
Abstract
Introduction
Human papillomavirus (HPV) infection is a common sexually transmitted infection often associated with cancer development. This study aimed to estimate the prevalence of HPV in women receiving care at the AUNA healthcare network in Peru.
Methods
We conducted an observational, descriptive, cross-sectional, retrospective study. A de-identified database of HPV-positive women who underwent the BD Onclarity™ HPV Assay between December 2018 and December 2021 at Auna clinics was analyzed. The database contained information regarding age, city, and HPV type. High-risk HPV types were analyzed individually (16, 18, 31, 45, 51, 52) and pooled [P1 (33, 58), P2 (56,59,66), and P3 (35,39,68)]. The study was approved by an independent research ethics committee in Peru.
Results
Of 68,714 women included in the study, the HPV prevalence was 14.21% (N = 9765, 95%CI:13.95%–14.47%). The highest prevalence was detected in Piura (16.85%, 95%CI:15.40%–18.38%), where HPV-51, HPV-52, HPV-P1, HPV-P2, and HPV-P3 were most common compared to other Peruvian cities included in the study. In Arequipa, the prevalence was the lowest (13.58%, 95%CI:12.38%–14.85%), but the percentage prevalence of HPV-16 was the highest compared to other cities. The prevalence of multiple HPV infections was 2.88% (N = 1981, 95%CI:2.76%–3.01%), with most of them co-presenting two types of HPV (N = 1522). The most frequent co-occurrences were P2 and P3, P2 and 52, and P2 and 16. Among HPV-positive women, the mean age was 41.31 years (±9.48) and 25.29% were in the 31–35 years group. HPV-P2 was the most frequent in all age groups except in the 65–72 years group, where HPV-P3 was the most common.
Conclusion
HPV prevalence was shown to be highest in Piura, with the most prevalent types being HPV-16, HPV-52, and HPV-P2 (HPV-56, -59, -66). HPV infection was found to be more frequent among women in the 31–35 years age group.
Background
Human papillomavirus (HPV) is one of the most common sexually transmitted infections worldwide. 1 In fact, most sexually active individuals are likely to acquire HPV at some point in their lives, 2 usually without any symptoms and with infections resolving on their own without treatment. 3 However, persistent infections can lead to different health issues. 4
HPV encloses over 200 types of viral strains, but only some of them have oncogenic potential. 1 This high-risk HPV group includes strains 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68. Although HPV has been mostly associated with cervical cancer, it is also strongly linked with anal, vaginal, vulvar, penile, and oropharyngeal cancers. 5 Furthermore, between 4.5%–5.2% of all cancers diagnosed worldwide could be attributed to HPV infections.5-8
Even though HPV vaccination has been proven as an effective method to prevent cancers associated with this viral infection, 6 cervical cancer is still the fourth most common cancer among women worldwide, being most prevalent and fatal in low- and middle-income countries. In Peru, the age-standardized incidence and mortality rates are 23.9 and 12.1 per 100.000, respectively. In 2022, 4809 Peruvian women were diagnosed and 2545 died from cervical cancer, becoming the second most common neoplasia, among women, and the leading cause of death. 9 Remarkably, HPV has been found in 99.7% of cervical cancers. 10
The prevalence of HPV varies depending on the geographical region, development index, ethnicity, lifestyle, sex, and age, among other factors.11-14 For instance, the highest prevalence has been reported in Sub-Saharan Africa (24.0%), followed by Eastern Europe (21.4%), and Latin America (16.1%). 14 Similarly, in Peru, the HPV prevalence differs significantly within the country, ranging from 8.4% to 43.9%,15-18 depending on geographical site, HPV type, method of detection and age.
AUNA is a private healthcare network with hospitals and ambulatory medical centers in different cities in Peru, Colombia and Mexico. In Peru, Auna has a presence in Lima, Arequipa, Trujillo, Chiclayo and Piura, all five of these among the seven most populated cities in the country. In addition, Lima is the capital city of Peru, while Piura, Chiclayo and Trujillo are located in the northern region and Arequipa is located in the south of Peru.
