
Abstract
Introduction
Lung cancer remains the leading cause of cancer-related death in the United States. Low density CT (LDCT) has been shown to reduce mortality in high-risk populations. Recognizing and mitigating gaps in knowledge in early medical training could result in increased utilization of screening CT in high risk-populations.
Methods
An electronic survey was conducted among Internal Medicine (IM) residents at 4 academic programs in the Midwestern United States. A survey was distributed to evaluate knowledge about high-risk populations, mortality benefits, and a comparison in mortality benefits between LDCT and other screening modalities using number needed to screen (NNS). Results: There was a 46.6% (166/360) response rate. Residents correctly answered an average of 2.9/7 (43.1%) questions. PGY-1 (post-graduate year) and PGY-2 residents performed better than PGY-3 (P = .022). Only 1/3 rd of all respondents correctly identified the population needed to be screened. Over 80% of residents thought screening with LDCT had a cancer-specific mortality benefit but were evenly split (except Program 2 residents), on recognizing an all-cause mortality benefit with LDCT, (P = .016). Only 7.7% thought women benefited the most from LDCT. Self-assess and attained knowledge were similar among programs.
Conclusions
LDCT is a noninvasive intervention with a substantial mortality reduction, especially in states with high rates of smoking, and is widely covered by insurers. With average knowledge score less than 50%, this study shows there is a substantial need to increase the knowledge of LCS in IM residency programs.
Introduction
The mortality burden of lung cancer in the United States remains elevated despite reducing smoking rates and better treatments. 1 An initial lung cancer presentation in advanced stages is common due to the asymptomatic nature of most early stage disease. The last decade has seen a substantial increase in lung cancer screening (LCS) centers, stemming from multiple societal guidelines as early as 2013 cataloging low-dose computed tomography (LDCT) as a life-saving intervention in certain populations. 2 However, less than 5% of eligible persons are being screened in the United States as of 2017.3,4 In Canada, 5 pilot feasibility studies are underway for a federal screening program. In the past 5 years, a Europe-wide policy to implement LCS has been developed with a focus on risk stratification, appropriate CT protocols, and smoking cessation. 6 Data from the MILD/NELSON trials have also shown a continuous benefit the longer period of time LCS is implemented. Despite the call for screening, many physicians are unaware of the efficacy of LDCT. Furthermore, LDCT may not be appropriately recommended to high-risk populations seen in primary care clinics, where future primary care physicians (PCPs) are currently training. In 2018, it was estimated that residents may be involved in up to 30% of primary care clinics nationwide. 7
Factors such as early detection, low harm in screening, and trust in the referring physician have shown to affect a patient’s preference for LCS. 8 Physicians were concerned about the effectiveness of the test, the cost to the patient, and the possible harm from subsequent interventions. However, many of them still ordered chest x-rays, which is ineffective at reducing lung cancer mortality. 9 Among internal medicine (IM) residents, knowledge about who the high-risk population appropriate for LCS and the effectiveness of LDCT to reduce mortality have been identified to be major barriers in recommending this measure. 10
In the US Midwest, smoking rates continue to be higher than the national mean. 11 In a recent review of 10 states, LCS rates ranged from 9–17%, including only 10.5% in 2 Midwestern U.S. states. 12 Targeting high-risk populations in these states, recognizing knowledge gaps, and developing curricula to support its prospective preventative health physicians may prove valuable to reduce lung cancer mortality rates. The principal aim of this study is to evaluate LCS knowledge among IM residents from 4 residency programs in the US Midwest, where the total outpatient primary care visits are estimated to be 20 million every year.
Methods
The 2013 USPSTF recommendation rationale was the source material to assess the knowledge base of IM residents. 2 Eligible participants were identified through their respective program’s residency leadership. Eligible participants had to be: a) active IM residents or medicine-pediatrics residents as of March of 2019. These residents were training in programs located in Indiana, Michigan, Nebraska, and Illinois. Data collection started in June of 2019 and stopped in January of 2020.
The survey sought primarily to evaluate general knowledge. This was a composite variable calculated based on total number of correct responses divided by total number of questions. Additionally, it specifically measured: a) age and smoking history group eligibility, b) cancer specific and overall mortality benefit, c) populations that benefit the most from screening, d) mortality benefit of lung cancer screening with LDCT compared to mammogram and colonoscopy, and e) self-perceived LCS knowledge. Prior to taking the survey, residents were asked not to review the literature on LCS.
