
Abstract
Purpose:
Although breast conservation surgery(BCS) followed by adjuvant radiotherapy is now the mainstream treatment method for breast ductal carcinoma in situ(DCIS), mastectomy is still performed in some patients who refuse to undergo radiation. However, the most effective treatment method for these patients is still unknown. In the current study, we aimed to compare the survival rates between mastectomy and BCS plus adjuvant radiotherapy in patients with DCIS.
Materials and Methods:
We performed a retrospective study of 333 patients with DCIS from May 2004 to December 2016. There were 209 patents who were treated with BCS and adjuvant radiotherapy, while the remaining of 124 patients underwent mastectomy. The disease-free survival (DFS) and local recurrence-free survival(LRFS) rates were compared between the 2 treatment groups. Cox proportional hazards regression was performed to explore factors associated with DFS and LRFS.
Results:
The 10-year local recurrence(LR) rates in the mastectomy and BCS plus adjuvant radiotherapy groups were 2.6% and 7.5%, respectively. There was no difference in the LR rate between the 2 groups. Furthermore the DFS rate was also similar between the mastectomy and BCS plus adjuvant radiotherapy groups. Based on the multivariable analysis, age and tumor grade were significantly correlated with the LRFS and DFS rates. In the subgroup analysis based on the factors of age and tumor grade, patients with a tumor grade of III who underwent mastectomy had better LRFS and DFS rates compared to those who received BCS plus radiotherapy.
Conclusion:
In patients with DCIS, the long-term efficacy was similar between mastectomy and BCS followed by adjuvant radiotherapy. However, in the subgroup of patients with grade III tumors, mastectomy seems to offer a better LRFS and DFS than BCS plus radiotherapy.
Introduction
Ductal carcinoma in situ (DCIS) accounts for approximately 20-25% of all diagnosed breast cancers. 1 Given its non-invasive nature, patients with DCIS have a quite favorable long term prognosis with >95% 10-year overall survival(OS) rate. 2 Although surgery plus intra-operative radiotherapy is emerging as a new treatment option for DCIS, the main treatment methods are still mastectomy and breast conservation surgery(BCS) with or without radiotherapy. 3 -5 In a large population study from the United Kingdom, the percentage of patients who received only BCS, BCS plus radiotherapy, and mastectomy were 26.3%, 40.4%, and 29.8%, respectively. Furthermore, mastectomy was found to be performed more commonly in patients with a tumor of high-grade (36%) compared to that of low-grade (15%). 6 The authors of several large clinical trials have shown that adjuvant radiotherapy can bring improved local control for DCIS and therefore, most patients with DCIS are currently treated with BCS plus radiotherapy with reported 10-year local recurrence (LR) rates of 1.5-15.0%. 7 -12 In addition to improving local control, adjuvant radiotherapy after BCS could also provide better overall survival. 2
In clinical practice, patients with DCIS can also have concomitant lobular carcinoma in situ (LCIS), which was considered a risk factor for breast cancer. 13 -15 However, the incidence of LCIS is much lower than DCIS with approximately 2.75 cases per 100,000 women(representing 1-2% of all breast cancers). 16,17 Similar to DCIS, the long-term prognosis of LCIS is very good with a 10- and 20-year cancer-specific overall survival rate of 98.9% and 96.3%, respectively. 18,19 If patients with DCIS also had synchronous ipsilateral LCIS, they were likely to suffer double the risk of contralateral breast cancer tumor recurrence. 13
Patients with DCIS may choose to undergo mastectomy for various reasons such as no desire of breast conservation or refusal of adjuvant radiotherapy. The efficacy of mastectomy for treating DCIS has been reported in several studies and the local recurrence(LR) rate in those patients treated by mastectomy was approximately 1.9-6.3%. 20 -22 However, there are currently no randomized trials to show the comparison of efficacy between mastectomy and BCS plus radiotherapy in the management of DCIS. Therefore, the treatment modality with the best tumor control efficacy in DCIS remains unclarified.
In our study, we have compared the efficacy between mastectomy and BCS plus radiotherapy for the treatment of patients with DCIS at our institution. Additionally, we also attempted to identify clinical factors associated with the tumor prognosis and explored their relationship with the selection of treatment method.
