
Abstract
Background:
Adequate bowel preparation quality is essential for high-quality colonoscopy according to the current guidelines. However, the effect of excellent bowel preparation on adenoma/polyp detection rate (ADR/PDR) remained controversial.
Methods:
During the period from December 2020 to August 2022, a total of 1566 consecutive patients underwent colonoscopy by an endoscopist. Their medical records were reviewed. According to the Boston bowel preparation scale, patients were divided into excellent, good, and poor bowel preparation quality groups. ADR/PDR, diminutive ADR/PDR, small ADR/PDR, intermediate ADR/PDR, large ADR/PDR, and number of adenomas/polyps were compared among them. Logistic regression analyses were performed to identify the factors that were significantly associated with ADR/PDR.
Results:
Overall, 1232 patients were included, of whom 463, 636, and 133 were assigned to the excellent, good, and poor groups, respectively. The good group had a significantly higher ADR/PDR (66% vs 55%, P = .015) and a larger number of adenomas/polyps (2.5 ± 3.2 vs 2.0 ± 2.8, P = .030) than the poor group. Both ADR/PDR (63% vs 55%, P = .097) and number of adenomas/polyps (2.2 ± 2.8 vs 2.0 ± 2.8, P = .219) were not significantly different between excellent and poor groups. The excellent (9% vs 4%, P = .045) and good (9% vs 4%, P = .040) groups had a significantly higher intermediate ADR/PDR than the poor group. Logistic regression analyses showed that either good (odds ratio [OR] = 1.786, 95% CI = 1.046-3.047, P = .034) or excellent (OR = 2.179, 95% CI = 1.241-3.826, P = .007) bowel preparation quality was independently associated with a higher ADR/PDR compared with poor bowel preparation quality. Excellent (OR = 1.202, 95% CI = 0.848-1.704, P = .302) bowel preparation quality was not independently associated with a higher ADR/PDR compared with good bowel preparation quality.
Conclusions:
The pursuit of excellence in bowel preparation does not show an association with increased ADR/PDR and number of adenomas/polyps compared with a good level. In addition, our study further contributes to the existing evidence that poor bowel preparation compromises ADR/PDR and number of adenomas/polyps.
Introduction
Colorectal cancer (CRC) is the third most common cancer and the fourth leading cause of cancer-related death worldwide. 1 Colonoscopy is the most effective approach for screening for CRC, which can significantly reduce the morbidity and mortality of CRC.2,3 Adenoma detection rate (ADR) is considered a critical performance indicator and quality assurance standard for colonoscopy. 4 An improved ADR has been shown to be associated with a reduced incidence of post-colonoscopy CRC.5,6
Factors associated with ADR include the skills of endoscopists, withdrawal time of colonoscopy, age and gender of patients, a personal history of colorectal polyp or cancer, endoscopic devices, and bowel preparation quality.7-10 Among them, bowel preparation quality plays an important role in influencing ADR.11,12 Poor bowel preparation quality is strongly associated with lower rates of cecal intubation, longer time of colonoscopy, lower rates of lesion detection, higher rates of complications, and increased patient discomfort during colonoscopy.12-14 Therefore, guidelines have proposed that the rate of adequate bowel preparation for high-quality colonoscopy to be achieved in 90% of patients.4,15
There is still a controversy on whether better bowel preparation quality improves ADR.11,12,16-20 Some studies showed that ADR was increased with the improvement of bowel preparation quality. 19 However, others demonstrated that ADR was statistically similar between excellent and good bowel preparation quality groups 18 and even found that ADR was significantly higher in good bowel preparation quality group than excellent bowel preparation quality group. 17 For this reason, we have conducted this study to further evaluate the difference in ADR or polyp detection rate (PDR) among bowel preparation quality groups by reviewing the data of colonoscopy by the same endoscopist.
