
Abstract
Background
Sedated colonoscopy has been increasingly selected. However, the effect of sedated colonoscopy on polyp/adenoma detection rate (PDR/ADR) remains controversial among studies.
Methods
In this retrospective study, the medical records of 11 504 consecutive patients who underwent colonoscopy at our department from July 1, 2021 to December 31, 2022 were collected. Patients were divided into sedated and unsedated groups according to the use of intravenous sedation during colonoscopy. Overall PDR/ADR, right-side, transverse, and left-side colon PDR/ADR, and single and multiple PDR/ADR were calculated. By adjusting for age, gender, body mass index, inpatient, screening/surveillance, cecal intubation time, colonoscopy withdrawal time ≥6 min, and an endoscopist’s experience ≥5 years, multivariate logistic regression analyses were performed to evaluate the association of sedated colonoscopy with overall PDR/ADR, right-side, transverse, and left-side colon PDR/ADR, and single and multiple PDR/ADR, where the absence of PDR/ADR was used as reference. Odds ratios (ORs) with their 95% confidence intervals (CIs) were calculated.
Results
Overall, 2275 patients were included, of whom 293 and 1982 underwent sedated and unsedated colonoscopy, respectively. Multivariate logistic regression analyses showed that sedated colonoscopy was independently associated with lower overall PDR/ADR (OR = 0.640, 95% CI = 0.460-0.889, P = 0.008), right-side colon PDR/ADR (OR = 0.591, 95% CI = 0.417-0.837, P = 0.003), single PDR/ADR (OR = 0.659, 95% CI = 0.436-0.996, P = 0.048), and multiple PDR/ADR (OR = 0.586, 95% CI = 0.402-0.855, P = 0.005), but not transverse or left-side colon PDR/ADR.
Conclusion
Sedated colonoscopy may not be beneficial in terms of overall PDR/ADR, right-side colon PDR/ADR, and number of polyps/adenomas. Thus, it should be selectively recommended. Additionally, it should be necessary to explore how to improve the quality of sedated colonoscopy.
Introduction
Colonoscopy plays an important role in detecting colorectal lesions, and is regarded as the gold standard for detecting colorectal cancer (CRC) and precancerous lesions.1,2 Unsedated or sedated colonoscopy can be selected according to the individuals’ preference and status. In general, unsedated colonoscopy has some obvious advantages, including rapid recovery, lower cost, and lack of need for escorts.3,4 Nevertheless, during unsedated colonoscopy, some individuals may experience anxiety, abdominal pain, or bloating, thereby causing difficult colonoscopy or even cecal intubation failure.5,6 By contrast, a sedated patient will not experience pain or bloating during colonoscopy, thus an examiner can proceed without requirement to respond to distress. Therefore, sedated colonoscopy should be appropriate for pain-sensitive individuals for improving their satisfaction and acceptance of colonoscopy. 7
In real-world clinical practice, colorectal polyps/adenomas are frequently missed during colonoscopy, causing a misdiagnosis rate of 16.8-28%.8-13 Thus, endoscopists are committed to improving the quality of colonoscopy to reduce the misdiagnosis of polyps/adenomas. Polyp/adenoma detection rate (PDR/ADR) is an important indicator for the quality of colonoscopy, and the improvement of PDR/ADR is beneficial for reducing the risk of interval CRC.14-16 However, it should be noted that PDR/ADR can be affected by multiple factors.17-20 Sedated or unsedated colonoscopy may influence the PDR/ADR. But the conclusion is inconsistent among studies.21-25 In addition, previous studies focused on the effect of sedated colonoscopy on overall PDR/ADR, but not PDRs/ADRs at different colorectal segments. Considering that the incidence and prognosis of CRC located at different colorectal segments are heterogeneous,26,27 it is worthwhile to perform further studies regarding the effects of sedated colonoscopy on PDRs/ADRs at different colorectal segments.
Herein, our current study aimed to investigate the effects of sedated colonoscopy on both overall PDR/ADR and PDRs/ADRs at different colorectal segments. Furthermore, the association of sedated colonoscopy with single and multiple PDR/ADR was also evaluated.