Material and Methods
Ethics Statement
Our current study was conducted according to the principles of the Institutional Review Board of Sun Yat-Sen Memorial Hospital. The design of our research was retrospective and therefore, written consent was not required from the included patients at our hospital.
Patients
Patients enrolled in our study were selected from the clinical database at our hospital. This database stores the patient’s information, such as age, sex, diagnosis, treatment history, medical examination reports, and follow-up data. Patients selected for the present study met the following criteria: (1)pathologic diagnosis of pure DCIS; (2)underwent mastectomy or BCS followed by adjuvant radiotherapy; (3)no history of other malignant tumor or contralateral breast cancer history; (4) all the related clinical information was available. Patients who received intraoperative radiation were excluded. A total of 333 patients were included for our analysis.
Treatment
Surgery was performed in all the patients. The types of surgery included in our study were mastectomy and BCS. For patients who received BCS, a negative surgical margin confirmed by pathology was achieved in all. After surgery, adjuvant radiotherapy was scheduled in the patients who underwent BCS with the aim of improving local control. Radiotherapy was usually conducted with 6- or 10-MV photons. The prescription dose for the whole breast was 50Gy/25F. When the radiation of the whole breast was completed, a boost to the tumor bed was administered in about 50% of the patients. However, the application of boost radiotherapy to patients was based on the physicians’ decision which was made according to their experience and the patient’s general condition. Additionally, endocrine therapy was suggested for patients with estrogen receptor (ER)- and/or progesterone receptor (PR)-positive disease.
Follow Up
Patients were recommended to visit their physician every 3-6 months in the first 5 years after treatment. Then, patients were asked to undergo evaluations annually until 10 years and every 2 years after that. Physical examinations and ultrasonography were usually performed at each visit. Examinations using mammography and computed tomography were usually performed annually. Disease-free survival (DFS) was defined as time from diagnosis to local or distant failures. Similarly, local recurrence-free survival (LRFS) was defined as the time from diagnosis to ipsilateral breast recurrence.
Statistical Analysis
Statistical analyses were performed by using SPSS software, version 19.0. We used the chi-square test or Fisher’s exact test to analyze categorical variables. Student’s t test or the Mann–Whitney U test was employed to do the analysis for all continuous variables. The survival data were estimated by using the Kaplan–Meier method and differences between patient groups were compared using log rank test. Multivariate Cox regression was performed to find significant predictors of DFS and LRFS. Results with a p-value of <0.05 were considered to be significant.
Results
Clinical Characteristics
Among the 333 patients included in our present study. Among them, 209 patients underwent BCS followed by adjuvant radiotherapy, while the remaining 124 patients were treated with mastectomy. Therefore, all patients were divided into 2 groups based on the treatment method. Compared to patients who received BCS plus radiotherapy, those who underwent mastectomy showed no differences in tumor size, ER status, PR status, adjuvant endocrine therapy and follow-up. However, patients in the mastectomy group had a higher tumor grade than those in the BCS group. A higher proportion of elderly patients and patients with human epidermal growth factor receptor 2(HER2) positive status were also observed in the mastectomy group than that in the BCS plus radiotherapy group (Table 1).
Clinical Characteristics.

Comparison of Survival Between BCS Plus Radiotherapy and Mastectomy Groups
There were 3 patients who died during follow-up. The 10-year overall survival(OS) rates were similar in the BCS plus radiotherapy and mastectomy groups (98.8% vs. 97.7%, respectively; p = 0.855; Figure 1). Sixteen patients developed disease recurrence and the pathology of recurrence was all invasive cancer. Among those with recurrence, 13 patients suffered only local recurrence and 1 patients developed only distant metastasis. Two patients were observed to have both local and distant failures. The sites of distant metastasis were bone (2 cases) and subcutaneous tissue of upper extremity(1 case). The 10-year DFS rate was also not significantly different between the BCS plus radiotherapy and mastectomy groups (91.4% and 97.4%, respectively; p = 0.109; Figure 2).

OS for the whole group of patients. There was no significant difference in OS between patients treated by mastectomy and patients treated by BCS plus adjuvant radiotherapy (p = 0.855).

DFS for the whole group of patients. There was no significant difference in DFS between patients treated by mastectomy and patients treated by BCS plus adjuvant radiotherapy (p = 0.109).