Methods
Study design
We retrospectively screened the medical records of 1566 consecutive patients who underwent colonoscopy by an endoscopist (X.Q.) at the Department of Gastroenterology of the General Hospital of Northern Theater Command from December 3, 2020 to August 31, 2022. The endoscopist completed nearly 500 colonoscopies before the study period and was skilled at the diagnosis and treatment of intestinal diseases on endoscopy as previously described. 21 The exclusion criteria were as follows: (1) patients hospitalized for resection of colorectal adenomas/polyps; (2) patients diagnosed with inflammatory bowel disease or familial polyposis; (3) patients with a history of colectomy; (4) cecal intubation was unnecessary or unsuccessful; (5) bowel preparation score data was missing; and (6) colonoscopy was not performed by this endoscopist alone. The study protocol was reviewed and the approval of the Ethics Committee of the General Hospital of Northern Theater Command has been obtained (Y (2023) 028). The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. The requirement for informed consent for this study was waived, and all the data were de-identified.
Data collection
The following data were collected by our study group: age, gender, height, weight, type of patient (outpatient or inpatient), type of colonoscopy (sedated or unsedated), history of colonoscopy, history of abdominal surgery, time of starting colonoscopy (morning or afternoon), indications for colonoscopy (ie, abdominal discomfort, formless stool, difficult defecation, and screening/surveillance), major findings during colonoscopy (ie, size, number, and location of colorectal adenomas/polyps), cecal intubation time, colonoscopy withdrawal time, and bowel preparation score. Body mass index (BMI) was calculated. The accuracy of original data was checked by 3 investigators (Y.L., C.G., and D.S.).
Definitions and group
Bowel preparation score was evaluated by the Boston bowel preparation scale (BBPS). 22 The BBPS score for each colon segment (right, transverse, and left colon segment) ranged from 0 to 3. The total BBPS score was the sum of the BBPS scores of the 3 colon segments. Excellent bowel preparation quality was defined as a total BBPS score of ⩾8; good bowel preparation quality was defined as a total BBPS score of 6 or 7 with a BBPS score of ⩾2 for each colon segment; and poor bowel preparation quality was defined as a BBPS score of <2 for any colon segment. According to the BBPS score, patients were divided into excellent, good, and poor groups. Excellent and good bowel preparation quality were considered as adequate bowel preparation quality.
ADR/PDR was defined as the proportion of patients with at least one adenoma/polyp detected during colonoscopy among all included patients.
Diminutive adenoma/polyp was defined as its size of ⩽5 mm, small adenoma/polyp as 6 to 9 mm, intermediate adenoma/polyp as 10 to 19 mm, and large adenoma/polyp as ⩾20 mm. 23
Colonoscopy withdrawal time also included the time of biopsy and adenoma/polyp resection in the present study.
Procedures
A split-dose regimen consisting of 3 bags of polyethylene glycol (PEG-4000) solution with 3 L of water was used for all colonoscopies. Specifically, patients were asked to take 1 bag of PEG-4000 with 1 L of water at the night before colonoscopy, and 2 other bags of PEG-4000 with 2 L of water and 30 mL of simethicone in the morning of colonoscopy as previously described. 24 If a patient was planned to undergo colonoscopy in the afternoon, the last 2 bags of PEG-4000 with 2 L of water and 30 mL of simethicone were permitted to be taken at noon. If a patient felt that bowel preparation quality was inadequate after traditional bowel preparation, an additional bag of PEG-4000 could be taken. Even if a patient did not strictly undergo bowel preparation according to our protocol of bowel preparation, we would discuss with him or her about whether the colonoscopy was performed. The Fujinon colonoscope (EC-530WM, EC-450WI5, EC-250WM5, Japan) was used, and all procedures were completed using white light endoscopy. The number, location, and size of adenomas/polyps detected during colonoscopy were recorded.
Statistical analyses
Continuous variables were expressed as mean ± standard deviation and median (range), and compared by nonparametric Kruskal-Wallis test or Mann-Whitney U test. Categorical variables were expressed as frequency (percentage) and compared by chi-square test. ADR/PDR, diminutive ADR/PDR, small ADR/PDR, intermediate ADR/PDR, large ADR/PDR, and number of adenomas/polyps were compared between the excellent, good, and poor bowel preparation quality groups. Notably, if the number of adenomas/polyps was ambiguously recorded as multiple, more than 10, or dozens in a patient, the data would be excluded from statistical analyses regarding the difference in the number of adenomas/polyps among the 3 groups. Logistic regression analyses were performed to identify the factors that were significantly associated with ADR/PDR. Variables with P < .1 in univariate analyses were enrolled in multivariate analyses. Odds ratios (ORs) with 95% CIs were calculated. A 2-tailed P < .05 was considered statistically significant. All statistical analyses were performed using IBM SPSS version 20.0 statistical software (IBM Corp, Armonk, New York, USA). Statistical results were checked by 1 investigator (K.W.).
