
Abstract
Background
Cervical cancer ranks as the fourth most common cancer among women, with 662,301 new cases and 348,874 deaths reported in 2022. The majority of the disease burden occurs in low- and middle-income countries. In Ghana, there were 3072 new cases and 1815 deaths reported in 2022. While human papillomavirus (HPV) infection, a key cause for cervical cancer, resolves in most individuals, it can progress to cancer in some. This has led to research into other factors that may, in conjunction with HPV, increase the risk of cervical cancer progression. Improving knowledge of HPV, risk factors, and screening will be important in reducing the burden of cervical cancer. In this study, we investigate the knowledge on HPV, risk factors, and cervical screening among women in Ghana.
Methods
A hospital-based case-control study was conducted among women aged 18 to 95 years. This involved Ghanaian women diagnosed with cervical cancer and hospital controls. Data were collected using a structured questionnaire, and basic descriptive analyses were performed.
Results
Results from the 206 cases and 230 controls revealed limited knowledge about HPV and its role in cervical cancer development, with minimal disparity between women with (2.4%) and without (6.5%) cervical cancer. The majority of participants lacked awareness of HPV transmission (95.9%), and awareness of HPV vaccination was low (3.5%). Barriers to HPV vaccination included insufficient awareness about HPV, limited access to vaccination centers, and cost concerns. Respondents expressed a preference for educational programs delivered through church, radio, and television channels.
Conclusions
Knowledge of HPV, risk factors, and cervical screening was found to be very low among Ghanaian women. These findings underscore the need for a comprehensive cervical cancer educational initiative within Ghana’s national cervical cancer control policy to mitigate the disease’s impact.
Background
Cervical cancer remains an important global public health issue. It is the fourth most common cancer among women, with 662,301 new cases and 348,874 deaths in 2022. 1 The majority of the burden of the disease occurs in low and middle-income countries (LMICs). In 2022, 117,944 cases were recorded in sub-Saharan Africa with 10,532 in South Africa, 6,938 in Uganda, 10,868 in Tanzania, 13,676 in Nigeria and 8,168 in Ethiopia.2,3 In Ghana, an estimated 3,072 people were diagnosed with cervical cancer in 2022 and 1,815 died from it. 4
Infection with high-risk human papillomavirus (HPV) has been established as the cause of cervical cancer. While HPV infection resolves in most individuals, in others it progresses to cancer. This has led to a search for co-factors that promote persistent high-risk HPV infection. High parity, long-term use of oral contraceptives, cigarette smoking, and immune suppression have been associated with increased progression to cervical cancer.5,6 Specific risk factors have also been documented in some settings such as polygamy and various socio-economic indicators.7,8 In Ghana, the prevalence of HPV has been estimated to range from 10.7% to 63.8%, with other risk factors also showing significant prevalence.9,10
As the cause and associated risk factors of HPV have been established, various methods of prevention have also been proposed. HPV vaccination has been suggested for young adolescents who are yet to be sexually active, along with screening for precancerous lesions in women within the target age group. However, HPV vaccines, which are for sexually transmitted infections, may face acceptance and marketing challenges in certain settings.11-13 Some studies have reported low acceptability of the HPV vaccine in many LMICs, including Ghana.14,15 This may be due to several factors, including the levels of education about HPV and cervical cancer among study participants. 16
Most women diagnosed with cervical cancer in many LMICs present with late-stage disease.17-22 This has been associated with deficiencies in the health system, cultural, or patient-related factors such as a lack of knowledge about the disease.17,23 Improved knowledge of women about the various risk factors of the disease is likely to reduce incidence and mortality rates. The burden of HPV infection and other risk factors for cervical cancer is reported to be high in Ghana. 24 The prevalence of cervical screening has been reported to be between 2.1% to 5.0%.25-27 It is therefore important to assess the level of knowledge of these factors among women in Ghana and determine if this knowledge varies between women with and without cervical cancer. This information is significant in developing more targeted educational programs. A number of studies have assessed the knowledge of cervical cancer in Ghana.28,29 The restriction of study participants to university students and a lack of comparison groups have limited the generalizability of this previous research. The current study evaluates the knowledge of cervical cancer among women with and without cervical cancer at two large hospitals in Ghana.
