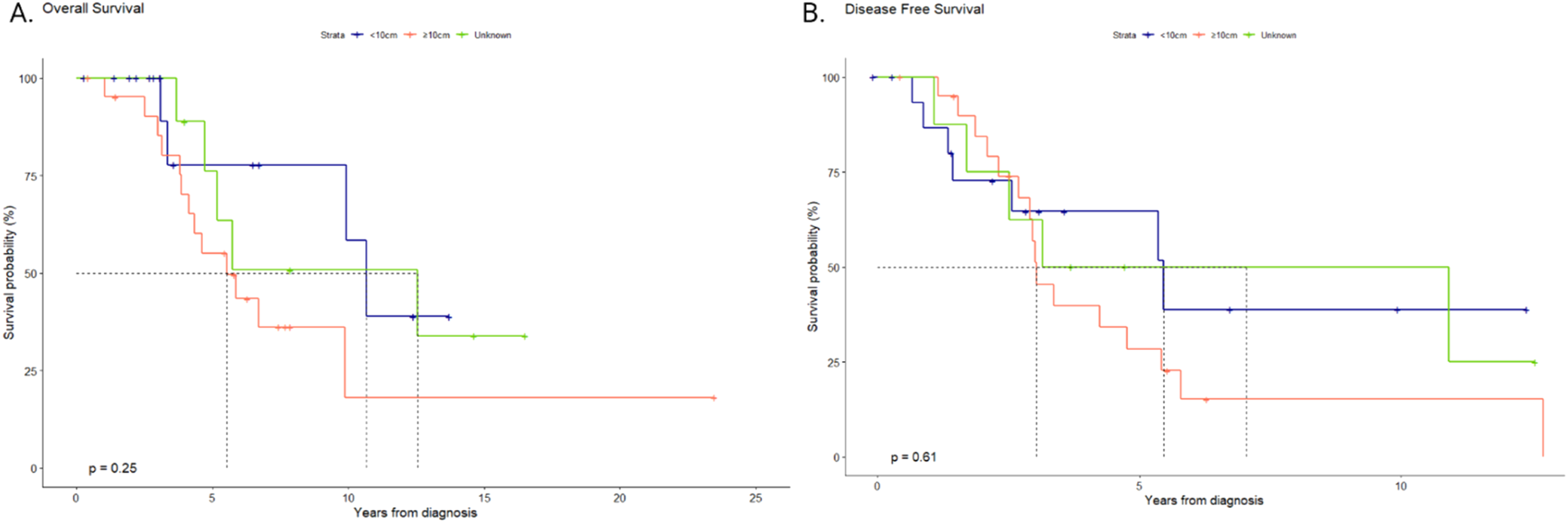
Furthermore, operative margins did not influence long-term treatment outcomes, as evidenced by OS and DFS. The resection status was available for 23 of 28 patients in the analyzed group of patients (82%). Twelve patients underwent an R0 resection, 8 underwent an R1 resection, and 3 underwent an R2 resection. A significant difference in OS or DFS was not identified (P = 0.42 in both cases) (Figure 5). Nevertheless, a trend towards superior DFS was observed in the surgical group (Figure 5B). (A) Overall survival (OS) in patients treated for chordoma depending on the surgical margin. (B) Disease-free survival (DFS) in patients treated for chordoma depending on the surgical margin.
In this study, 30% of patients, comprising 8 individuals, experienced perioperative complications, with the majority occurring within the first-month post-surgery. Among these cases, only 1, which was related to wound complications, developed as a late complication. Twenty-six percent of patients experienced postoperative wound issues, necessitating 1 patient undergoing revision surgery for debridement. No radiotherapy-related complications were reported.
Treatment of the Recurrence
Among the patients who received RTH for recurrence, 8 received proton beam radiation and 4 received conventional radiotherapy (median dose 70 Gy) (Figure 6). The mean duration of recurrence-free survival (RFS) was 10.4 months (95% CI: 9.2-11.6 months), with 67.5% of patients remaining recurrence-free within a 12-month observation period. In the event of recurrence, neither surgical nor radiotherapeutic techniques demonstrated any benefit to OS (P = 0.76) (Figure 7). Conventional radiotherapy plan of (A) the primary chordoma (dose 70 Gy/2 Gy) (B) the recurrence of chordoma after surgery (dose 70 Gy/2 Gy). Overall survival (OS) in patients treated for chordoma recurrence with surgery or radiotherapy.