Results
Characteristics of patients
Overall, 1232 patients were included in the final analysis (Figure 1). The mean age was 51.5 years, the mean BMI was 24.1 kg/m2, and the proportion of female was 45.9% (Table 1).
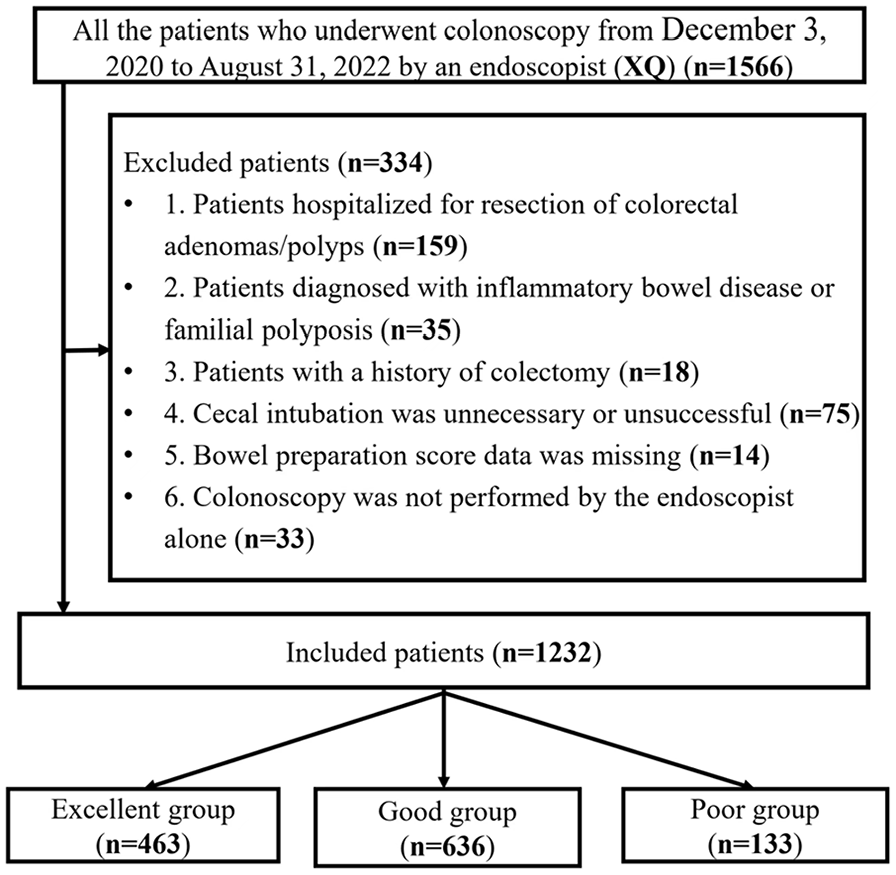
Flowchart of patients’ enrollment.
Characteristics of included patients.