Comparison of Recurrence Pattern Between BCS Plus Radiotherapy and Mastectomy Groups
In the BCS plus radiotherapy group, local recurrence was found in 11 patients and distant metastasis was found in 1 patients. One patient had both local and distant failures. In the mastectomy group, 3 patients had recurrence (One patients suffered both local and distant recurrences and the other 2 patients recurred only locally). We found that the rate of LR rate was similar between patients who received BCS plus radiotherapy and those who underwent mastectomy(7.5% vs. 2.6%, respectively; p = 0.151; Table 2). Similarly, no difference was found in the rate of distant metastasis between the 2 groups(2.5% vs. 1.8%; p = 0.820; Table 2).
Recurrence Patterns for the Whole Group Patients.

Abbreviations: LR = local recurrence; DM = distant metastases; BCS = Breast-conservation surgery.
Clinical Predictors for DFS and LRFS for All the Patients
In order to investigate the potential clinical factors associated with DFS and LRFS in patients with DCIS. Based on the results of the univariate analysis, only age and tumor grade were predictors of DFS and LRFS(Table 3), while, the other factors including treatment method failed to predict both DFS and LRFS. Next, the multivariable analysis was performed to confirm the results from univariate analysis and We found that age and tumor grade remained as significant factors associated with DFS and LRFS in the multivariate analysis. The treatment method was not found to be associated with DFS and LRFS, which further confirmed our initial results and indicated that there was no difference in survival between patients undergoing BCS plus radiotherapy and those receiving mastectomy(Table 4).
Univariate Analysis of DFS and LRFS for the Whole Group.

Abbreviation: DFS = disease-free survival; LRFS = local-recurrence free survival; BCS = Breast-conservation surgery.
Multivariate Analysis of DFS and LRFS for the Whole Group.
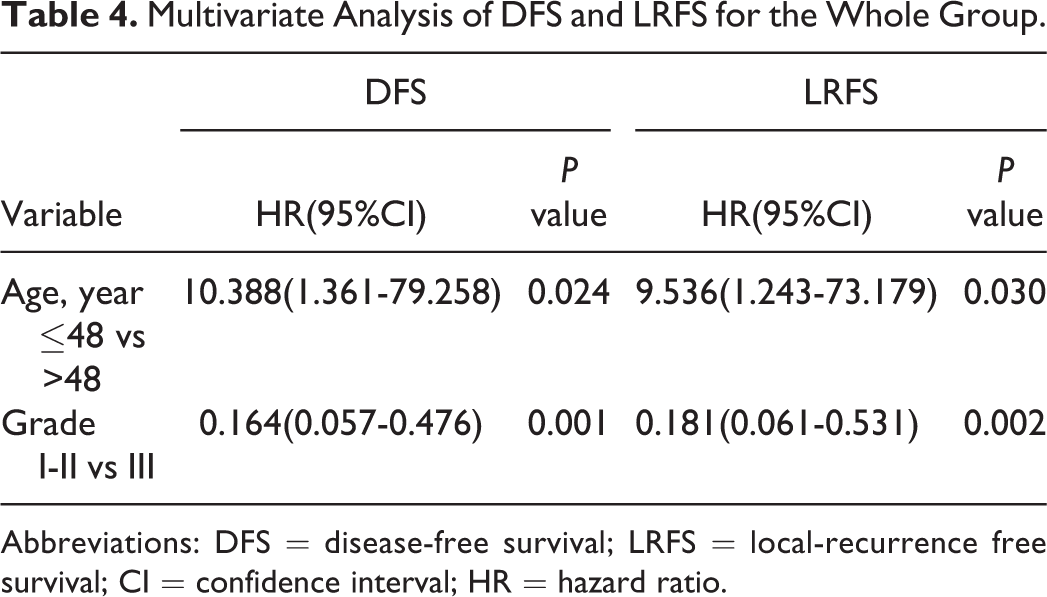
Abbreviations: DFS = disease-free survival; LRFS = local-recurrence free survival; CI = confidence interval; HR = hazard ratio.