Methods
Study Design
In this retrospective study, the medical records of 11 504 consecutive patients who underwent colonoscopy at the Department of Gastroenterology of the General Hospital of Northern Theater Command from July 1, 2021 to December 31, 2022 were collected. The exclusion criteria were as follows: (1) incomplete colonoscopy due to endoscopic therapy alone, ultrasonic colonoscopy alone, or poor bowel preparation; (2) failed cecal intubation due to colonic stenosis, patients’ intolerable pain, or colonic redundancy; (3) history of colectomy; (4) inflammatory bowel disease; (5) familial polyposis; and (6) cecal intubation time (CIT) was not recorded. This study was approved by the Medical Ethical Committee of the General Hospital of Northern Theater Command [Y (2023) 177] on September 27, 2023, and performed following the 1975 Declaration of Helsinki. This study conformed to the STROBE guidelines. 28 All patients’ details were de-identified. Due to the retrospective nature of the study, the requirement for written informed consent was waived.
Data Collection
The following data was collected: age, gender, height, weight, type of patient (i.e., outpatient or inpatient), type of colonoscopy (i.e., sedated or unsedated), screening/surveillance, endoscopists’ experiences, CIT, colonoscopy withdrawal time, and major colonoscopic findings (i.e., colon diverticulosis, colitis, and polyps/adenomas). Body mass index (BMI) was calculated.
Definitions
PDR/ADR was defined as the proportion of patients with at least 1 polyp or adenoma detected during colonoscopy. 29
Location of polyps/adenomas included right-side colon, transverse colon, and left-side colon. Right-side colon referred to the cecum and ascending colon; transverse colon referred to the hepatic flexure, transverse colon, and splenic flexure; and left-side colon referred to the descending colon, sigmoid colon, and rectum.
Number of polyps/adenomas was classified as single and multiple. Single polyp/adenoma was defined as only 1 polyp/adenoma was detected during colonoscopy; and multiple polyps/adenomas were defined as 2 or more polyps/adenomas were detected during colonoscopy.
CIT was defined as the time from the anus to ileocecal valve, appendiceal orifice or terminal ileum by the colonoscope. 30 Colonoscopy withdrawal time was defined as the time for colonoscopy withdrawal from the cecum to the anus, 29 including the time for removing polyp/adenoma.
Group and Procedures
All patients signed informed consent forms related to colonoscopy. All included patients were divided into sedated and unsedated groups according to the use of intravenous sedation during colonoscopy. In the sedated group, the participants received sedation medication including propofol or etomidate at our department, and in the unsedated group, the participants did not receive any sedation-related medication. It is worth noting that unsedated colonoscopy did not include conscious sedation, as mentioned in our previous study.30-32 The type and dosage of sedation medication used during induction were individually selected by our anesthesiologists according to the patient’s height, weight, and medical history. The requirement of additional dosage of sedation was dependent upon the duration of colonoscopy. Electrocardiographic monitoring and oxygen inhalation through a nasal catheter were given to all patients in the sedated group.
Statistical Analyses
IBM SPSS version 26.0 statistical software (IBM Corp, Armonk, New York, USA) was used for the data analyses. Continuous variables were reported as mean ± standard deviation and median (range), and categorical variables were reported as frequency (percentage). Student’s t-tests were used for continuous variables and chi-square tests for categorical variables. Overall PDR/ADR, right-side, transverse, and left-side colon PDR/ADR, single and multiple PDR/ADR were calculated. Univariate and multivariate logistic regression analyses were performed to explore whether sedated colonoscopy was associated with overall PDR/ADR, right-side, transverse, and left-side colon PDR/ADR, and single and multiple PDR/ADR, where the absence of PDR/ADR was used as reference. Age, gender, BMI, inpatient, screening/surveillance, CIT, colonoscopy withdrawal time ≥6 min, and an endoscopist’s experience ≥5 years were adjusted in multivariate logistic regression analyses. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. A two-tailed P value of <0.05 was considered statistically significant.
