
Abstract
Objectives
Surgery is the mainstream treatment for early-stage esophageal squamous cell carcinoma (ESCC) and occult recurrent laryngeal nerve lymph node metastasis (RLNM) is not uncommon among those with R0 resection. The clinical value of postoperative radiotherapy (PORT) in patients with RLNM only is still controversial.
Methods
Consecutive patients with early-stage ESCC treated with R0 resection and pathologically confirmed RLNM only from June 2012 to July 2022 were retrospectively reviewed. PORT, covering the supraclavicular and superior mediastinum area (small T-field) at a dose of 50.4 Gy for 28 fractions, was performed in some patients. Propensity score matching (PSM) was performed to balance the baseline characteristics between patients with or without PORT. Pattern of failure, disease-free survival (DFS), and overall survival (OS) were compared.
Results
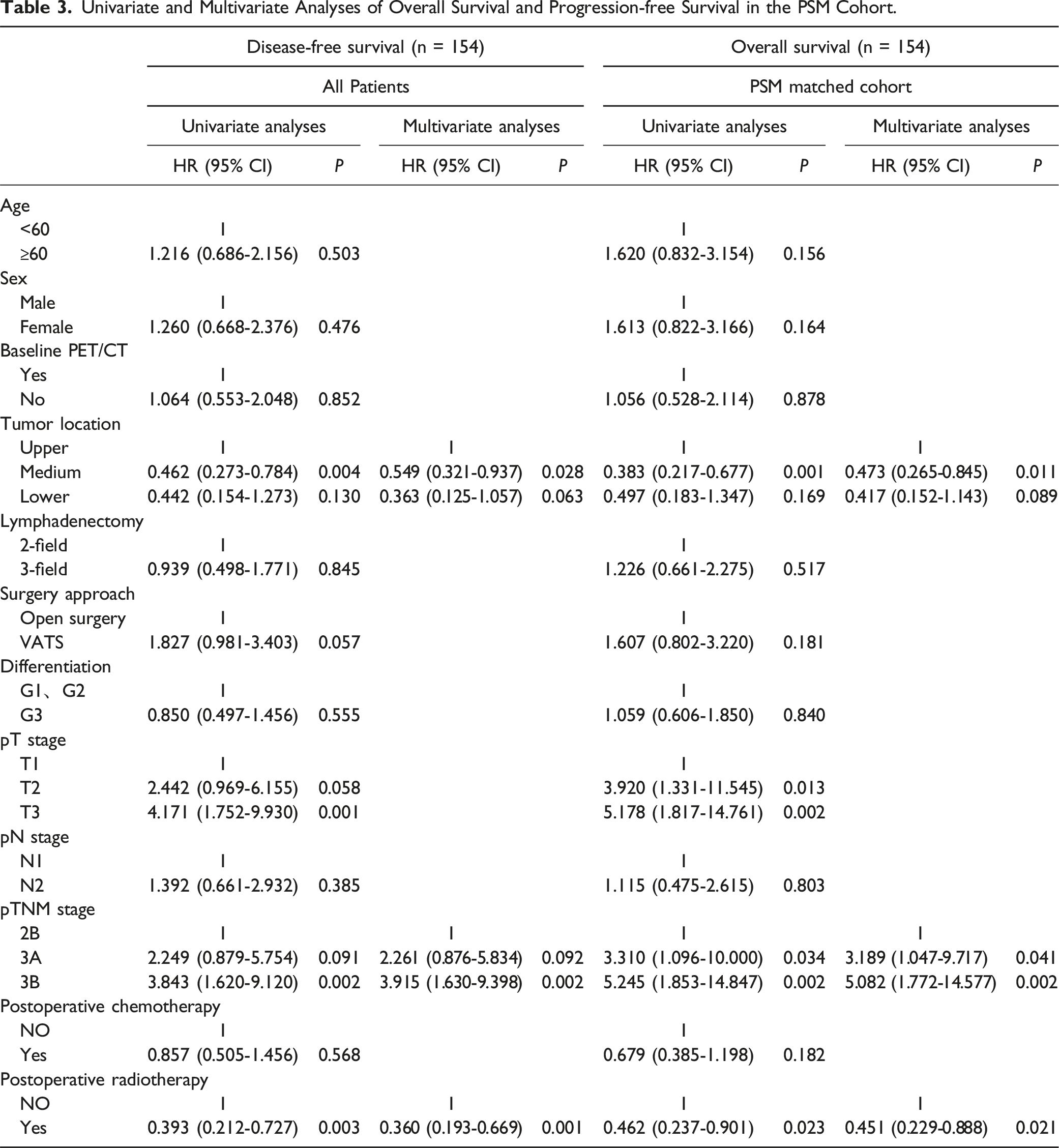
Among the 189 patients identified, 69 (35.5%) received PORT and the other 120 (63.5%) did not. After PSM, 154 patients were included in the matched cohort, including 62 in the PORT group and 92 in the non-PORT group. With a median follow-up of 48 (95% CI: 40.3-55.7) months, 69 patients developed their initial disease recurrence in the whole population and PORT significantly decreased the frequency of local recurrence (61.2% vs 21.4%) among those with recurrent disease. Additionally, in the PSM matched cohort, PORT significantly prolonged patients’ DFS (HR 0.393, P = 0.002) and OS (HR 0.462, P = 0.020). Moreover, PORT remained as the independent factor associated with improved DFS (HR 0.360, P = 0.001) and OS (HR 0.451, P = 0.021) after multivariate Cox analyses. In addition, tumor location and pathological TNM stage were found to be independent prognostic factors associated with survival outcomes.
Conclusion
PORT is associated with improved DFS and OS in ESCC patients with R0 resection and RLNM only, which warrants future validation.
Keywords
Introduction