Subgroup Analysis Based on the Factor of Age
We performed further subgroup analysis based on age and tumor grade, which were factors correlated with the DFS and LRFS, to determine whether the treatment method would affect survival in these subgroups. In the aged ≤48 years subgroup, 15 patients developed recurrence. The 10-year DFS and LRFS rates were 89.6% and 91.0%, respectively, in the BCS plus radiotherapy group and 95.1% and 95.1%, respectively, in the mastectomy groups. There were no significant differences in the DFS and LRFS rates between the 2 treatment groups (p > 0.05; Table 5).
DFS and LRFS for the Patients With Young Age.
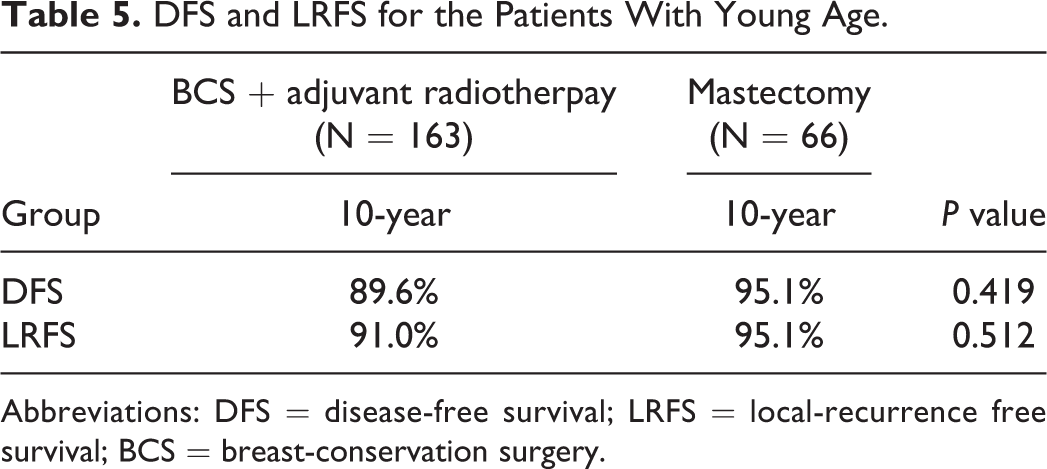
Abbreviations: DFS = disease-free survival; LRFS = local-recurrence free survival; BCS = breast-conservation surgery.
In patients aged >48 years, recurrence was observed in only 1 patient. Specifically, recurrence was observed in 1 patient in the BCS plus radiotherapy group and no patients in the mastectomy group. The 10-year DFS rate was comparable between patients in the BCS plus radiotherapy and mastectomy groups. Furthermore, there was no significant difference in the LRFS rates between the 2 groups (p > 0.05; Table 6). The above results demonstrated that the similar efficacy of the 2 treatment methods was independent of age.
DFS and LRFS for the Patients With old Age.
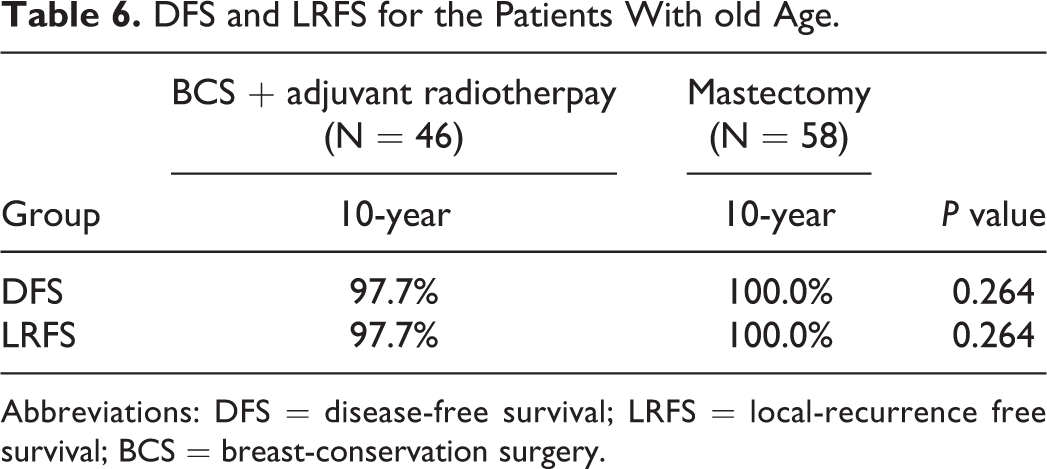
Abbreviations: DFS = disease-free survival; LRFS = local-recurrence free survival; BCS = breast-conservation surgery.