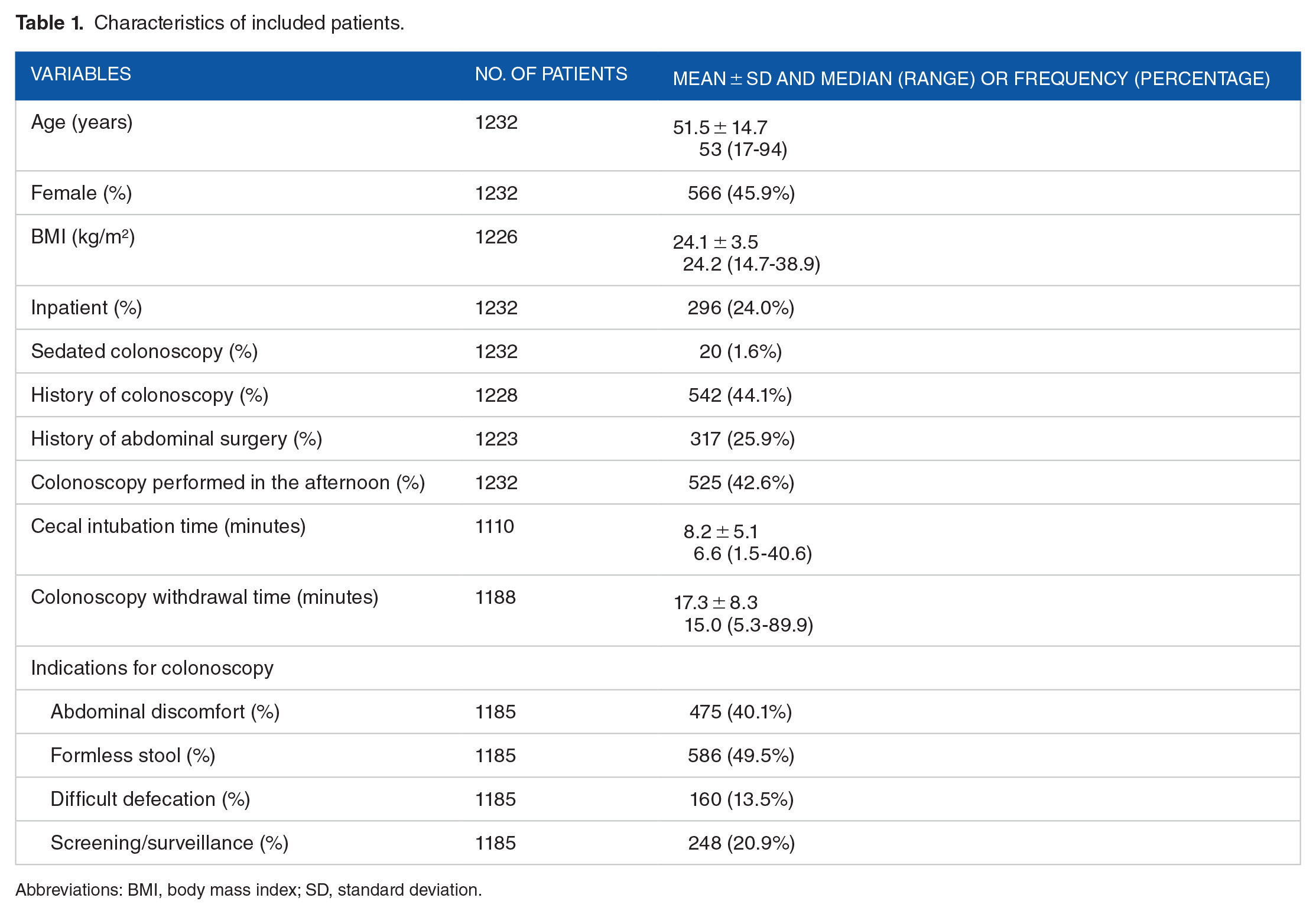
Abbreviations: BMI, body mass index; SD, standard deviation.
Among them, 463, 636, and 133 patients were assigned to the excellent, good, and poor groups, respectively. There was significant difference in the proportions of female (50.5% vs 44.8% vs 35.3%, P = .006), colonoscopy performed in the afternoon (31.7% vs 48.1% vs 54.1%, P < .001), formless stool (55.7% vs 48.4% vs 32.3%, P < .001), difficult defecation (9.4% vs 14.3% vs 24.2%, P < .001), BMI (23.8 ± 3.4 kg/m2 vs 24.4 ± 3.5 kg/m2 vs 24.1 ± 4.0 kg/m2, P = .024), and colonoscopy withdrawal time (16.5 ± 7.5 minutes vs 17.7 ± 8.8 minutes vs 17.4 ± 8.5 minutes, P = .042) among the 3 groups (Table 2).
Characteristics of patients among excellent group, good group, and poor group.