The results of the Cox regression analysis indicated that female patients exhibited a 21% reduced risk of recurrence compared to their male counterparts (HR 0.79, 95% CI: 0.13-4.8, P = 0.8). Furthermore, an inverse relationship was observed between age and recurrence risk. Specifically, a 36% reduction in recurrence risk was associated with a 10-year increase in age (HR 0.96, 95% CI: 0.9-1.01, P = 0.16). However, these findings did not reach statistical significance.
Discussion
At present, there is a lack of clear guidance regarding the use of RTH in the treatment of chordoma, either as an adjuvant or definitive treatment. En-bloc tumor-sacrum resection remains the primary treatment for primary sacral chordoma, with the goal of achieving negative microscopic margins. It appears that particle RTH may offer comparable outcomes, yet the available data is limited. Moreover, there is a paucity of data retrospectively comparing surgical treatment with different types of RTH. 16 A significant increase in LR rates was observed in patients who underwent en bloc resection, in which the tumor capsule was entered during surgery, in comparison to those who underwent a complete en bloc excision with the capsule intact. This highlights the importance of adequate surgical margins. 42 Moreover, other studies have confirmed the advantage of pursuing a more aggressive surgical approach during the initial surgical intervention for sacral chordomas. 43 Neoadjuvant RTH is intended to improve resectability and may help preserve critical structures during surgery. The high-dose neoadjuvant stereotactic RTH regimen yielded a 2-year local control rate of 96% (95% CI 74%-99%) in the neoadjuvant treatment group. Notably, no patient in this group experienced LR. 44 The efficacy of adjuvant RTH remains a subject of investigation. Some studies have indicated that adjuvant RTH does not significantly impact the survival of patients undergoing such treatment. 17 Nevertheless, patients who have undergone non-radical tumor resection may potentially benefit from the addition of RTH to improve disease control. 18 As previously mentioned, the efficacy of traditional RTH techniques, which are based on relatively low doses, appears to be ineffective in the treatment of chordomas. Techniques such as image-guided intensity-modulated conformal radiotherapy or proton therapy are recommended. Stereotactic radiotherapy permits the delivery of high-dose treatments over a few sessions, typically constrained to treating small tumor volumes. However, for correctly selected spinal chordomas, it is possible to treat gross tumors to 24 Gy in a single fraction with low treatment-related morbidity and good tumor control as either a definitive or adjuvant treatment.45,46 Stereotactic radiotherapy may also be employed as a treatment for inoperable chordoma cases presenting with local or metastatic recurrences. A study on salvage stereotactic radiotherapy among patients with inoperable chordomas demonstrated benefits even in the case of recurrence, with a median progression-free survival of 24 months, mOS of 33.9 months, and a LC rate of 84.6% in the first year. 47 The advent of hadron therapy, which employs high-dose protons or charged particles such as carbon ions, helium, or neon, has enabled the direct delivery of higher radiation doses to tumor sites while minimizing damage to adjacent tissues and enhancing radiobiological effects. 48 This form of therapy offers significant improvements over traditional photon-based radiation therapy in the treatment of chordomas because it allows high-dose administration and sparing of critical organs. While comparisons between photon and hadron therapy in clinical trials are lacking, initial findings indicate that hadron therapy, especially when combined with surgical intervention, holds considerable promise and may be at least as effective, if not more so, than photon therapy. In particular, proton therapy is typically employed as an intervention for the treatment of spinal chordoma. Long-term results indicate a >90% LC rate for primary chordomas after a median follow-up of 7.3 years, with only 1 out of 23 (4.3%) patients experiencing a LR. It is noteworthy that none of the 7 patients who underwent R0 resection experienced a LR. 49 This finding supports the significance of surgical resection in achieving the best possible local control. As previously mentioned, the challenge posed by the treatment of recurrence is a significant concern. Even optimal surgical treatment with high-dose RTH failed to achieve a significant advantage among those patients. 50
Our findings indicate that radical surgical resection of the primary tumor is the only treatment modality that has a lasting effect on improving patient survival (P = 0.01). This was related to the qualification of patients for the surgical procedure vs RTH if the possibility of radical resection was questionable. However, this treatment approach did not have a significant impact on DFS in our cohort of patients (P = 0.77). Long-term treatment outcomes were numerically superior in the surgical group, with 3- and 5-year OS of 96% and 76%, respectively, in comparison to 88.9% and 51.4% in the definitive RTH group. Although tumors treated with RTH were larger than those treated surgically, there were no significant differences in OS and DFS in the group with tumors <10 cm and >=10 cm (P = 0.25; P = 0.61, respectively). Additionally, the extent of the surgical procedure did not reach a statistically significant difference between patients who underwent R0 resection and those who underwent R1/2 resection. In our cohort of patients, complications related to the treatment applied occurred only in the surgically treated group (30% of patients) and were predominantly associated with complicated wound healing. A comparison of the outcomes of patients treated at our center for recurrence revealed that neither surgical treatment nor RTH resulted in any improvement in OS (P = 0.76). However, the recurrence rate was 33.3%, with the mean duration of RFS being 10.4 months (95% CI: 9.2 to 11.6 months). For patients initially deemed inoperable who have undergone radiotherapy as a primary treatment option, the management of subsequent recurrences remains a substantial challenge.