Subgroup Analysis Based on the Factor of Tumor Grade
In patients with a tumor grade of I-II, recurrence was observed in 3 patients in the BCS plus radiotherapy group and 2 patients in the mastectomy group. Both the 10-year DFS and LRFS rates were similar between patients receiving BCS plus radiotherapy and those receiving mastectomy (Table 7). In patients with grade III tumors, recurrence was found in 10 patients in the BCS plus radiotherapy group and 1 patient in the mastectomy group. Patients in the mastectomy group had significantly better DFS and LRFS rates than those in the BCS plus radiotherapy group (Table 8). These results indicated that tumor grade could be a reference for the treatment selection in patients with DCIS.
DFS and LRFS for the Patients With Tumor Grade of I-II.
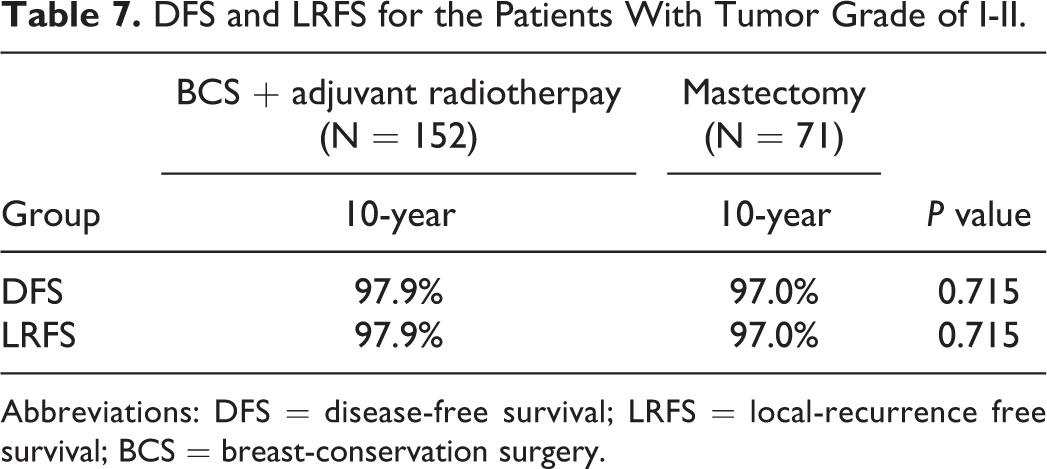
Abbreviations: DFS = disease-free survival; LRFS = local-recurrence free survival; BCS = breast-conservation surgery.
DFS and LRFS for the Patients With Tumor Grade of III.
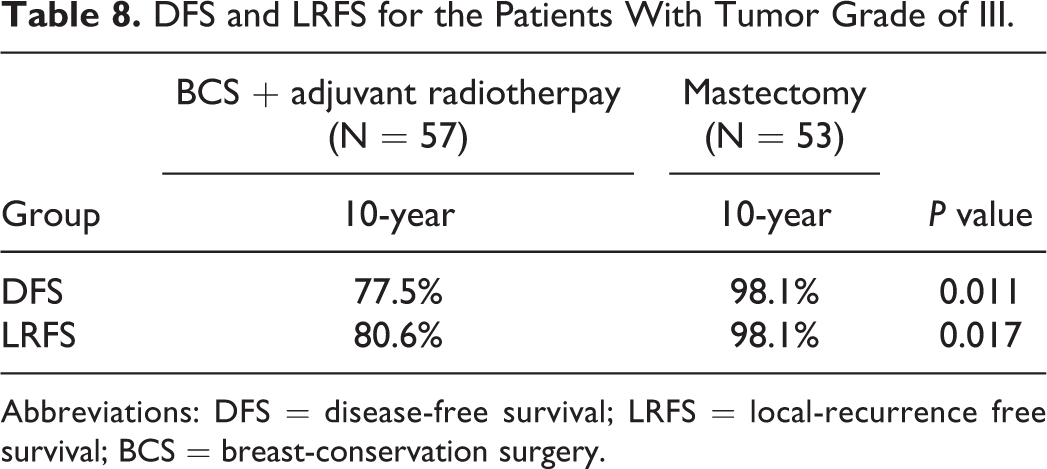
Abbreviations: DFS = disease-free survival; LRFS = local-recurrence free survival; BCS = breast-conservation surgery.