Results
Characteristics of Study Population
Overall, 2275 patients were included (Figure 1). The median age was 52.05 ± 14.21 years, and 45.8 % of patients were female. The median BMI was 24.09 ± 3.51 kg/m2, the median CIT was 7.79 ± 5.36 min, and the median colonoscopy withdrawal time was 13.42 ± 10.53 min. Among them, 10.1% had colon diverticulosis and 13.5% had colitis. Overall PDR/ADR was 61.5%. Right-side colon, transverse colon, and left-side colon PDR/ADR was 22.3%, 25.7%, and 48.6%, respectively. Single and multiple PDR/ADR was 17.4% and 44.1%, respectively. The proportion of patients who underwent colonoscopy by endoscopists with experiences ≥5 years was 53.6% (Table 1). Flowchart of patients’ enrollment. Characteristics of Study Population. Abbreviations: SD, standard deviation; No. Pts., numbers of patients; BMI, body mass index; CIT, cecal intubation time; PDR/ADR, polyp/adenoma detection rate.

Comparison Between Sedated and Unsedated Groups
Comparison Between Sedated and Unsedated Groups.
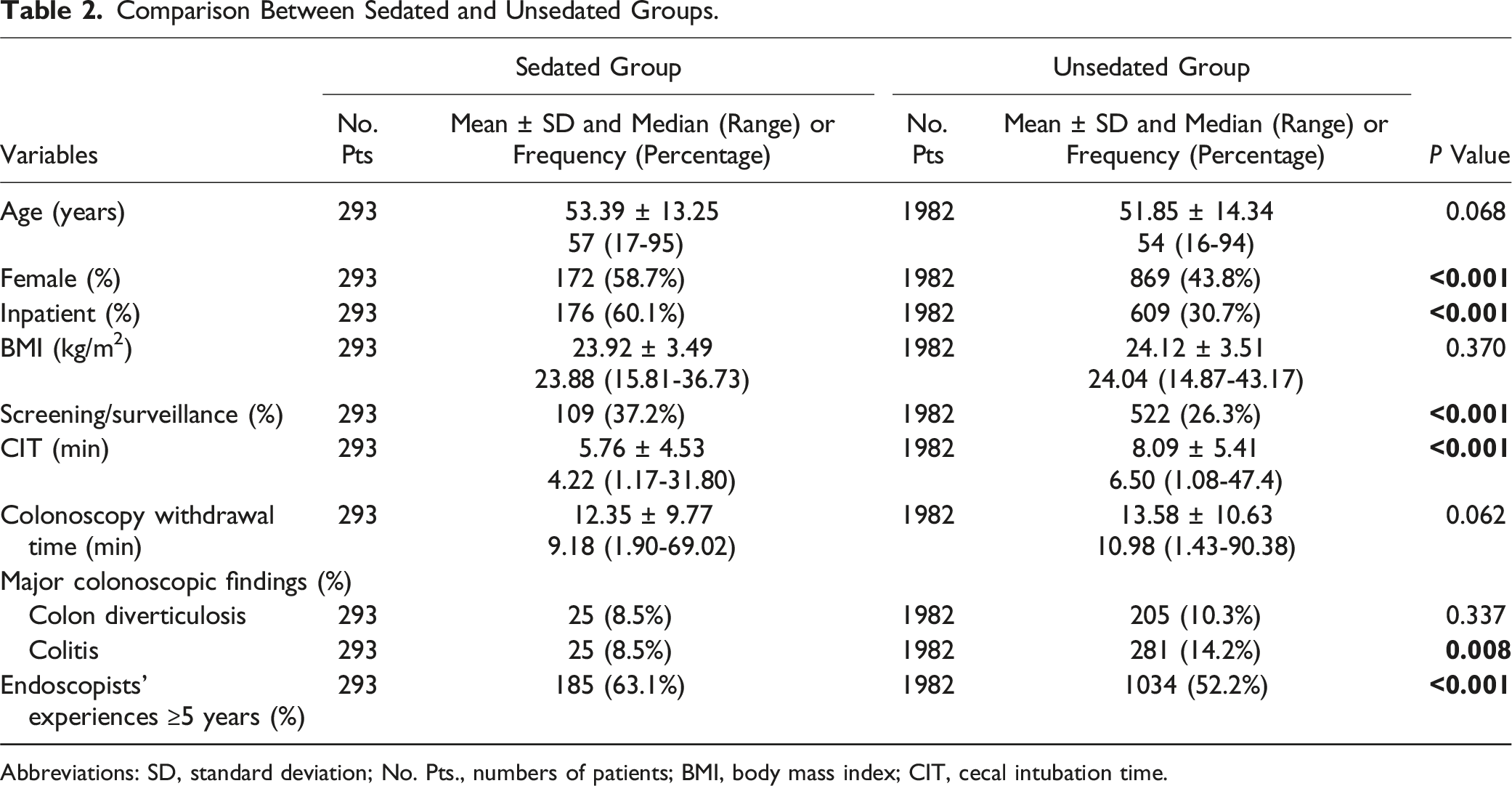
Abbreviations: SD, standard deviation; No. Pts., numbers of patients; BMI, body mass index; CIT, cecal intubation time.
Association of Sedated Colonoscopy with PDRs/ADRs