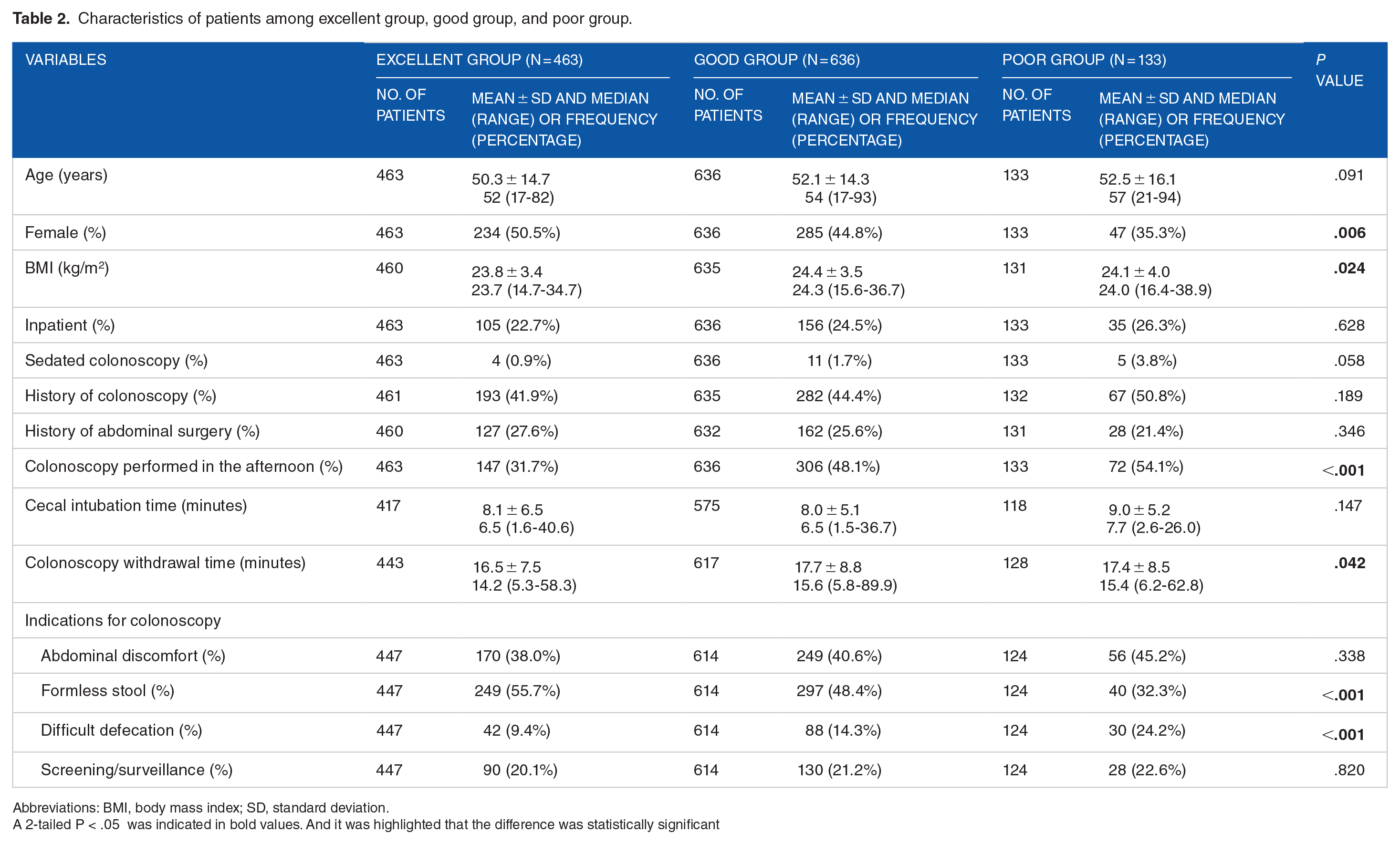
Abbreviations: BMI, body mass index; SD, standard deviation.
A 2-tailed P < .05 was indicated in bold values. And it was highlighted that the difference was statistically significant
ADR/PDR
Overall ADR/PDR were 291/463 (63%), 420/636 (66%), and 73/133 (55%) in the excellent, good, and poor groups, respectively. Compared with the poor group, the good group had a significantly higher ADR/PDR (P = .015).