Clinical Predictors for DFS and LRFS for Patients With Tumor Grade of III Tumors
Finally, we performed multivariable analysis in order to confirm that treatment method was correlated with tumor grade in patients with grade III tumors. Based on our results, both the treatment method and PR status were significant predictors of DFS. Additionally, treatment method was also significantly associated with LRFS. Patients who received BCS plus radiotherapy had a 13.5-fold risk of having local recurrence compared to those treated by mastectomy (Table 9)
Multivariate Analysis of DFS and LRFS for Patients With Tumor Grade of III.

Abbreviations: DFS = disease-free survival; LRFS = local-recurrence free survival; CI = confidence interval; HR = hazard ratio; NA = not available.
Discussion
In our present study, we showed that the 10-year DFS and LRFS rates were comparable between patients in the BCS plus radiotherapy and mastectomy groups. There were also no difference in LR and distant metastasis rates between patients who received mastectomy and those treated with BCS followed by adjuvant radiation. We further performed multivariable analysis and found that the treatment method was still not significantly associated with DFS and LRFS. All the data just indicated that the long-term prognosis was similar between patients who underwent mastectomy and those who received BCS plus radiotherapy. Considering local tumor control, the treatment method of mastectomy is feasible for patients who have no desire for breast conservation or refuse to receive radiotherapy.
Although the treatment method was not a predictor of DFS or LRFS, the factors of age and tumor grade were found to be significantly associated with both DFS and LRFS. Young patients have a higher risk of LR than the elderly. This finding was also supported by the study of Kong et al who also found that age was a strong predictor of LR in women with DCIS who underwent BCS and radiotherapy. 23 We also showed that patients with a low/mediate tumor grade were less likely to develop LR than the patients with a high tumor grade, which was rarely reported by other studies. Other clinical factors, such as surgical margin and tumor size, has also been reported to be associated with LR. 24,25 Solin et al reported that patients with a large tumor size tended to have more ipsilateral breast recurrence compared to those with small tumors. 24 However, tumor size was not found to be correlated with LR in our study and by other researchers. 12,23 A possible reason for this may be that mastectomy or adjuvant radiation could mitigate tumor size as a risk factor because none of the patients in the study by Solin et al received radiotherapy after surgical excision.
As we know, data to compare the efficacy between mastectomy and BCS plus radiotherapy for patients with DCIS is still limited. 20,21 In a large population-based study, the cumulative incidence of LR after mastectomy, BCS plus radiotherapy, and BCS alone were 1.9%, 8.8%, and 15.4%, respectively. 20 BCS plus radiotherapy was found to be associated with a higher LR rate than mastectomy. However, the baseline characteristics were not compared between different treatment groups in that study and Cox proportional-hazards analyses only included the period of DCIS diagnosis and age as covariables, which may affect the reliability of their results. Similar findings were also reported by Frank et al in their analysis of 608 DCIS patients. 22 Conversely, one large study which enrolled 140 366 patients with DCIS showed that the 15-year breast cancer mortality rate for patients treated with lumpectomy alone, lumpectomy and radiation, and mastectomy were 2.33%, 1.74%, and 2.26%, respectively. Patients who received lumpectomy plus radiotherapy had a significantly lower risk of death than those treated by mastectomy (hazard ratio, 0.75; 95% confidence interval, 0.65-0.87). However, this study failed to report the details of LR, which is considered to be an important endpoint in evaluating the treatment modality for DCIS. Similarly, another study also reported a slightly higher rate of RR in patients treated by mastectomy than patients treated by BCS plus radiotherapy(4.5% vs 4.1%, respectively). 21 In our study, we showed that local control was favorable in patients who received mastectomy, with a 10-year LR rate of 2.6%. There was no significant difference in the LR rate between patients who received mastectomy and those who received BCS plus radiotherapy. The similar oncologic outcome observed between the 2 treatment methods was not affected by the factor of age. However, tumor grade seemed to be a reference in the selection of treatment method. The efficacy of mastectomy was equal to that of BCS plus radiotherapy in patients with a tumor grade of I-II. However, mastectomy was associated with improved local control than BCS plus radiotherapy in patients with a tumor grade of III, which could be explained by the idea that high-grade tumors showed more aggressive invasive behavior behavior and resistance to radiotherapy. Therefore, mastectomy may allow the maximum possibility for completely eradicating the tumor completely.