Logistic Regression Analyses of Association of Sedated Colonoscopy With PDRs/ADRs.
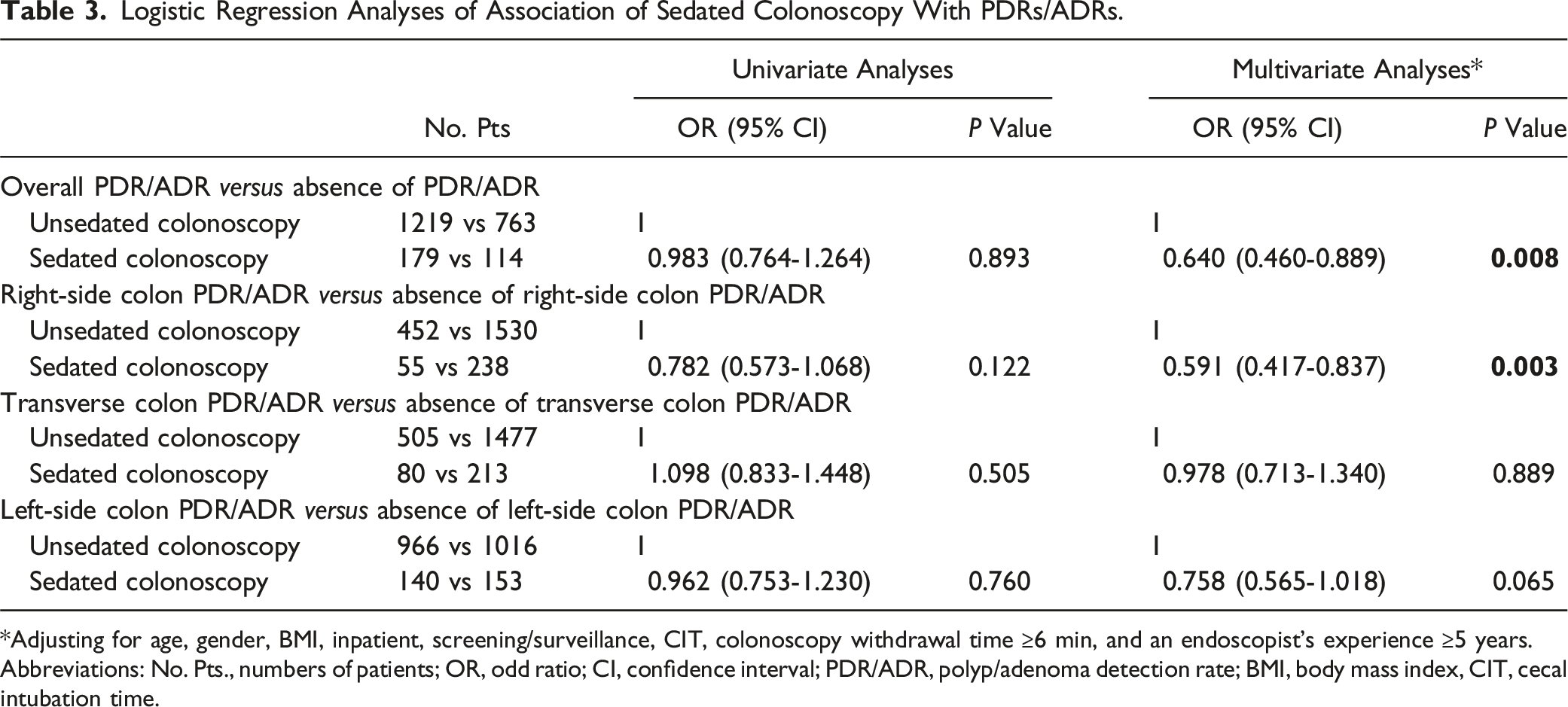
*Adjusting for age, gender, BMI, inpatient, screening/surveillance, CIT, colonoscopy withdrawal time ≥6 min, and an endoscopist’s experience ≥5 years.
Abbreviations: No. Pts., numbers of patients; OR, odd ratio; CI, confidence interval; PDR/ADR, polyp/adenoma detection rate; BMI, body mass index, CIT, cecal intubation time.
Association of Sedated Colonoscopy with Single and Multiple PDR/ADR
Logistic Regression Analyses of Association of Sedated Colonoscopy With Single and Multiple PDR/ADR.

*Adjusting for age, gender, BMI, inpatient, screening/surveillance, CIT, colonoscopy withdrawal time ≥6 min, and an endoscopist’s experience ≥5 years.
Abbreviations: No. Pts., numbers of patients; OR, odd ratio; CI, confidence interval; PDR/ADR, polyp/adenoma detection rate; BMI, body mass index, CIT, cecal intubation time.
Discussion
There were some major findings in the current study. First, sedated colonoscopy was inversely associated with overall PDR/ADR, right-side colon PDR/ADR, and single and multiple PDR/ADR. Second, sedated colonoscopy could not significantly influence transverse colon or left-side colon PDR/ADR.
Nowadays, sedation is increasingly used for colonoscopy. However, the selection of sedated colonoscopy may be influenced by patients’ age and conditions. Nearly all patients can undergo sedated colonoscopy, but there are some relative contraindications, such as American Society of Anesthesiologists physical status class 4, cardiorespiratory-decompensation with chronic global obstructive lung disease, and allergy of sedation medication, etc. 33 Patients with relative contraindication may undergo sedated colonoscopy under close monitoring by experienced anesthesiologists. In addition, sedated patients may have some sedation-related adverse events, such as aspiration, respiratory depression, hypoxemia, oxygen desaturation, and hypotension, so monitoring of the patient’s heart rate, arterial oxygen saturation, blood pressure, and state of consciousness must be performed and appropriate resuscitation equipment must be prepared during colonscopy. 34 In our study, all sedated patients were assessed for anesthesia risk before colonoscopy. Their heart rate, arterial oxygen saturation, and blood pressure were closely monitored by anesthesiologists during colonoscopy.