The survey was distributed using REDCap (Research Electronic Data Capture) via email containing a public hyperlink leading to an online form. It was sent weekly to all residents and distributed by the authors and their respective program’s coordinators. REDCap is an online software toolset for electronic collection and management of research data. 13 Data was hosted at Indiana University. The study received Ethics exemption from the office of research compliance at Indiana University (protocol #1904577492A001) because it involved research that only included interactions involving educational tests, survey procedures, interview procedures, or observation of public behavior.
Data were analyzed using STATA 14. Descriptive statistics were used to stratify residents by post-graduate year (PGY). Statistical significance was set at P < .05 and was analyzed using Student’s t test and chi-square test, as appropriate.
Results
Forty-six percent (166/360) of residents responded to the survey. The distribution was 42%, 30%, and 28% among PGY-1, PGY-2, and PGY- 3, respectively. The distribution per program was 37%, 15%, 28%, and 20%, respectively.
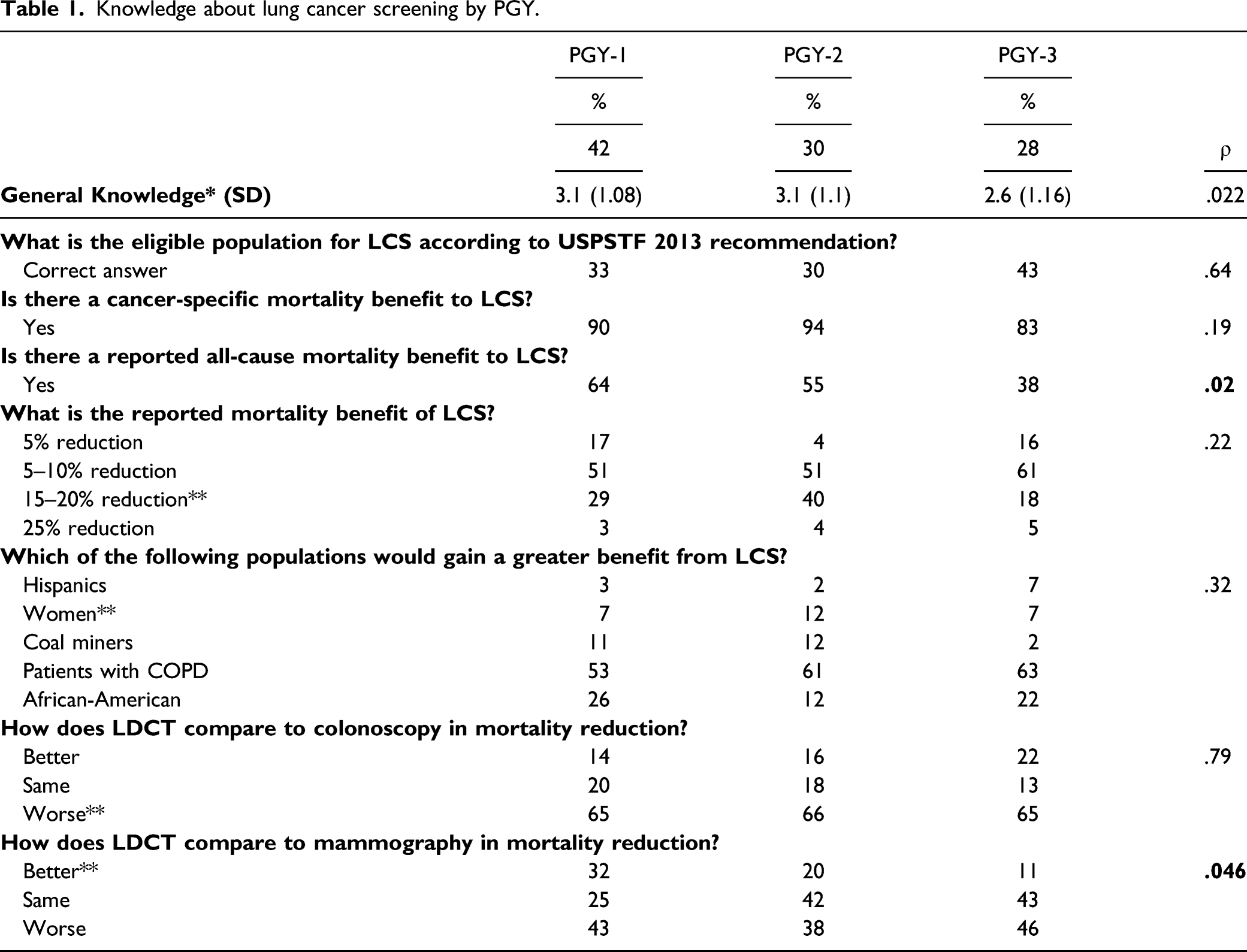
A 2.9/7 (43.1%) general knowledge score was attained among all surveyed. Programs’ general knowledge ranged between 30% and 55% with no statistical significance among them (ρ = .56). General knowledge was statistically significantly better among PGY-1 (42%) outperforming PGY-2 and PGY-3 (30% and 28%, respectively; ρ = .022).