Material and Methods
Study Setting and Design
The current study was conducted at two hospitals in Ghana: Komfo Anokye Teaching Hospital (KATH) in Kumasi and Korle Bu Teaching Hospital (KBTH) in Accra, Ghana. Women with invasive cervical cancer and control women were recruited from the National Center for Radiotherapy Oncology and Nuclear Medicine and the Department of Obstetrics and Gynecology at both hospitals. The methodology for participant selection was previously outlined in a published study. 30
In brief, cases consisted of newly diagnosed individuals with histologically confirmed invasive cervical cancer who had not yet received treatment for the disease. Control subjects were identified and selected from the Department of Obstetrics and Gynecology without a current or past history of cervical cancer. Eligible participants were aged between 18 and 95 years, had been residents in Ghana for at least 3 years, and had not received HPV vaccination. Trained research assistants conducted interviews with all consenting study subjects during their hospital visits.
Study Instrument and Variables
A structured questionnaire was used to gather data on various indicators including women’s knowledge about HPV. Study subjects were provided with study packages that included an information sheet and a consent form, both available in English and translated into two Ghanaian languages, Twi and Ga. After explaining the study to eligible participants, written informed consent was obtained. Interviews were conducted in consulting rooms. Trained research assistants conducted the interviews in Twi, Ga, or English, depending on the participant’s preference. The current paper was written following the STROBE guidelines. 31
Ethical Consideration
Ethical approval for this study was obtained from the University of Otago Ethics (Health) Committee, Ghana Health Service Ethical Committee (Protocol ID: GHS-ERC: 01/05/14), and the Committee on Human Research, Publication, and Ethics of the Kwame Nkrumah University of Science and Technology (KNUST) and Komfo Anokye Teaching Hospital (KATH), Ghana (CHRPE/AP/661/19).
Data Analysis
All completed questionnaires underwent a thorough review for completeness before being entered into computer files. The data were then imported from Excel into STATA® version 16.1 (STATA Corporation, College Station, TX). Results were summarized using frequencies, percentages, and tables. Given the substantial number of respondents who indicated “do not know” for questions pertaining to knowledge of HPV, HPV vaccines, and cervical cancer, detailed statistical analysis for these variables was limited.
Results
Knowledge and Awareness of HPV Among Women in Ghana.

Abbreviation: HPV-Human papilloma virus, STI-Sexually transmitted infection.
Knowledge and Awareness of HPV Vaccines Among Women in Ghana.

Abbreviation: HPV-human papilloma virus.
Source of Information About HPV Vaccines.

aNews paper, durbar.
Abbreviation: HPV-Human papillomavirus.
Knowledge and Awareness of Cervical Cancer Among Women in Ghana.

Abbreviation: HPV-Human papillomavirus.
About 11.3% of controls believed that a woman needed to have cervical screening after HPV vaccination. Only 18.8% of the controls believed that cervical screening detects changes before they develop into cancer. Overall, there were large proportions of cases and controls who did not have enough knowledge to answer yes or no to the questions posed about cervical screening.