In order to develop and implement more effective health policies to reduce the burden of HPV infections and cervical cancer, analysis of the HPV prevalence is imperative. Thus, we conducted a study aimed at estimating the prevalence of high-risk HPV strains within the AUNA network, segregating the results by HPV type, age group and concomitant infections.
Methods
Study Design and Population
We conducted an observational, descriptive, cross-sectional, retrospective study, by analysis of a de-identified database of HPV-positive women who underwent molecular HPV testing at AUNA hospitals located in five geographical regions, Piura (Piura), Lambayeque (Chiclayo), La Libertad (Trujillo), Lima (Lima) and Arequipa (Arequipa), from December 2018 to December 2021. The de-identified data was obtained from the pathology department record system and included age, location, and HPV-type. Patients under 16 years with cervical lesions were included. In cases where more than one diagnostic test was done during the study period, only the first result was included.
The reporting of this study aligns with the STROBE guidelines. 19
HPV Testing
Cervical samples were collected using a cytobrush and sent to the central laboratory of Auna in Lima. HPV genotyping was done using the BD Onclarity™ HPV Assay. This qualitative assay employs real-time PCR and fluorescent probe technology to identify the E6 and E7 DNA regions of the HPV genome. Results are reported as either presence or absence of high-risk HPV, individually for the following types: 16, 18, 31, 45, 51 and 52, or pooled: P1 (33, 58), P2 (56,59,66), and P3 (35,39,68). A cellular β-globin control is included to differentiate HPV-negative samples from those that do not present an HPV signal due to insufficient cell mass in the sample. Testing was conducted using the BD Viper™ LT system following the manufacturer’s instructions.
Statistical Analysis