In the 3 groups, diminutive ADR/PDR was 264/463 (57%), 389/636 (61%), and 71/133 (53%), respectively; small ADR/PDR was 83/463 (18%), 130/636 (20%), and 24/133 (18%), respectively; intermediate ADR/PDR was 42/463 (9%), 58/636 (9%), and 5/133 (4%), respectively; and large ADR/PDR was 7/463 (2%), 10/636 (2%), and 0/133 (0%), respectively. The excellent group (P = .045) and the good group (P = .040) had a significantly higher intermediate ADR/PDR than the poor group. But there was no significant difference in diminutive ADR/PDR, small ADR/PDR, and large ADR/PDR between the poor, good, and excellent groups (Figure 2).

Bar diagrams showing main findings among the excellent, good, and poor groups. ADR/PDR indicates adenoma/polyp detection rate.
Factors associated with overall ADR/PDR
In the overall patients, univariate logistic regression analysis showed that age ⩾50 years (OR = 3.240, 95% CI = 2.545-4.125, P < .001), BMI ⩾ 25.0 kg/m2 (OR = 1.324, 95% CI = 1.040-1.678, P = .023), inpatient (OR = 1.868, 95% CI = 1.396-2.498, P < .001), history of colonoscopy (OR = 1.828, 95% CI = 1.438-2.325, P < .001), longer cecal intubation time (OR = 1.031, 95% CI = 1.005-1.057, P = .018), longer colonoscopy withdrawal time (OR = 1.372, 95% CI = 1.315-1.432, P < .001), and screening/surveillance (OR = 1.780, 95% CI = 1.303-2.432, P < .001) were significantly associated with a higher ADR/PDR; and colonoscopy performed in the afternoon (OR = 0.772, 95% CI = 0.611-0.976, P = .030), abdominal discomfort (OR = 0.712, 95% CI = 0.560-0.906, P = .006), and formless stool (OR = 0.710, 95% CI = 0.560-0.901, P = .005) were significantly associated with a lower ADR/PDR (Table 3).
Univariate and multivariate logistic regression analyses of factors associated with ADR/PDR in all patients.

Abbreviations: ADR/PDR, adenoma/polyp detection rate; BMI, body mass index; OR, odd ratio; CI, confidence interval.
A 2-tailed P < .05 was indicated in bold values. And it was highlighted that the difference was statistically significant.
In the overall patients, multivariate logistic regression analysis showed that good bowel preparation quality (OR = 1.786, 95% CI = 1.046-3.047, P = .034) and excellent bowel preparation quality (OR = 2.179, 95%= 1.241-3.826, P = .007) remained independently associated with a higher ADR/PDR (Table 3).
In the patients with adequate bowel preparation quality, both univariate (OR = 0.870, 95% CI = 0.678-1.117, P = .275) and multivariate logistic regression analyses (OR = 1.202, 95% CI = 0.848-1.704, P = .302) showed that excellent bowel preparation quality was not associated with a higher ADR/PDR (Table 4).
Univariate and multivariate logistic regression analyses regarding the effect of excellent and good bowel preparation quality on ADR/PDR.