Esophageal cancer is the sixth leading cause of cancer deaths and the seventh most common cancer worldwide.1,2 Neoadjuvant chemoradiotherapy is currently the standard treatment modality for locally advanced operable esophageal cancer, while some early to mid-stage esophageal cancers can be directly resected. 3 However, the results of surgery alone are disappointing, with 5-year survival rates ranging from 15% to 40%. 4 The pattern of failure is dominated by distant metastasis and local recurrence. 5
In patients with early to mid-stage esophageal squamous cell carcinoma (ESCC) undergoing direct surgery, the decision of whether or not to perform postoperative adjuvant radiotherapy (PORT) after R0 resection is still highly controversial, and phase III randomized controlled trials investigating the efficacy and safety of PORT in modern times are limited. 6 An RCT conducted by Xiao et al. showed that PORT improved 5-year survival compared to similar patients who did not receive radiotherapy. 7 A previous meta-analysis by Liu et al. that included 6 RCTs and 13 retrospective studies showed that PORT improves disease-free survival (DFS) and reduces the local recurrence risk. 8 Although accumulating retrospective studies support the survival benefit of PORT in ESCC patients staged with pT3-4/N + M0 after R0 resection,9,10 its clinical value has not been widely accepted. Moreover, the optimal patient selection and target volume delineation are largely unknown.
Multiple studies11,12 have indicated that the recurrent laryngeal lymph nodes are the most susceptible sites for lymphatic metastasis in esophageal cancer and serve as a significant prognostic factor. Lymph node dissection of the recurrent laryngeal lymph nodes can significantly improve the 5-year survival rate of patients with esophageal cancer.13-16 Bilateral dissection of the recurrent laryngeal lymph nodes undoubtedly improves the accuracy of staging in esophageal cancer patients and to some extent improves their prognosis, but it also increases the incidence of recurrent laryngeal nerve injury and respiratory complications during the perioperative period.17,18 Due to the unique anatomical location, the clinical value of PORT covering the mediastinum and bilateral supraclavicular lymph drainage area in those with recurrent laryngeal lymph node metastasis (RLNM) only after R0 resection, is highly debated.