A descriptive analysis of the collected information was performed, and absolute frequencies and percentages were estimated. To calculate the HPV prevalence, the pathology department provided the total number of women tested within the study period in each clinic. The 95% confidence intervals for HPV prevalence were calculated using the Clopper–Pearson interval method. The analysis and plots were performed with the R Studio Software (2023.12.1- 402 version; RStudio PBC, Boston, MA, USA).
Ethical Considerations
This study was approved by the Ethics Research Committee of the Universidad Privada San Juan Bautista (N°1142-2024-CIEI-UPSJB) located in Lima, Peru, in July of 2024.
Results
HPV Prevalence
A total of 68,714 women, who underwent molecular HPV testing, were evaluated during the study period. Most of them were located in Lima (N = 56,628, 82.4%), followed by La Libertad (N = 3699, 5.4%), Arequipa (N = 3042, 4.4%), Lambayeque (N = 2859, 4.2%) and Piura (N = 2486, 3.6%). HPV global prevalence was 14.21% (N = 9765, 95% CI: 13.95% – 14.47%). The highest prevalence was identified in Piura, where 16.85% were positive (N = 419, 95%CI: 15.40%–18.38%), while the lowest prevalence was 13.58%, in Arequipa (N = 413, 95%CI: 12.38% – 14.85%) (Figure 1). HPV prevalence by department in which AUNA clinics are located. The figure shows the prevalence of HPV and HPV type, according to the geographical distribution of the molecular HPV testing by departments. N: Number of HPV positive women. %: Prevalence. 95% CI: 95% confidence interval.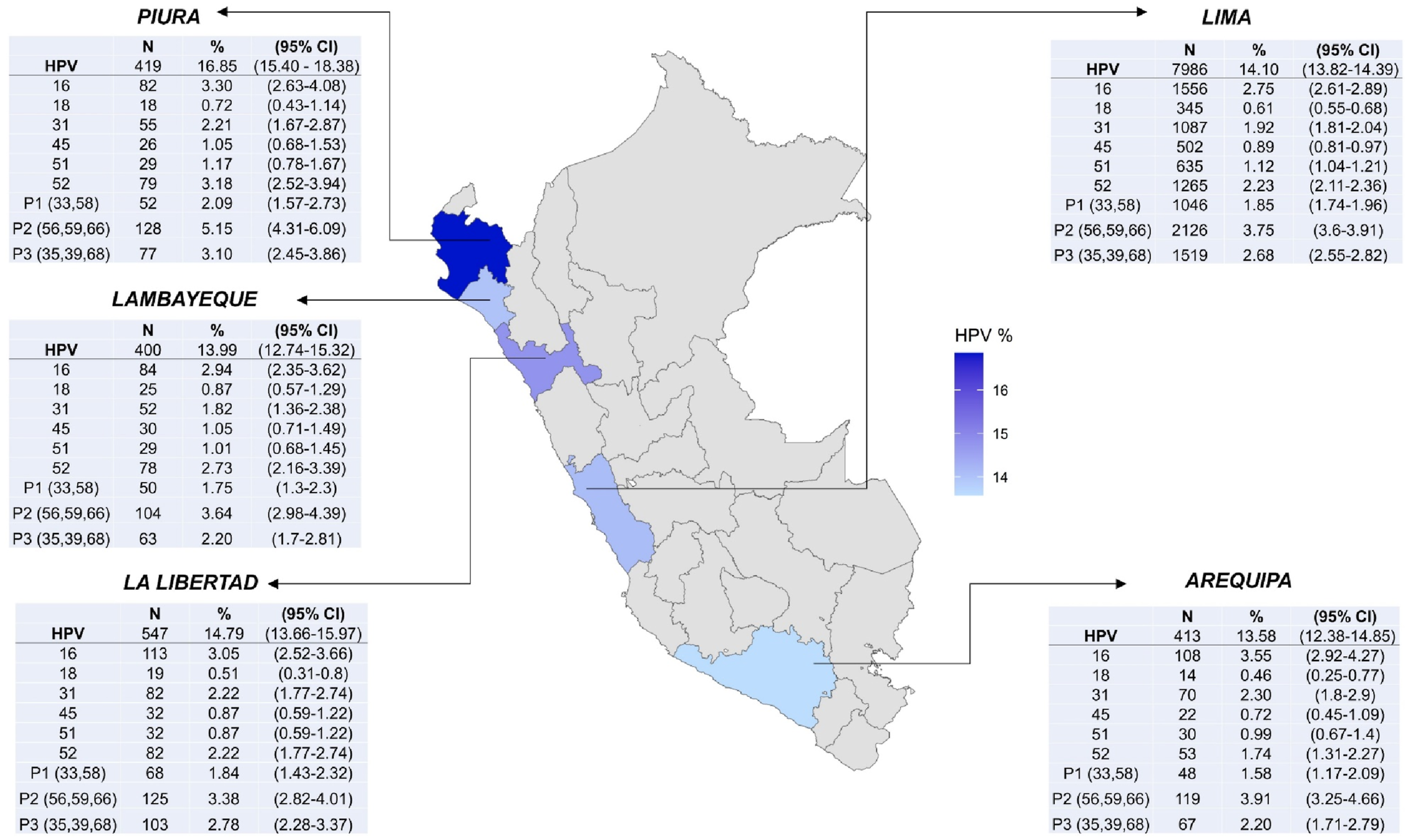
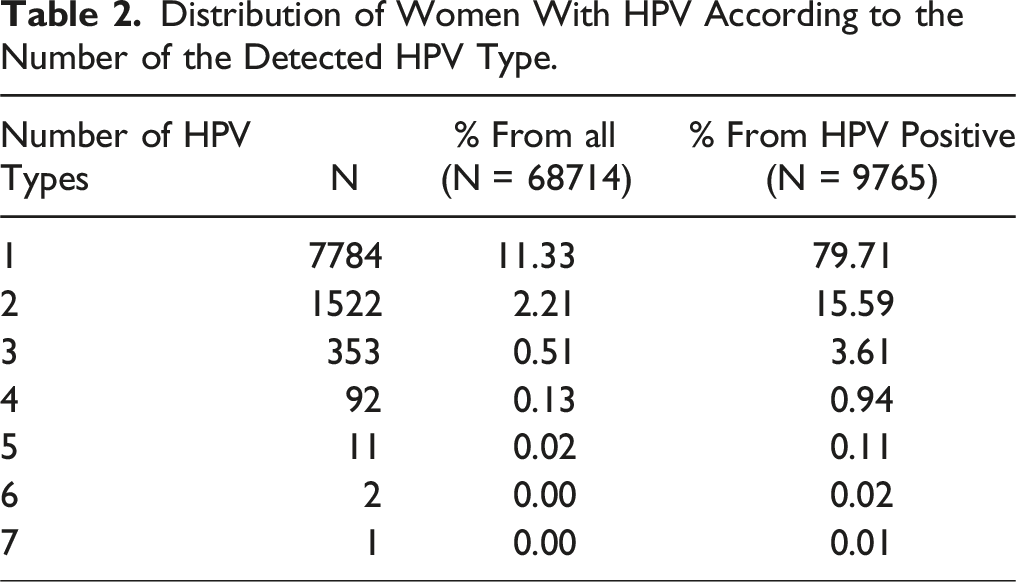
The most prevalent HPV types were HPV-P2 (56,59, 66) (3.79%, 95%CI: 3.65% - 3.93%), HPV-16 (2.83%, 95%CI: 2.70% – 2.95%) and HPV-52 (2.27%, 95%CI: 2.16% – 2.38%) (Figure 2). Furthermore, 2.88% of women were positive for more than one HPV type (N = 1981, 95%CI: 2.76%–3.01%). Prevalence of HPV types. The figure shows the prevalence of each HPV type, in the evaluated population. N: Number of HPV positive women. %: Prevalence. 95% CI: 95% confidence interval.
Regarding the prevalence of HPV types by geographic region where AUNA hospitals are located, HPV-16 was remarkably predominant in Arequipa (3.55%, 95%CI: 2.92 – 4.27), followed by HPV-31 (2.30%, 95%CI: 1.8 – 2.9). On the other hand, HPV- positive women tested in Piura showed a higher prevalence of HPV-51, HPV-52, HPV-P1, HPV-P2 and HPV-P3 compared to other regions (Figure 1).