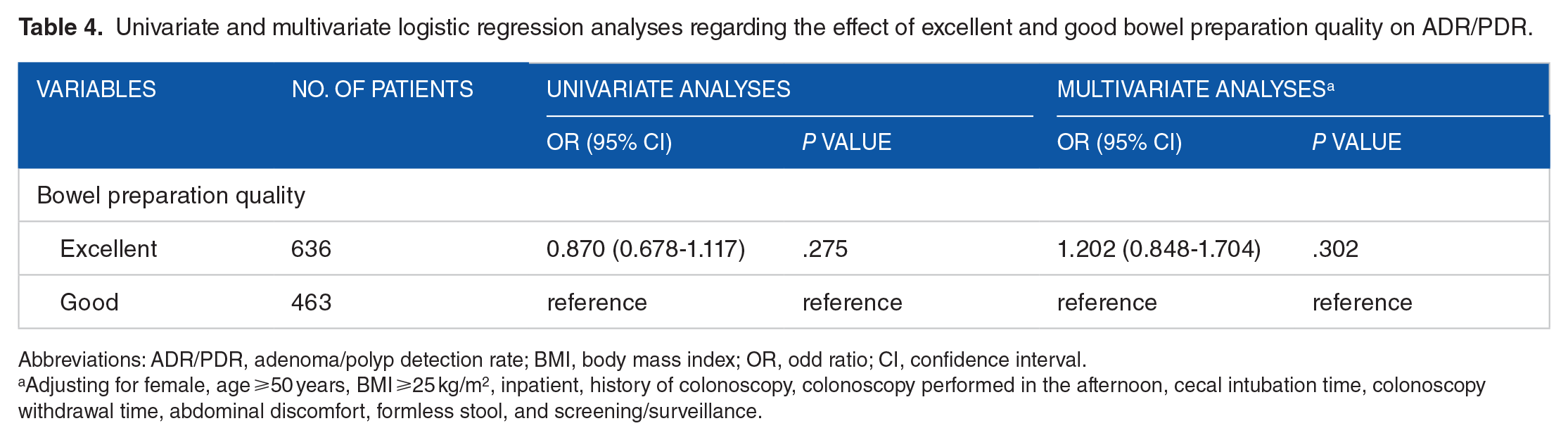
Abbreviations: ADR/PDR, adenoma/polyp detection rate; BMI, body mass index; OR, odd ratio; CI, confidence interval.
Adjusting for female, age ⩾50 years, BMI ⩾25 kg/m2, inpatient, history of colonoscopy, colonoscopy performed in the afternoon, cecal intubation time, colonoscopy withdrawal time, abdominal discomfort, formless stool, and screening/surveillance.
Number of adenomas/polyps
Number of adenomas/polyps was 2.2 ± 2.8, 2.5 ± 3.2, and 2.0 ± 2.8 in the excellent, good, and poor groups, respectively. Compared with the poor group, the good group had a significantly larger number of adenomas/polyps (P = .030) (Figure 3).

Box diagram showing number of adenomas/polyps among the excellent, good, and poor groups.
Discussion
The main findings of the current study were as follows. First, good bowel preparation quality has the highest ADR/PDR, followed by excellent and poor bowel preparation quality. Notably, the difference in ADR/PDR between good and poor bowel preparation quality groups becomes statistically significant. Second, adequate bowel preparation quality should be an independent risk factor associated with improved ADR/PDR. Third, according to the size of adenoma/polyp, only intermediate ADR/PDR, but not diminutive ADR/PDR, small ADR/PDR, or large ADR/PDR, is significantly improved by adequate bowel preparation quality.
Until now, many criteria for scoring bowel preparation quality have been established. Among them, the Aronchick Scale, BBPS, and Ottawa Bowel Preparation Scale have been verified and commonly employed. 25 In this study, BBPS was used to evaluate bowel preparation quality. Notably, BBPS score should be calculated during colonoscopy withdrawal procedure and after flushing and suctioning fluid and food residue by endoscopists. 22 According to the BBPS score, our patients were divided into 3 groups and then ADR/PDR was compared among them. By comparison, the difference in ADR/PDR was analyzed according to the endoscopists’ subjective and intuitive criteria for bowel preparation quality in other studies.16,18
Few previous studies discussed the influence of different endoscopists on the relationship of bowel preparation quality with ADR/PDR. Notably, different endoscopists scored the same bowel preparation differently. Moreover, for the same group of patients, ADR/PDR might also be different among endoscopists. 26 Our study evaluated the relationship of bowel preparation quality with ADR/PDR in only one endoscopist, which substantially avoided bias from different endoscopists.