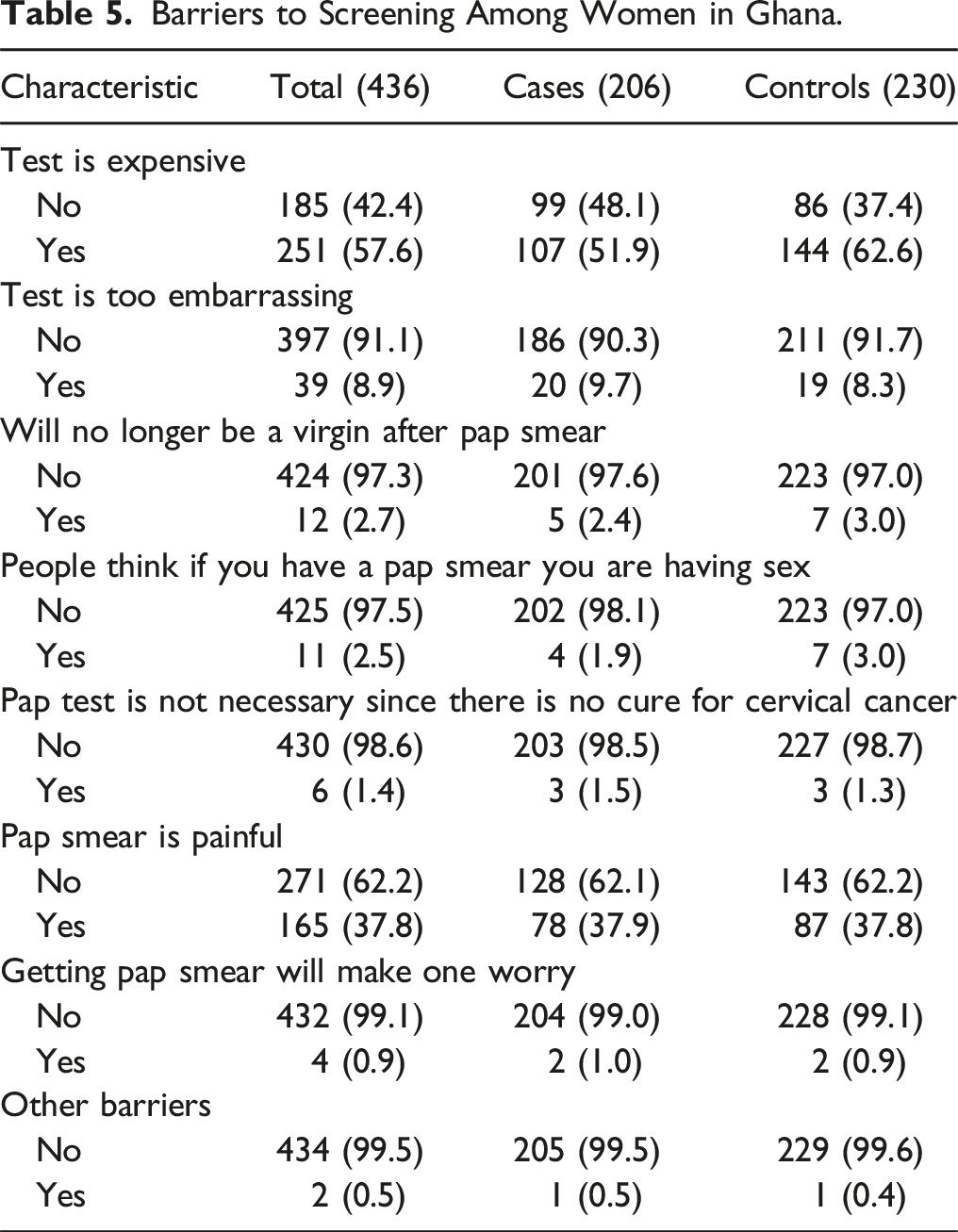
Barriers to Screening Among Women in Ghana.
Discussion
Main Findings
In the current study, both cases and controls demonstrated limited knowledge of HPV infection, cervical screening and cervical cancer. These findings suggest that women in Ghana are largely unaware that HPV infection is the primary cause of cervical cancer or how they can protect themselves against it. The implementation of HPV vaccination and HPV DNA testing for screening may be more successful if women understand the role of HPV infection in the development of cervical cancer.
Comparison with Existing Literature and Possible Explanation
Studies conducted in Ghana and elsewhere have also found women lack knowledge on HPV infection and cervical cancer.19,29,32,33 Only 3.4% of women had heard of HPV vaccines, with a higher percentage of controls than cases knowing that HPV vaccines exist. Accessibility to the HPV vaccine is poor, as there is no systematic vaccination program in place, and it is primarily available in big cities and mostly through private pharmacies. Among the study subjects who were aware of HPV vaccines, most had learned about them through television or healthcare workers. This is in agreement with other studies. 34 However, in a study by Schwendener and colleagues, the main source of information was school health programs and social networks. 35
The low level of knowledge about HPV vaccines highlights the need for enhanced health promotion and education using various media sources, including television. It also underscores the importance of healthcare professionals in educating the public about HPV and its vaccines. With increased resources, a national vaccination program could be implemented, providing women with an understanding of the role of vaccination in reducing the incidence of cervical cancer.