Methods
Patients
Consecutive patients with ESCC receiving R0 resection and pathologically confirmed RLNM only from June 2012 to July 2022 at Fudan University Shanghai Cancer Center were retrospectively reviewed, and those meeting the following criteria were included. Inclusion criteria: (1) pathologically confirmed diagnosis of ESCC; (2) clinically stage N0 according to the TNM staging system (AJCC, sixth edition); (3) patients who did not receive any neoadjuvant therapy, such as preoperative radiotherapy or chemoradiation; (4) patients who underwent radical (R0) resection with two-field or three-field lymph node dissection; and (5) pathologically confirmed metastasis only in the recurrent laryngeal nerve lymph nodes. Exclusion criteria: (1) patients with pathologically confirmed non-squamous cell carcinoma; (2) R1 and R2 resections; (3) secondary primary malignancies; (4) patients receiving PORT which did not cover the clavicular region; (5) patients with severe complications which did not revolve within 3 months after surgery; and (6) incomplete follow-up. We defined pathological stage according to the AJCC eighth edition of the esophageal cancer staging system.
19
The inclusion processes were summarized in Figure 1. For each patient, age, gender, pathological type, baseline PET/CT, tumor location, status of lymph node dissection, surgical approach, differentiation degree, T stage, N stage, TNM stage, total number of dissected lymph nodes, status of postoperative chemotherapy, detailed information about PORT including target volume, dose fractionation, date of treatment initiation and completement, were collected. The present study was approved by the institutional review board and the independent ethics committee of Fudan University Shanghai Cancer Center (FUSCC, approval number: 2202251-5). The study was conducted in accordance with the Helsinki Declaration (as revised in 2013). Since this was a non-randomized retrospective analysis and the data were de-identified and analyzed anonymously, the requirement for informed patient consent was waived. The reporting of this study conforms to STROBE guidelines.
20
Flowchart of patient enrollment and study design. Abbreviations: RLNM = recurrent laryngeal nerve lymph node metastasis; PORT = postoperative radiotherapy; ESCC = esophageal squamous cell carcinoma; PSM = propensity-score matched.
PORT and Follow-Up
Some patients received PORT in a small T-shaped field that included only the bilateral supraclavicular area and the drainage areas of the lymph nodes in the upper and middle mediastinum. The clinical target volume (CTV) included bilateral supraclavicular and mediastinal lymph node drainage area (zones 2, 4, 5, and 7), and the lower boundary was 2-3 cm below the tracheal bulge. The superior, inferior, anterior, posterior and lateral borders of planning target volume (PTV) were 1 cm beyond CTV. PORT was delivered with photons (≥ 6 MV) from a linear accelerator to a total dose of 50.4 Gy in 28 fractions. Organs at risk were limited: bilateral lungs V5 ≤ 55%, V20 ≤ 25%, V30 ≤ 1 8%, spinal cord < 45 Gy, cardiac Dmean < 25 Gy.
Regular follow up was carried out for each patient, generally at 4 weeks after surgery, every 3 to 6 months for the first 2 years, and every 12 months thereafter. Throughout the follow-up period, patients underwent complete examinations, including ultrasonography (US) of the neck and abdomen and computed tomography (CT) scans of the neck, chest, and abdomen. Additionally, as part of the follow-up protocol, bone scans, positron emission tomography (PET) scans, and head-enhanced magnetic resonance imaging (MRI) were performed based on clinical symptoms, clinical signs, and chemical analyses. Tumor recurrence at the anastomotic sites and/or loco-regional lymph nodes was defined as locoregional recurrence, otherwise was defined as distant metastasis. Disease-free survival (DFS) was defined as the time from the date of surgery to the date of disease recurrence or death due to any cause. Overall survival (OS) was defined as the time from the date of surgery to death due to any cause.
