
Abstract
Background
Treatment for parameningeal rhabdomyosarcoma (PM-RMS) has been a challenge since local control is difficult. The goal of this study was to analyse the impact of different local treatment approaches on childhood PM-RMS patients and help dispel the doubt that whether secondary radical surgery (SRS) should be encouraged in the management of PM-RMS.
Methods
A total of 17 children with PM-RMS who received unified systemic chemotherapy and individualized local therapy such as radiotherapy (RT) and/or SRS were included in this retrospective study. The overall survival (OS) and event free survival (EFS) were compared between groups adopting different local strategies.
Results
The 3-year OS and EFS of our PM-RMS patients was 75.5% and 56.5% respectively. The OS and EFS of patients who received SRS were both significantly lower than that of the non-SRS group (3-year OS: 50.0% vs 90.0%, P = .031; 3-year EFS: 33.3% vs 60.6%, P = .020). The OS and EFS of the patients who received RT was higher than that of the patients of the non-RT group (3-year OS: 85.6% vs 0%, P = .001; 3-year EFS: 64.0% vs 0%, P = .011).
Conclusion
This study illustrates that SRS was associated with poor prognosis of PM-RMS and should not be routinely performed. Optimized RT strategies along with more intensive chemotherapy may be alternative options to improve the survival of patients with PM-RMS. Multi-center, large sample and prospective studies are needed to further validate these findings.
Introduction
Rhabdomyosarcoma (RMS) is the most common soft tissue sarcoma of children and accounts for 3.5 to 4.5% of all childhood tumors.1,2 RMS may occur at any anatomical position since it originates from immature striated muscle which exists anywhere in human body. 1 After decades of efforts, clinicians have developed relatively mature multimodal therapeutic protocols to increase the 5-year overall survival (OS) rate of children with RMS from 25% before 1970 to nearly 80%∼90% nowadays.3,4 However, patients with high-risk factors such as unfavorable locations could not share the equal fortune. Parameningeal rhabdomyosarcoma (PM-RMS) is a specific group of RMS arising from parameningeal regions including nasal cavity, paranasal sinuses, infratemporal fossa, nasopharynx, or mastoid/middle ear. PM-RMS accounts for about 20% of all RMS cases and outcome of these patients is worse than those of other locations. 5 The reported 5-year OS of PM-RMS varied from 45.7% to 73%.6,7 Disease recurrence at the primary site and distant metastases are the leading cause of death in PM-RMS.6,8
It is reported that about 37.5% of PM-RMS patients may experience local failure (LF) 9 and the estimated 3-year survival after LF was 17%. 10 Local treatment plays an important role in controlling local lesions and preventing recurrence of RMS. However, the optimal local treatment strategy for PM-RMS patients is still under debate. In regard of the anatomic complexity and concerns about functional and cosmetic impairments, complete resection with negative margins is often difficult to achieved in the initial surgery approach. Therefore a second-look operation is available if residual disease is suspected after induction chemotherapy. 11 At present, there is limited data for secondary radical surgery (SRS) in PM-RMS.
The aim of this study was to analyse the impact of different local treatment approaches on childhood PM-RMS patients and help dispel the doubt that whether SRS should be encouraged in the management of PM-RMS.
Methods
Study Population and Setting
We retrospectively reviewed the records of patients with childhood rhabdomyosarcoma at the pediatric department of the Sun Yat-sen Memorial Hospital from January 2013 to December 2018. The study was approved by the ethics committee of Sun Yat-sen Memorial Hospital. The reporting of this study conforms to STROBE guidelines. 12
Risk Classification of Rhabdomyosarcoma.

LR, low-risk; IR, intermediate-risk; HR, high-risk; ERMS: Embryonal rhabdomyosarcoma, ARMS: Alveolar rhabdomyosarcoma.
RMS-CQ-2009 Protocol.