Some previous studies evaluated the effect of sedated colonoscopy on PDR/ADR, but their conclusions were controversial. Bannert et al, 24 Zhao et al, 35 and Shavakhi et al. 36 found no significant difference in PDR/ADR between sedated and unsedated colonoscopy, but they did not perform multivariate logistic regression analyses. Lang et al. 25 performed multivariate logistic regression analysis and found that sedated colonoscopy was not significantly associated with PDR/ADR after adjusting for confounder factors, but they only included participants who underwent screening colonoscopies. By comparison, Khan et al. 21 and Xu et al. 37 found that sedated colonoscopy was significantly associated with a higher ADR. However, the number of patients included in the study by Khan et al. 21 was greatly different between sedated and unsedated groups, and only patients aged 45-65 years were included in the study by Xu et al, 37 which might affect the generalizability of the conclusions. Compared with previous studies, our study has some strengths. First, except for the effect of sedated colonoscopy on overall PDR/ADR, we also evaluated the effects of sedated colonoscopy on PDRs/ADRs at different colorectal segments, and single and multiple PDR/ADR. Second, apart from univariate logistic regression analyses, we also performed multivariate logistic regression analyses to explore the association between sedated colonoscopy and overall PDR/ADR, PDRs/ADRs at different colorectal segments, and single and multiple PDR/ADR. Third, we did not restrict the indication for colonoscopy or age of included patients.
There were several possible explanations for inverse association of sedated colonoscopy with overall PDR/ADR and number of polyps/adenomas. First, patients could not feel pain or discomfort during sedated colonoscopy, thus it’s more likely that endoscopists insufflate a large amount of air to the colon. 24 In this setting, the intestinal wall may be overexpanded, thereby missing some small and flat polyps/adenomas. Second, compared with those undergoing sedated colonoscopy, patients undergoing unsedated colonoscopy are easier to change their positions for exposing unobservable colonic mucosa locating in the colonic angulation.18,38 Third, patients could communicate with endoscopists during unsedated colonoscopy, and even ask them to inspect some colorectal segments repeatedly. 3
There were also several possible explanations for an inverse association between sedated colonoscopy and right-side colon PDR/ADR. First, patients undergoing sedated colonoscopy are always lying on the left lateral position, which may decrease luminal distention of the cecum.39,40 Luminal distension positively correlated with polyp/adenoma detection.18,41 Therefore, cecal PDR/ADR may be reduced in patients undergoing sedated colonoscopy. Second, because polyps/adenomas in the right-side colon are always flat,42-44 air aspiration on right-side colon is required to reduce missed rate. During unsedated colonoscopy, endoscopists often control air insufflation in the right-side colon to minimize the patient’s discomforts. Thus, right-side colon PDR/ADR may be increased in patients undergoing unsedated colonoscopy. By contrast, during sedated colonoscopy, the overexpansion of intestinal wall may be more likely to occur, leading to a higher probability of missing polyps/adenomas in the right-side colon. Third, ascending colon folds are multiple and deep, and polyps/adenomas in the ascending colon are frequently located on the proximal side of the folds.17,45 When the intestine moves, polyps/adenomas behind folds could be exposed during colonoscopy. However, the use of sedation would reduce intestinal motility, missing such polyps/adenomas. 46
There were several limitations in the current study. First, we were not able to obtain patients’ position information which might affect luminal distention and detection of polyps/adenomas. Second, the detection rates of colorectal polyps and adenomas were not separately reported, because not all included patients had pathological reports. Third, a large number of patients were excluded due to the incomplete data of withdrawal time, thereby causing selection bias.
Conclusion
In conclusion, sedated colonoscopy may miss some polyps/adenomas, especially those in the right-side colon. However, our findings need to be further confirmed in well-designed prospective studies. Additionally, how to improve PDR/ADR during sedated colonoscopy deserves further studies.
Abbreviations
adenoma detection rate
polyp detection rate
colorectal cancer
body mass index
cecal intubation time
Footnotes
Authors’ Contributions
Conceptualization: Xingshun Qi; Formal analysis: Jie Han and Xingshun Qi; Data curation: Jie Han, Rongrong Cao, Dongshuai Su, Yingchao Li, and Xingshun Qi; Writing–original draft: Jie Han, Rongrong Cao, Yingchao Li, and Xingshun Qi; Writing–review and editing: Jie Han, Rongrong Cao, Dongshuai Su, Yingchao Li, Cong Gao, Fei Gao, Xingshun Qi. Supervision: Fei Gao and Xingshun Qi. All authors have made an intellectual contribution to the manuscript and approved the submission.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.