HPV Type Distribution in HPV- Positive Women
Distribution of the Frequency of HPV Among Positive Women According to Type and Age Group.

The average age of HPV-positive women was 41.31 years (±9.48); 25.29% of them were in the 31–35 years age group. In almost all age groups, HPV-16 was the most frequent type, except for the 21–25 and the 65–72 years age groups, where HPV-52 was the most common. With respect to pooled detection, P2 (56,59, 66) was the most predominant group among women between 16 and 65 years of age, while P3 (35,39, 68) was the most prevalent in the 65–72 age group (Table 1).
Multiple HPV Infections
Distribution of Women With HPV According to the Number of the Detected HPV Type.

Frequency of concurrent HPV types. The figure shows the combinations for two types of HPV and the percentage of women that tested positive for each combination. The percentages are estimated from de total of patients with two types of HPV (N = 1522).
Discussion
Since HPV is still one of the most prevalent sexually transmitted infections and the cause of some types of cancer, especially cervical cancer, unceasing surveillance is an essential step for early detection and control. We present in this study the largest cohort of Peruvian women screened for HPV by molecular testing. Here, we estimated the prevalence of high-risk HPV in women who come to the AUNA network for health care in Peru.
In 2021, the Peruvian Ministry of Health (MINSA) inaugurated the first molecular laboratory for HPV detection. 20 Since then, molecular screening has been made available in 14 regions of Peru (out of 24), including Lima (Lima and Callao), Junín, Loreto, Arequipa, Ayacucho, Cajamarca, La Libertad, Lambayeque, Cusco, Piura, Ica, Tacna, San Martín and Ancash. 21 According to MINSA, in 2022 alone, more than 600,000 25-64-year-old women were tested. 22 However, HPV prevalence has not been reported yet.
Comparison of HPV Prevalence in Our Study Population Vs Prevalence Reported in Other LATAM Countries.

aMeta-analysis.