The conclusions of our report are consistent with those of previous analyses. It was indicated that the 5-year survival rates in the group of patients treated with surgery vs definitive RTH were 79.7% and 61.9%, respectively, which is similar to our group. 29 Nevertheless, studies have demonstrated that the incorporation of RTH into surgical treatment does not significantly impact OS or local disease control.11,51 More recent reports utilizing contemporary RTH techniques have demonstrated excellent LC and patient survival. A study of 100 patients treated with proton therapy achieved a 3-year OS rate of 83% with no grade ≥3 toxicities. 52 A meta-analysis of outcomes after carbon ion RTH revealed that the OS rates at 3, 5, and 10 years in the included studies were 93%, 85%, and 69%, respectively. 53 Nevertheless, even a study comparing carbon ion RTH and en-bloc surgery did not demonstrate any differences in OS between these groups (68.1 months vs 58.6 months; P = 0.57). 26 Newer particle-based techniques offer distinct advantages in the context of treatment over conventional RTH. 54 A direct comparison of the results of RTH and surgery remains a topic of further debate. Our analysis indicated a potential advantage of surgical treatment, yet further prospective studies are necessary to confirm this hypothesis. The SACRO study, a randomized controlled trial that directly compares these techniques, is currently underway (NCT02986516). With regard to the treatment of recurrence, studies have demonstrated that the 5-year OS ranged from 50 to 67%, while the 10-year OS exhibited a significant degree of variability between studies, with values ranging from 19 to 50%.34,55 As previously stated, the treatment of recurrence remains a clinical challenge. Despite reports of benefits from surgery among these patients, our study did not observe a trend of OS benefits with either surgery or RTH.
Nevertheless, our study, like other previous reports, is subject to certain limitations. These include its retrospective nature, small sample size, and potential bias due to the qualification for treatment in relation to tumor size and surgical options. Furthermore, our study includes all patients treated for sacral chordoma in our institutions, excluding sample size calculations. A noteworthy limitation of our study is the inclusion of patients treated with conventional radiotherapy, given the superiority of more modern techniques in this indication, which has been demonstrated.
Conclusion
The results of our cohort study may indicate that radical resection with negative margins should remain the cornerstone of treatment for chordoma. Although we were unable to demonstrate a significant impact of radiotherapy on patient prognosis, long-term 3- and 5-year OS and DFS are favorable in the group of patients who cannot be offered surgical treatment. The utilization of more advanced radiotherapy techniques is likely to further enhance the efficacy of this treatment approach. The results of a clinical trial directly comparing radical radiotherapy and surgical treatment in chordoma are also awaited, which may confirm our reports. Nevertheless, the treatment of recurrence remains a significant concern, as our study revealed that none of the therapies demonstrated a clear benefit to the patients.
Supplemental Material
Supplemental Material - Long-Term Outcomes of Patients Diagnosed With Sacral Chordoma in a Retrospective Multicenter Study
Supplemental Material for Long-Term Outcomes of Patients Diagnosed With Sacral Chordoma in a Retrospective Multicenter Study by Aneta Maria Borkowska, Andrzej Pieńkowski, Paulina Chmiel, Tomasz Skóra, Radosław Michalik, Piotr Rutkowski, and Mateusz Jacek Spałek in Cancer Control.
Footnotes
Author contributions
Conceptualization A.M.B, A.P, P.R; study design A.M.B, A.P, P.R; data acquisition A.M.B, A.P, M.J.S, R.M, T.S, P.R; quality control of data and algorithms A.M.B, P.C; statistical analysis A.M.B, P.C.; manuscript preparations A.M.B, P.C; manuscript editing A.M.B, P.C; manuscript review M.J.S, P.R. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.