The women reported several barriers to HPV vaccination, including difficulty finding a service provider, the high cost of the vaccine, and the limited availability of clinics offering the vaccination. This is consistent with studies conducted in other settings.36-38 The perceived lack of access to healthcare professionals who can administer the HPV vaccine significantly affects its uptake. As the vaccine is not widely available, physicians may not routinely recommend it to their patients. However, training other healthcare professionals to administer the vaccine could help address this issue. Currently, the cost of a single dose of the vaccine ranges from 900 to 1500 GH¢ ($60-100), which is prohibitively expensive for most women.
Similar to other studies we found knowledge of cervical cancer and cervical screening to be low.18,39-42 Few women had ever had a previous cervical smear in this study. This is supported by other studies conducted in Ghana.25,27,43 The relationship between embarrassment and low uptake of screening has been documented in other settings and cultures.44-46 The male gender of the provider may also be associated with increased embarrassment. 47 The likelihood of screening is also lower among women who believe the test is painful with consequently less tolerance of the screening procedure. 48 This belief may be endorsed or reinforced by women who have previously been screened or by unscreened women. 49 The findings suggest that overcoming practical barriers may be important factors to consider in the quest to increase the uptake of cervical screening. This could include making the service free for women, providing more information about the procedure and addressing public concerns about cervical screening such as pain.
Strength and Limitations
A strength of our study is the comparison of knowledge between women with and without cervical cancer, a comparison that has not been previously conducted in Ghana. The high response rates of 98.6% for cases and 96.6% for controls contribute to the validity of the results. However to the lack of population lists in Ghana from which to select controls for women wh cervical cancer attending hospitals for diagnosis, a population-based case-control study was not feasible. Additionally, it was considered a priori that access to the two hospitals from which the cases were drawn was unlikely to be universally available. To reduce access bias, selecting hospital controls was deemed a suitable alternative. Hospital patients may have greater awareness of certain exposures compared to healthy individuals. In this regard, their comparability to cases in the accuracy of reporting information could potentially reduce recall bias. However, this approach can introduce bias if hospital controls do not represent a random selection of the population from which the cases are drawn. To minimize such bias, controls were recruited exclusively from the Departments of Obstetrics and Gynaecology, specifically from the gynaecology unit. Controls with conditions related to the risk factors of interest, such as other cancers, were excluded to reduce potential confounding. Using all women attending the hospital as the sampling frame for controls was deemed unfeasible due to logistical challenges. The use of self-reported data may have introduced potential recall bias, as cases are more likely to recall past events compared to controls. Additionally, the relatively small sample size limited the statistical power, making detailed subgroup analyses infeasible.
Conclusion
The study revealed that knowledge about HPV, cervical screening, and cervical cancer is significantly low among women in Ghana. This underscores the urgent need for widespread public education on cervical cancer, including its risk factors and the importance of regular cervical screening. Educational initiatives should focus on sexual and reproductive factors related to cervical cancer, while highlighting the benefits of HPV vaccination and routine screenings. Additionally, it is crucial to dispel misconceptions about cervical cancer, such as the belief that effective treatment is unavailable, to reduce disease related mortality. As Ghana prepares to roll out the HPV vaccination program, it is essential to educate the public and address barriers such as cost and accessibility to ensure the program’s success.
Footnotes
Acknowledgments
We would like to thank the participants of this study.
Author contributions
Conceptualization: Yvonne Nartey, Brian Cox, Philip C Hill. Data curation: Yvonne Nartey, Brian Cox, Philip C Hill, Kwabena Amo-Antwi. Formal analysis: Yvonne Nartey, Brian Cox, Philip C Hill, Kwabena Amo-Antwi. Methodology: All authors. Project administration: Yvonne Nartey, Brian Cox, Philip C Hill, Kwabena Amo-Antwi. Writing-original draft: Yvonne Nartey. Writing review and editing: All authors.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received no specific funding for this work. Associate Professor Brian Cox was supported by the Director’s Cancer Research Trust. Funding for HPV DNA testing was provided by the Department of Preventive and Social Medicine.