Statistical Analysis
The baseline characteristics of patients with or without PORT, were summarized descriptively and compared using the chi-square test or Fisher’s test for categorical variables and the t-test or rank-sum test for continuous variables, respectively. DFS and OS were assessed using the Kaplan-Meier method and compared using the log-rank test. To address any potential biases in the comparison, propensity score matching (PSM) analysis provides a convenient way to create an approximate balance between the 2 groups by collapsing all confounders into a single value (propensity score), which is usually estimated by logistic regression. After randomly sorting the patients in the entire cohort, 1:2 near-neighbor matching was implemented with a caliper width of 0.25 standard deviations. Before and after matching, balance of covariates was assessed by the standardized mean difference (SMD) between the two groups. A SMD of 0.2 or less was considered the smallest difference. Further univariate and multivariate Cox proportional risk regressions were used to find factors associated with survival. Variables associated with DFS and OS in univariate analysis (P < 0.050) were further included in multivariate analysis. All statistical analyses were performed using SPSS version 26.0. A two-sided P value of less than 0.050 was considered statistically significant.
Results
Patient Characteristics
Patient Characteristics Stratified by Groups (Non-PORT and PORT) for all Patients and Matched Data sets.

Patterns of Treatment Failure
Patterns of Treatment Failure in Patients With Initial Disease Recurrence.

aDetailed information about the sites of recurrent disease was missing in 6 patients and thus were excluded.
Survival Outcomes
In the entire cohort, the median DFS was not reached, but there was a statistical difference between the Non-PORT and PORT groups (P = 0.006) (Figure 2(A)). The median OS was 118 months (95% CI: 63.7-172.3) in the whole population and PORT was associated with improved OS (NR vs 98 months, P = 0.030) (Figure 2(B)). In the PSM matched cohort, PORT was also associated with prolonged DFS (P = 0.002, Figure 2(C)) and OS (NR vs 73 months, P = 0.020) (Figure 2(D)). Comparison of survival outcomes between the PORT and non-PORT groups in the entire cohort (A and B) and PSM cohort (C and D). Abbreviations: PSM = propensity-score matched; PORT = postoperative radiotherapy.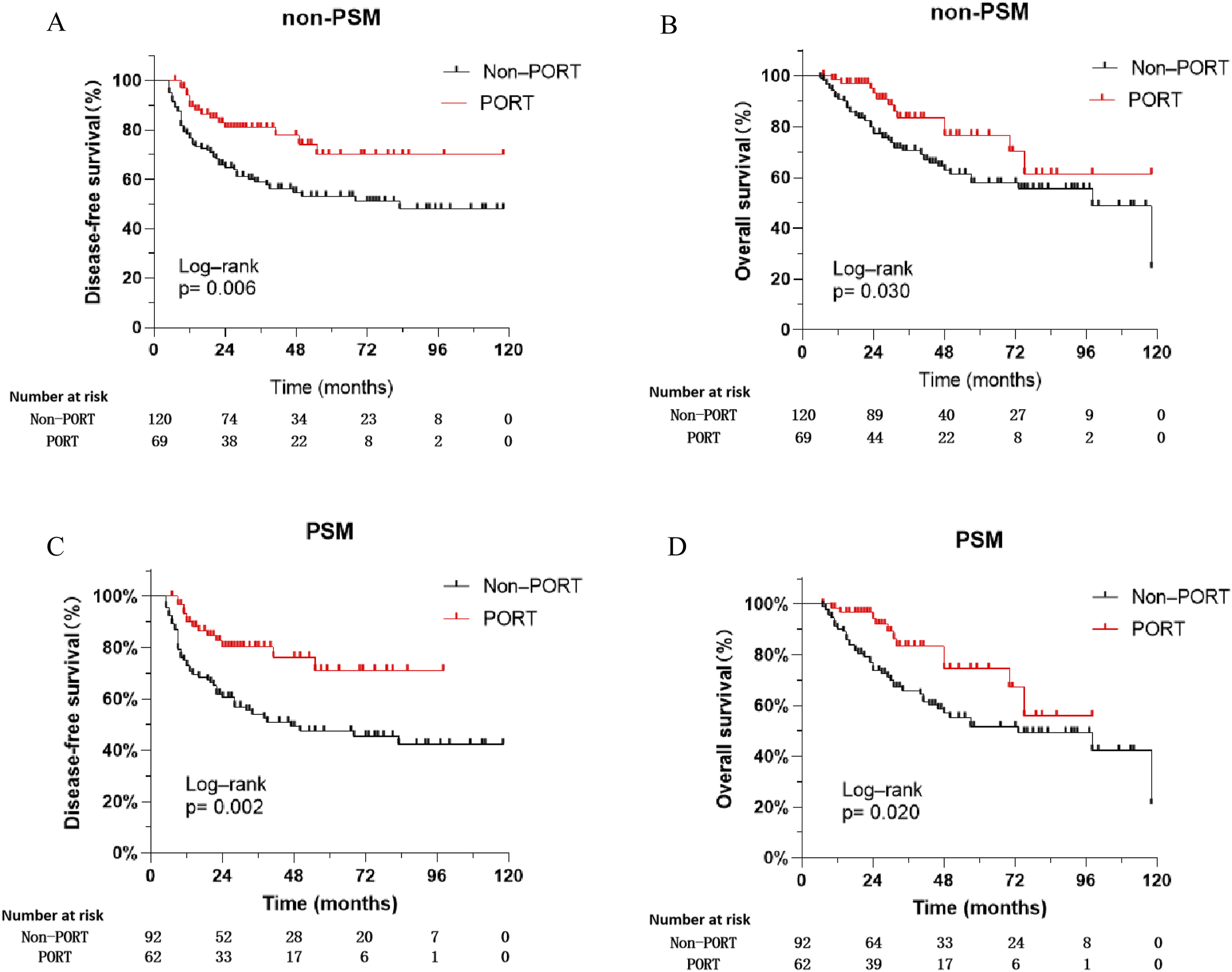
Prognostic Factors of DFS and OS