Remarkably, a higher prevalence was observed in Piura, focused on HPV-51, HPV-52 and the three types of pooled-HPV strains. In contrast, in other regions, HPV-16 and HPV-31 were the most frequent types. In Peru, it is well known that the existence of geographical, cultural, infrastructural and socioeconomic barriers affects the screening and evolution of some health conditions, including HPV infections. Taking into consideration that our study population belongs mostly to socioeconomic levels A and B (according with the Asociación Peruana de Empresas de Inteligencia de Mercados classification 26 and that these groups of patients have access to HPV-vaccination and well-implemented health facilities, 27 cultural and personal barriers may explain the increased prevalence in Piura. For instance, Requena et al have reported that 100% of women with abnormal cytology cared for at a public hospital in Piura were not vaccinated. Moreover, 93.3% did not have a previous history of molecular HPV screening, 55.0% had only one or two previous Pap smear controls, and the median age for starting Pap smears was 42.97 years (±12.18). 28 Fear and shame to undergo gynecological examinations, forgetting to schedule an appointment, and laziness have been identified as associated factors for not adhering to Pap smear controls. 29
Regarding the prevalence by HPV type, HPV-16 and HPV-52 were the most prevalent types, consistent with global data, where 3.2% and 0.9% of women with normal cytology were positive for HPV-16 and HPV-52, respectively. Conversely, HPV-18 was the least frequent in our study. 14 In Peru, a report published in 2023, found that the most prevalent subtypes in women with normal cytology were HPV-16 (5%), HPV-31 (2.6%) and HPV-58 (1.9%), while HPV-16, HPV-52 and HPV-31 were the most prevalent in women with low-grade lesions. In high-grade lesions, HPV-16 and HPV-33 were the most frequent types, whereas in cervical cancer, HPV-16 and HPV-18 were predominant. 30 However, the number of studies included in this analysis was small and the studies themselves were published between 2001 to 2014.
Among the group of HPV-positive women, HPV-16, HPV-52 and HPV-P2 (56,59), were the most frequent types in all age groups, except for women between 65 and 72 years, where HPV-52 and HPV-P3 (HPV-35,39,68) were the most common. Most positive women (71.51%) were between 31 and 50 years old, with the majority clustered in the group of 31-35 years. Similarly, a notable increase in HPV prevalence among women aged 14-19 years, followed by another peak in those aged 30-34 years has been reported. 31 In women with abnormal cytological findings, the prevalence of high-risk HPV was statistically higher in women aged between 35 and 45 years with lower levels of education, multiple pregnancies and childbirths, history of gynecological conditions and those in the premenopausal stage. 32
In our study, around 3% of women presented multiple HPV infections, the majority of which had two types of HPV. This is consistent with previous studies.31,33,34 Although we could not assess associations with age or cytology results, previous studies have shown that multiple HPV infections were more frequent in women between 14 and 25 years and that the prevalence decreased with age. In addition, women with cervical abnormalities showed an increased prevalence of multiple HPV strains, compared to those with normal cytology.31,35 Furthermore, multiple HPV positivity is associated with high viral loads (>3 log HPV copies/105 cell) and with infection persistence. 36
Our study has some limitations. First, the evaluated population might not represent the general Peruvian population, since only women coming to one private health care network were included and most of them are of socioeconomic levels A and B. In addition, it was not possible to estimate the prevalence by age and cytology results, and for some HPV types, only pooled estimates were feasible. Furthermore, important sociodemographic factors that could be associated with such HPV prevalence could not be evaluated given the retrospective nature of this study and because it is not available in the analyzed dataset. Despite this, we have evaluated a large cohort of women from different regions in Peru and found that the prevalence of HPV in women coming for molecular HPV testing at Auna is similar to previous reports, highlighting the need for better strategies for prevention.
Conclusion
HPV prevalence was higher in Piura and the most prevalent types were HPV-16, HPV-52 and HPV-P2 (HPV-56, -59, −66). Arequipa had the lowest HPV prevalence, and there, the HPV-16 type was most prevalent. HPV infection was more frequent among women in the 31-15 years age group. Regarding co-occurrences, HPV-P2 (HPV-56, -59, −66) and HPV-P3 (HPV-35, -39, −68) was the most frequent one in women who presented two different types of HPV.
Our results provide relevant information regarding HPV prevalence according to geographic location and HPV type in Peru and call for improved strategies for HPV prevention and screening.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Auna Ideas and Auna Laboratorio.