Knowledge about lung cancer screening by PGY.
Knowledge about lung cancer screening by program.


The percentage distribution of general knowledge and self-perceived knowledge regarding lung cancer screening separated by program and PGY (post-graduate year). *Correct answers divided by number of total questions.
Discussion
According to this study, the knowledge of at-risk populations and impact of LDCT on mortality was low amongst IM residents at 4 large training programs in the Midwest U.S. This result is consistent with the finding that, as of 2017, less than 5% of the high risk for lung cancer population are being screened with LDCT in the United States. 3 Improvement in screening rates for high-risk populations requires an improved knowledge base of future primary care physicians, who are most likely to recommend screening modalities for their patients.
CMS has established the age range 14 to be considered for LCS. This age range varies slightly from the landmark NLST trial (55–77 instead of 55–80). 15 The reported lung cancer-specific mortality benefits by Pastorino et al 16 and Becker et al 17 were in the 20–39% range. Most of our respondents selected a lower lung cancer-specific mortality rate benefit, which may inform their decision on whether to recommend the intervention. In the NELSON and MILD trials, women benefited significantly more than men. Fewer than 10% of our respondents were aware of this finding. When we consider the trend in smoking behavior among women compared to men, 18 women may represent a population at overall higher risk of developing lung cancer in the future.
LDCT carries risks, especially in lower-risk populations. A veteran’s administrations study showed a high risk of false positives and an increase rate of this in low-risk population screening. It was suggested this may decrease the risk-benefit ratio for LCS. 19 A different study found that patients who underwent LCS were more likely to continue smoking, possibly because of a false sense of security given by negative screening exams. 4 Notwithstanding, it remains an internationally recommended method of screening. The national smoking rate in the United States is 16.7%. In the United States Midwest, smoking rates are 18.2%, only surpassed by the US South (18.8%). 20 Interventions for early detection of lung cancer are essential to reduce mortality in these areas.
The USPSTF evidence review 2 suggested LDCT and mammogram in women aged 50–59 may have a comparable number needed to screen (NNS) to prevent one death. Based on this metric, LDCT outperformed mammogram and underperformed colonoscopy. Our respondents all agreed that they perceived LDCT to need more patients to prevent one death compared to the other two interventions. We believe that this assessment is consistent with an increased skepticism to new interventions. 18
This is the first study to evaluate the multi-institutional knowledge of lung cancer screening among internal medicine residents. Similar studies in practicing primary care providers or residents echo these findings. 21 The trend for PGY-1 to outperform PGY-2 and PGY-3 residents was consistent among all programs, ratifying a previously seen trend. 10 This may be partially explained by increased motivation or recent medical school curricula or early residency training covering LCS recommendations. There was also a not statistically significantly higher proportion of PGY-1 residents in the sample analyzed.
There are several limitations to this study. Our response group may be more motivated, increasing their willingness to respond and engage with the survey. This may skew the results to better overall knowledge—a concerning hypothesis. All residents must be exposed to primary care settings during their training as required by the American Board of Internal Medicine. However, in university-based programs, most of the residents may decide to go into subspecialty training. Additionally, the lack of time limit in for survey response may have allowed for literature review with no feasible way to control for this. Furthermore, knowledge may not be the only factor in preventing LCS recommendations. Many factors derive from patients, providers, system, and insurance characteristics which may be suboptimal to promote preventive care.
Trainees providing primary care have a fundamental role in preventative health. Lung cancer screening knowledge in all respondents was unacceptably low. In their knowledge self-assessment, most were aware of their deficiencies. Early year residents performed better than their seniors. Uninformed skepticism and knowledge gaps continue to be significant barriers in recommending lung cancer screening.
Footnotes
Author Contributions
Samuel Urrutia-Argueta: Conceptualization and Methodology.
Samuel Urrutia-Argueta: Conceptualization, Methodology, Writing, Editing, Investigation.
Nishraj Basnet: Data curation, Methodology, and Editing.
Owais-Abdul Kafi: Data curation, Methodology, and Editing.
Nasser Hanna: Supervision, Reviewing, Editing, Writing, and Conceptualization.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
This study was approved by the Indiana University IRB #2006129350. Participants granted verbal informed consent as recommended by the IRB prior to answering the survey. This research project was unfunded.