Clinicians may also question whether patients with DCIS can be treated with BCS alone instead of mastectomy. The study of Rakovitch et al answered this question and they found that patients treated by BCS alone had a high rate of LR(20.8%). 26 BCS plus radiotherapy is now considered to be the standard treatment for patients with DCIS, and several researchers have confirmed the improved local control associated with providing adjuvant radiotherapy to patients receiving BCS. 7 -9 Warren et al retrospectively analyzed 245 patients with DCIS who received BCS and adjuvant radiotherapy, and they found LR in only 4 patients (10-year LR rate of 1.5%). 11 However, Frank et al reported that in patients with good prognosis factors, BCS plus radiotherapy showed no advantage in local control than BCS alone. Therefore, BCS alone may be feasible in DCIS with favorable features, and this viewpoint was also supported by another small study. 27 We observed a 10-year LR rate of 7.5% in the BCS plus radiotherapy group, which was higher than that reported by Warren et al. 11 A possible reason for this may be that nearly all the patients in the study by Warren et al received a boost to the surgical cavity with a median dose of 16 Gy, while, about 50% of patients in our study were given a radiation boost. In fact, the boost has been found to improve local control in DCIS. 28 -30 As we know, mastectomy alone can provide good local control for DCIS, there was still one study which evaluated the addition of radiotherapy after mastectomy in DCIS and their data showed that no patients who received radiotherapy had an ipsilateral further event, while, in patients known not to have had radiotherapy post mastectomy, 1.6% of them had an ipsilateral event. 31 Besides, the use of adjuvant radiotherapy after mastectomy was associated with a close (<1 mm) margin, large tumor size and microinvasion. 31 In our study, although the LR was lower in the mastectomy group than that in the BCS plus radiotherapy group, the difference was not statistically significant. We also observed that compared to the BCS plus radiotherapy group, mastectomy was performed at a higher percentage in patients with grade III tumors (p = 0.004), which was consistent with another study in which tumor grade was reported as one of the factors significantly influencing the mastectomy choice for patients with DCIS. 32
There were several limitations with our study. Firstly, the sample size was relatively small because the number of DCIS patients at our institution was limited. Secondly, this was a retrospective study and we could not avoid the possibility of selection bias. However, the strength of our study was that we found tumor grade as an important factor in influencing the treatment strategy. Furthermore, mastectomy may be more feasible for patients with tumor grade III tumors. For patients who are reluctant to undergo radiotherapy which can cause the organ toxicity, 33 -36 mastectomy is an alternative option.
Conclusion
In conclusion, both mastectomy and BCS plus radiotherapy were feasible for DCIS regarding the long-term prognosis. However, in subgroup of patients with tumor grade III tumors, mastectomy provide a more beneficial survival rate. A further large prospective clinical trial is needed to confirm our findings.
Footnotes
Author Contributors
Kai-yun You, MD, Zhuo-fei Bi, MD, and Yu-jia Ma, BD are authors equal contributors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
Our current study obtained approval from Institutional Review Board of Sun Yat-Sen Memorial Hospital. Since the study design of our research was retrospective, there was no requirement of written consent from included patients in our hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant 2020ZX09201021 from the National Science and Technology Major Project, grant YXRGZN201902 from the Medical Artificial Intelligence Project of Sun Yat-Sen Memorial Hospital, grants 81572596, 81972471, and U1601223 from the National Natural Science Foundation of China, grant 2017A030313828 from the Natural Science Foundation of Guangdong Province, grant 201704020131 from the Guangzhou Science and Technology Major Program, grant 2017B030314026 from the Guangdong Science and Technology Department, grant 2018007 from the Sun Yat-Sen University Clinical Research 5010 Program, grant SYS-C-201801 from the Sun Yat-Sen Clinical Research Cultivating Program.