Chemotherapy
All patients received systemic chemotherapy (CT). CT was always conducted immediately after primary surgery or as an upfront treatment in inoperable or metastatic patients. CT regimens consisted of vincristine (VCR, abbreviated as V), actinomycin D (ACTD, abbreviated as A) and cyclophosphamide (CTX, abbreviated as C). The protocol was composed of alternating VAC, V, A, VA, VC regimen (Table 2), in which ACTD was omitted during radiotherapy. Treatment courses varied from 12 weeks to 41 weeks according to different RMS risk groups.
Radiotherapy
Radiotherapy (RT) was not required for low-risk group embryonic RMS subjects with no residual tumors (Group I). For patients with residual tumor (group II and Group III), radiotherapy was initiated in the 3rd week (low-risk group A), the 5th week (low-risk group A), the 12th week (intermediate-risk and high-risk group A) and the 15th week (high-risk group B) respectively. Emergency radiotherapy was performed in those patients whose meningeal tumor directly invaded the brain tissue and oppressed the cranial nerve palsy or spinal cord.
Surgery
Complete surgical excision was initially conducted if it would not cause major functional or cosmetic deficits. In cases that could not be completely resected, initial biopsy followed by chemotherapy and definitive local control measures was carried out. The time point of SRS was arranged after the 12th week or the 24th week of chemotherapy. SRS was defined as extensive excision of primary tumor along with the lymph nodes in the regional lymphatic drainage area after chemotherapy. Rapid biopsies were performed intraoperatively to achieve negative margins as far as possible.
Statistical Analysis
EFS was defined as the time from the date of initial treatment to the first occurrence of disease progression, disease relapse, or death. For those not experiencing one of these events, EFS was censored at last contact. Estimates of OS and EFS as time-to-event distributions were calculated using the Kaplan-Meier method, and distributions were compared using log-rank tests. A P value of <.05 was considered statistically significant.
Results
Patient Characteristics
Characteristics of the 17 Patients With Parameningeal Rhabdomyosarcoma.
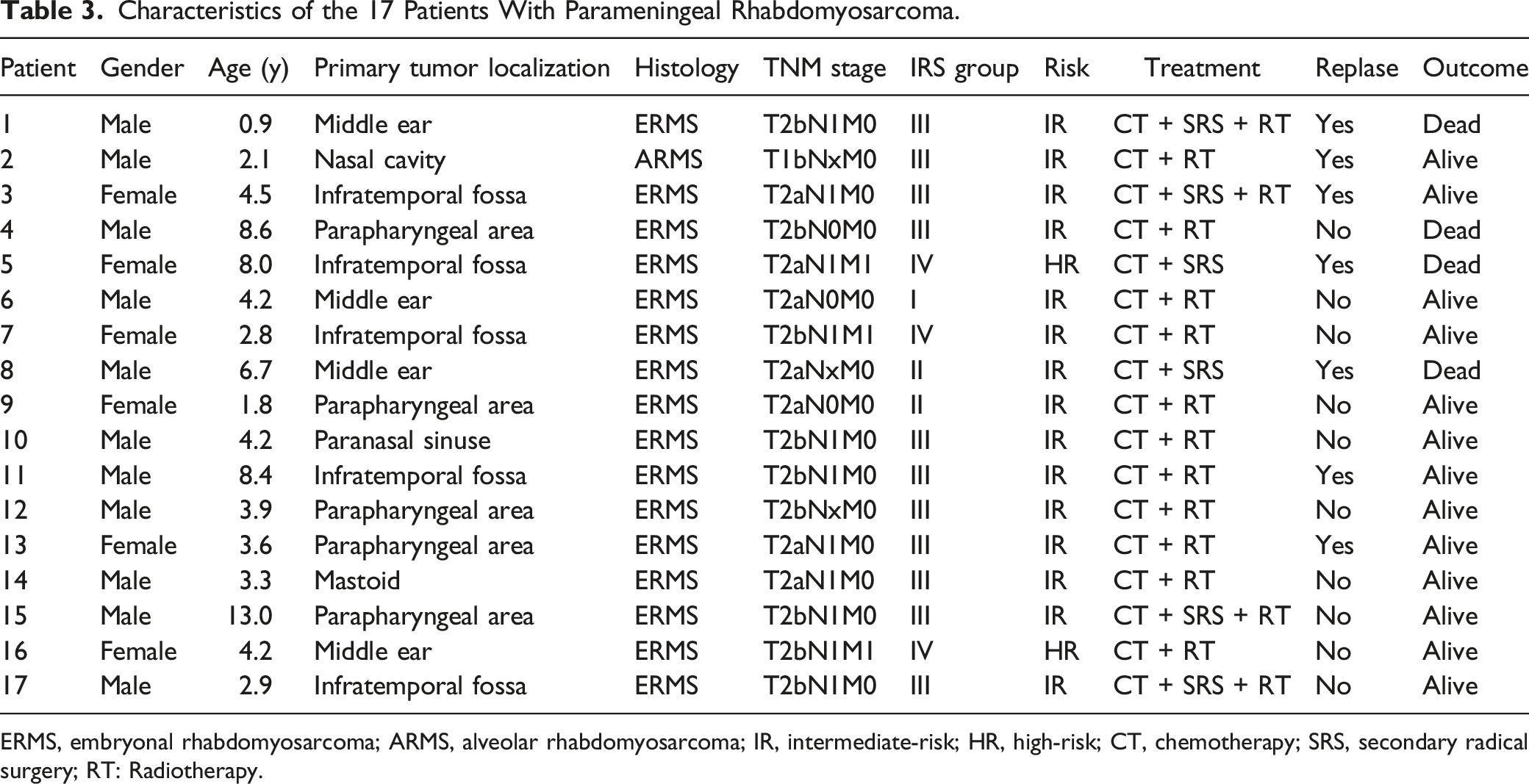