Univariate and Multivariate Analyses of Overall Survival and Progression-free Survival in the PSM Cohort.
Discussion
There has been ongoing debate regarding the use of PORT for early to mid-stage ESCC patients after R0 resection and some previous randomized studies on PORT found no improvement in survival rates.7,21-24 However, these studies have some limitations, such as patient enrollment including early-stage cancer, 22 variations in the scope, dosage, and techniques of PORT, 23 and the occurrence of severe complications. 24 In recent years, large-scale retrospective studies from both domestic and international sources have indicated that PORT may improve survival rates in patients with pathological lymph node metastasis.25-29 Nevertheless, the clinical value of PORT has not been widely accepted due to the lack of large-scale randomized controlled trials. Further exploration is needed to determine the optimal patient selection and target volume delineation. In the current study, patients with occult RLNM only were included and PORT using a small-T field was found to be associated with improved survival, warranting future validation.
The most common sites of locoregional recurrence in surgery-treated ESCC patients are in the bilateral supraclavicular and upper mediastinal regions, 30 suggesting potential clinical value of small T-field PORT in selected patients. Studies have shown that the rate of local or regional recurrence after surgery for esophageal cancer ranges from 23.8% to 58.0%,31-35 with the most common sites of recurrence being lymph nodes in the bilateral supraclavicular and upper mediastinal regions, including those near the recurrent laryngeal nerves. 28 In the current study, more than half of the patients in the non-PORT group developed their initial recurrent disease only in the supraclavicular and upper mediastinal regions, consistent with the previous studies. In addition, Studies by Kato et al 36 and Ma et al 15 have shown that lymph node metastasis near the recurrent laryngeal nerves is significantly associated with overall survival and disease-free survival rates (P < 0.001). Similarly, another study by Ye et al 16 found that patients with metastasis near the recurrent laryngeal nerves had a significantly lower 3-year survival rate than patients with metastasis at other lymph node sites (29.3% vs 58.2%, P < 0.050). Taken together, all of these studies provided preliminary rationale for PORT in R0 resected ESCC patients with occult RLNM.