It has been traditionally accepted that ADR/PDR is increased with the improvement of BBPS. Guo et al 19 showed that ADR was increased from 11.9% to 32.6% with an improvement in the total BBPS score from 4 to 9. Similarly, Tholey et al 18 found that sessile serrated PDR was significantly increased with an improvement of bowel preparation quality from good to excellent. By contrast, our study found that ADR/PDR, diminutive ADR/PDR, small ADR/PDR, intermediate ADR/PDR, and large ADR/PDR in the good bowel preparation quality group were higher than or similar with the excellent bowel preparation quality group, which was consistent with the findings by Calderwood et al 17 that ADR/PDR was significantly higher in patients with a total BBPS score of 6 to 8 than those with a total BBPS score of 9. There are some explanations for this seemingly counterintuitive phenomenon. First, excellent bowel preparation quality is often more conducive to observe colorectal mucosa. However, it should be noted that additional time on flushing and suctioning fluid and food residue during colonoscopy withdrawal procedure should be warranted to improve from good to excellent bowel preparation quality. If the total withdrawal time was relatively consistent or maintained, the time on detecting adenoma/polyp in other bowel segments, which are clean and do not require flushing and suctioning, would be shortened, probably causing missed adenoma/polyp. Second, our study demonstrated that the total withdrawal time was the shortest in excellent bowel preparation quality group, suggesting that an excellent visual field would reduce the endoscopist’s vigilance and speed up colonoscopy withdrawal, thus possibly ignoring adenoma/polyp. Third, it is more likely that fluid and food residue remain in proximal colon and the curved parts of bowel (ie, hepatic flexure and splenic flexure). Accordingly, bowel preparation at these parts is more prone to be of poor quality, 27 necessitating repeated flushing and suctioning, which increases the frequency of observation, thereby leading to higher ADR/PDR.28,29 Fourth, patients with good bowel function but without predisposing factors of adenoma/polyp may have a higher probability of excellent bowel preparation quality, vice versa.30,31 Fifth, we found that the largest number of adenomas/polyps was observed in the good bowel preparation quality group, which further supported that good bowel preparation quality should be a supreme condition for colonoscopy.
In addition, we found that intermediate ADR/PDR was significantly reduced by poor bowel preparation quality, which was inconsistent with previous findings by Sherer et al 16 that diminutive ADR was significantly reduced by poor bowel preparation quality. This may be because diminutive adenoma/polyp tends to be multiple and is difficult to be ignored regardless of bowel preparation quality; by contrast, intermediate adenoma/polyp is more likely to be single and thus is easy to be missed in the setting of poor bowel preparation quality.
The current study had some limitations. First, the withdrawal time also included the time of biopsy and adenoma/polyp resection in some patients.4,15 Regardless, it should be beyond 6 minutes in all of our patients. Second, the pathological reports could not be obtained in some patients. Thus, we could not accurately differentiate between adenoma and polyp. Third, baseline information was insufficient in some patients. Fourth, the study was conducted at a single center and colonscopy procedures were performed by a single endoscopist, limiting the generalization of the results. Fifth, the basic information we retrospectively collected was not comprehensive. Comorbidities, dietary habits, medication use, positive fecal occult blood test, weight loss, and family history, which could significantly influence bowel preparation quality and ADR/PDR, were lacking.
Conclusions
Excellent bowel preparation quality is not superior to good bowel preparation quality for improving ADR/PDR and number of adenomas/polyps. In contrast, poor bowel preparation quality significantly reduces ADR/PDR and number of adenomas/polyps. Therefore, adequate bowel preparation quality is necessary during colonoscopy, but there is no need to pursue the excellence in bowel preparation quality.
Footnotes
Acknowledgements
We would like to express gratitude to our study team for establishing and updating the database, including Hongxin Chen, Haijuan Yao, Cong Gao, Yingchao Li, and Yuhang Yin.
Correction (February 2024):
This abstract section of this article has been updated to correct the ‘ADR/PDR (63% vs 55%’ to ADR/PDR (66% vs 55%’. Also, one minor grammatical correction has been incorporated.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
XQ contributed to conceptualization, project administration, supervision, visualization, and writing—review and editing. YL contributed to data curation, formal analysis, methodology, software, and writing—original draft. FM and RC contributed to data curation, software, and writing—original draft. CG, DS, KW, and JH contributed to data curation, software, and writing—original draft. All authors have made an intellectual contribution to the manuscript and approved the submission.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Committee Approval
This retrospective observational study followed the 1975 Declaration of Helsinki and obtained the ethical approval of the Medical Ethical Committee of the General Hospital of Northern Theater Command (Y (2023) 028).
Informed Consent
The requirement for informed consent for this study was waived.