ERMS, embryonal rhabdomyosarcoma; ARMS, alveolar rhabdomyosarcoma; IR, intermediate-risk; HR, high-risk; CT, chemotherapy; SRS, secondary radical surgery; RT: Radiotherapy.
Treatment Outcome
Prognosis of Different Treatments.


The survival curve of PM-RMS patients. (A) OS of children with different treatments; (B) EFS of children with different treatments; CT: Chemotherapy; SRS: Secondary radical surgery; RT: Radiotherapy.
Discussion
RMS is a highly heterogeneous tumor with diverse primary sites, differing pathologic classifications, complex clinical features and varying outcomes. Compared to other locations, PM-RMS is endowed with more unfavorable features concerned with poor prognosis. This is attributed to not only delayed diagnosis, as PM-RMS patients can be asymptomatic and manifest with less distinctive symptoms, but also complexity of its anatomy, proximity to the cranial cavity and potential dissemination via the cerebrospinal fluid (CSF). In our research, the 3-year OS and EFS was 75.5% and 56.5% respectively. This result is similar to that in the IRS studies and the Associazione Italiana di Ematologiae Oncologia Pediatrica (AIEOP) studies.14,15 There were many factors that affected the prognosis of PM-RMS, including treatment programs, stage, primary site, age, etc. Rahman, H.A., et al claimed that late presentation and advanced local disease decreased OS and EFS, with a significant difference of the 3-year OS in metastatic patients and non-metastatic patients (35.8% vs 65.9%). 16 The IRS-II through -IV studies showed that the 5-year OS of patients with tumors in paranasal sinuses or pterygopalatine/infratemporal fossa with meningeal involvement was 57% while OS in those with tumors the middle ear/mastoid, nasopharynx/nasal cavity, or parapharyngeal space without meningeal involvement was 92%. 14 They also identified age 1-9 years at diagnosis as independent favorable factors. However, it’s reported histology did not predict outcome for PM-RMS independently.14,15,17 In our cohort, the majority (82.3%) of patients did not have distant metastasis at diagnosis and the median age was 4.2 years old, 88.2% of them within the range of 1-9 years old. Only 29.4% of the primary tumors located in the unfavorable parameningeal sites. Without regard to the differences in treatment options, the above characteristics may contribute to the relatively better outcome in our study.