Furthermore, various studies have found that PORT targeting the above-mentioned high-risk areas could improve survival outcomes. Chen et al 25 found that PORT was associated with a lower recurrence rate in patients with tumors located in the supraclavicular region and upper mediastinum. Zhao et al 37 found that postoperative radiotherapy using small T-shaped field for esophageal cancer showed advantages in terms of local recurrence rates in mediastinal lymph nodes, and this irradiation range was deemed safe and effective. In the current study, PORT covering the bilateral supraclavicular and upper mediastinal regions with lower border at the manubrium sterni (small T-field), significantly decreased the incidence of locoregional recurrence and improved survival outcomes in ESCC patients with occult RLNM only after R0 resection, which was generally consistent with previous studies. Given the high risk of local recurrence and its impact on prognosis, RLNM presented as a potential biomarker for patient selection for PORT and the current study provided preliminary evidence supporting the survival benefit of PORT in patients with occult RLNM.
The target volume delineation in ESCC patients receiving PORT is still controversial. The choice of appropriate radiation therapy area varies in different studies, which is crucial for treatment efficacy and toxicity. Currently, there are typically two types of target volume in PORT, including large-field irradiation and small T-field irradiation. Studies38,39 have selected wide-range radiation therapy (from the entrance of the esophagus to the celiac trunk) for patients with postoperative lymph node metastasis of esophageal cancer, with a maximum dose of up to 45 Gy while ensuring that normal tissue is not overexposed. However, it is difficult to achieve the goal of eradication of latent metastatic lesions. 40 In this study, small T-field irradiation was used and the radiation dose could reach 50.4 Gy, which may help eliminate micro-metastases and further improve the local control rate and long-term survival.
The clinical value of adjuvant systemic therapy is also undetermined. A study conducted in Japan in 2003 41 suggested that adjuvant chemotherapy after surgery can improve the DFS for selected patients with ESCC, but it does not significantly improve OS. However, the US guidelines recommend for esophageal adenocarcinoma a neoadjuvant treatment similar to the gastric one based on the triplet fluorouracil plus leucovorin, oxaliplatin and docetaxel.42,43 This neoadjuvant treatment improves the prognosis of patients with esophageal adenocarcinoma. In 2021, a large-scale Phase III randomized controlled trial (Checkmate 577 study) 44 revealed the value of adjuvant immunotherapy for esophageal cancer. In patients with locally advanced esophageal or gastroesophageal junction adenocarcinoma who underwent neoadjuvant concurrent chemoradiotherapy followed by R0 resection with residual tumors (non-pCR), adjuvant nivolumab treatment for one year significantly extended both DFS and OS. However, the patients included in this study were clinical early-to-mid stage ESCC and direct surgery was performed, without adopting the neoadjuvant treatment modality. Therefore, the treatment modality used in the Checkmate 577 study is not suitable for patients in this study.
In addition, in terms of esophageal tumor location, multivariate analysis showed that the prognosis of mid-thoracic esophageal cancer was better than that of upper thoracic esophageal cancer. This may be related to factors such as anatomical location, the scope and extent of lymph node dissection, and surgical approach. 25 Lymph node dissection in the lower neck and upper mediastinum is technically difficult because these regions have complex anatomical structures, are rich in nerves and lymphatic vessels, and are adjacent to large blood vessels and vital organs. Incomplete dissection in these regions may leave subclinical lesions. In contrast, the middle and lower mediastinum and upper abdomen can be well exposed, and lymph node dissection is relatively more thorough. A multicenter study 45 indicated that patients with esophageal cancer, whose primary tumors were located in the lower and middle segments, had a higher survival rate compared to those with primary tumors located in the cervical segment of the esophagus (P = 0.013).
This study has several limitations. First, this retrospective, single-center study could not avoid selection bias, although it has been corrected using COX regression and PSM. Second, the safety profile of PORT could not be accurately evaluated due to difficulties in data gathering. Future studies with prospective design and larger sample size are warranted.
Conclusion
In ESCC patients with occult RLNM only after R0 resection, PORT using a small T-field radiation was associated with improve survival, warranting future validation.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.