Local treatment is essential for RMS management. Since complete resection of the tumor is closely associated with the clinical stage and prognosis of the disease, 18 radical surgery with negative margins if possible is advisable for RMS. There were numerous researchers recommended SRS providing residual diseases was suspected after induction chemotherapy,6,15,19–22 but limited researches focused on the effect of SRS in childhood PM-RMS patients. In our study, stratified analysis demonstrated that the survival rate of children with PM-RMS treated with SRS was significantly lower than that of those without SRS. This could be attributed to the difficulties to obtain disease-negative margin in parameningeal areas especially for pediatric patients and increased risks of metastasis by iatrogenic spreading. In a recent study, the recurrence and metastasis rates of pediatric patients with RMS who received combined skull-maxillofacial resection reached 43.8%, with 31.3% of mortality. 23 On the other hand, SRS in itself may not contribute to prolong the survival of RMS patients. Result from COG D9803 study showed that the local control outcome of group III RMS patients with tumors at select anatomic sites (bladder dome, extremity and trunk) who received secondary excision with reduced radiation dose was similar to historic results with radiation therapy alone. 21 Another study concerning nonmetastatic adult head and neck RMS also demonstrated SRS did not have significant impact on OS. 24 Therefore we suggest SRS should not be routinely performed in pediatric patients with PM-RMS. Surgical resection must be prudently discussed by a multidisciplinary team and cautiously applied in selective cases such as recurrent disease salvage and small tumors without dural involvement. 25
RT is another effective means of local treatment for RMS. Postoperative RT is recommended for patients with rhabdomyosarcoma having microscopic disease. 26 It’s believed that cure of PM-RMS remains unlikely without systematic use of RT. 7 Both data from COG and International Society of Pediatric Oncology (SIOP) studies revealed that omission or delay of RT significantly increased local recurrence rate even in infant and children younger than 3 years old.7,26,27 Results of our research represented that the survival rate of patients treated with RT was significantly higher than those without radiotherapy, confirming the importance of RT for the treatment of PM-RMS.5,28 Despite concerns about the acute toxicity and late effects of its use in young children, progressive radiotherapy technologies such as intensity-modulated radiotherapy (IMRT) and proton radiotherapy (PT) are well-tolerated with mild-moderate toxicity.29,30 Specifically, PT has apparent radiation physical advantages for pediatric PM-RMS patients owing to superior normal tissue sparing with equivalent tumor control rate compared to traditional photon radiotherapy.30–33
Treatment for RMS is a joint effort involving systemic chemotherapy and local therapy. Systemic chemotherapy has significantly increased the OS of children with RMS in the past decades. It’s reported that that poor response to induction chemotherapy was associated with an increased risk of local failure in PM-RMS. 9 There is still a need to explore new effective treatments and protocols for patients with PM-RMS. Several studies have shown intensive induction chemotherapy improved local control rates as well as survival rates and may allow for a response-based radiotherapy approach which could decrease treatment-related morbidity.34,35 Experience from a tertiary cancer care center from India revealed that patients with PM-RMS who received >20 weeks of intended chemotherapy schedule and had complete response to first-line treatment were found to have superior failure-free survival. 36 Recently the Children’s Oncology Group (COG) reported a dose-intensive multiagent regimen, including dose-compressed cycles of ifosfamide/etoposide and vincristine/doxorubicin/cyclophosphamide, and irinotecan could improve outcome of patients with high-risk RMS. 37 Thus intensive chemotherapy with new agent combinations based on standard (VAC) regimen may be recommended in PM-RMS patients.
There are several limitations to this preliminary study, with the most prominent limitation being sample size. We are also aware of the limitations in the monocentric sample source. Though surgery operations of these cases were performed by experienced neurosurgical and maxillofacial surgeons, whose professions kept in an advanced level of China, multi-center, large sample and prospective studies are needed to further verify these results.
Conclusion
The present study suggested that SRS should not be routinely performed in PM-RMS. Optimized RT strategies along with more intensive chemotherapy may be alternative options to improve the survival of patients with PM-RMS. Multi-center, large sample and prospective studies are needed to further validate these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grant SYS-C-202007 from Sun Yat-sen Clinical Research Cultivating Program of Sun Yat-sen Memorial Hospital.
Ethical Statement
Data Availability Statement
Data is available upon request at the corresponding author.