
Abstract
Background
Although racial disparities in lung cancer incidence and mortality have diminished in recent years, lung cancer remains the second most diagnosed cancer among US Black populations. Many factors contributing to disparities in lung cancer are rooted in structural racism. To quantify this relationship, we examined associations between a multidimensional measure of county-level structural racism and county lung cancer incidence and mortality rates among Black populations, while accounting for county levels of environmental quality.
Methods
We merged 2016-2020 data from the United States Cancer Statistics Data Visualization Tool, a pre-existing county-level structural racism index, the Environmental Protection Agency’s 2006-2010 Environmental Quality Index (EQI), 2023 County Health Rankings, and the 2021 United States Census American Community Survey. We conducted multivariable linear regressions to examine associations between county-level structural racism and county-level lung cancer incidence and mortality rates.
Results
Among Black males and females, each standard deviation increase in county-level structural racism score was associated with an increase in county-level lung cancer incidence of 6.4 (95% CI: 4.4, 8.5) cases per 100,000 and an increase of 3.3 (95% CI: 2.0, 4.6) lung cancer deaths per 100,000. When examining these associations stratified by sex, larger associations between structural racism and lung cancer rates were observed among Black male populations than among Black females.
Conclusion
Structural racism contributes to both the number of new lung cancer cases and the number of deaths caused by lung cancer among Black populations. Those aiming to reduce lung cancer cases and deaths should consider addressing racism as a root-cause.
Introduction
Overall lung cancer incidence and mortality rates, and associated racial disparities between Black and White populations, have declined in the United States in recent years.1-3 However, lung cancer remains the second most diagnosed cancer type in Black populations in the US. 1 Additionally, racial disparities in lung cancer treatment persist, 4 and Black males continue to experience the highest burden of lung cancer incidence and mortality.1,3,5 To understand and address these persistent disparities in morbidity and mortality, we must account for the various socio-ecological factors that impact how lung cancer manifests across populations. One of these factors is structural racism, which refers to the intersecting and reinforcing ways that multiple macro-level systems (i.e., healthcare, education, economic, housing, judicial, political, neighborhood environment/design, media) ideologies, and practices converge to reinforce inequality that privilege whiteness; to the point where the inequitable distributions of resources and power become normalized.6-8 Structural racism may therefore represent a key characteristic of the social context influencing a variety of social determinants of health and population-level health outcomes, including lung cancer incidence and mortality rates. 9
As individual, interpersonal, social, and structural factors are interacting and reciprocal, the social environment in which people live influences behaviors and exposures that can result in disease.10,11 For example, studies also show that although Blacks smoke fewer cigarettes than Whites, Black people continue to have higher incidence of lung cancer. 12-14 Although the use of combustible tobacco products is the strongest behavioral determinant of lung cancer,15,16 individual smoking behaviors are influenced by a number of structural factors including social position, targeted advertising, strategic influence of industry within communities, local policies, and environmental characteristics, which have been shown to impact race groups differently.17-19 Additionally, the social patterning of tobacco use has been linked to stress among African Americans. 20 A mediation study examining the relationship between socioeconomic disadvantage, stress, and tobacco use found that African Americans reported greater daily stress than non-African Americans and that greater stress was associated with higher cigarette use. 20 Often used as proxies for structural racism, racial discrimination, or systematic disadvantage, in terms of interpersonal racism or living in environments with lower socioeconomic characteristics, have been documented as being associated with elevated levels of chronic and cumulative stress, with higher exposures among Black populations.21,22 Chronic stress, measured via allostatic load, has been associated with lung cancer, particularly among males.23,24 Other studies have suggested that higher levels of accumulated or chronic stress are associated with potentially more aggressive cancers.25,26 Thus, it is possible that structural racism increases Black peoples’ cumulative exposure to social, environmental, and structural stressors that subsequently contribute to their lung cancer incidence and death rates.
In addition to exposures from the social environment, exposures from the physical environment have been shown to impact cancer outcomes. Associations between lung cancer and outdoor environmental exposures are well documented. 27 However, exposures to environmental hazards are not evenly distributed across the population. In the US, because of structural racism, environmental pollution is racially segregated; causing Black and other minoritized populations to encounter greater exposures to environmental carcinogens.28-30
Exposure to these various stressors or carcinogens is socially patterned and demonstrates the multiple and compounding ways structural racism can accumulate and become embodied in individuals belonging to racially minoritized groups, resulting in population-level disparities in cancer outcomes. 31 In the US, race reflects social stratification categories that imbue conditions that influence a person’s chances of maintaining optimal health. 32 This is conceptually understood but not well measured.6,33,34 Quantifying how the embedded political, ideological, and social manifestations of structural racism are associated with cancer outcomes can help identify and inform how to intervene on the systems that contribute to perpetuating inequitable distributions of illness.
Until recently, studies attempting to account for the effects of structural racism on cancer outcomes have relied on single-dimension measures such as residential segregation. 35 For example, several studies on structural racism and lung cancer have found higher levels of residential segregation to be associated with greater mortality, and poorer treatment and survival outcomes among Black people compared to White.36,37 Meanwhile, other studies that used multidimensional indices of environmental quality to examine relationships between place-based environmental factors and cancer incidence did not explicitly examine racial differences. 38 Multidimensional indices have been noted as the most appropriate approach to attempt to assess structural racism.6,39 To our knowledge, only one study used a multidimensional index of structural racism and found county-level structural racism to be associated with increased all-cause cancer incidence and mortality rates. 40 However, examining the relationship between structural racism and site-specific cancer rates among Black populations is needed to inform more targeted intervention strategies.
Our study focused on lung cancer incidence and mortality rates among Black populations, using an ecological design. The objective of this study was to examine associations between a multidimensional measure of county-level structural racism and county lung cancer incidence and mortality rates among Black populations, while accounting for county levels of environmental quality.
Materials and Methods
Measures & Data Sources
Our key outcomes of interest were county-level lung and bronchial cancer incidence and mortality rates among Black male and female populations. These rates represent the average number of new lung and bronchial cases and deaths attributed to lung and bronchial cancer per 100,000 people, between 2016 and 2020. Publicly available county-level lung cancer incidence and mortality rates were gathered from the United States Cancer Statistics (USCS) Data Visualization Tool. 41 These data included the 2016-2020 age-adjusted 5-year incidence and mortality rates per 100,000 people for lung and bronchus cancers for US counties, adjusted to the 2000 US standard population. The county incidence rates data came from all US cancer registries except among states that prohibit the release of county-level data to outside entities (i.e., Kansas and Minnesota), states where county data were suppressed because of incompleteness (i.e., Virginia), and states who did not meet the USCS publication criteria during the reporting period (i.e., Indiana and Nevada). Mortality data come from the National Vital Statistics System which uses death certificate information to determine causes of death. Additional details about the cancer statistics used in our analyses can be found elsewhere. 42 Our study utilized de-identified publicly available datasets and did not require IRB approval.
Our primary independent variable of interest was the county-level standardized structural racism factor score. County-level structural racism data came from an existing multi-dimensional index developed by Siegel and colleagues. 43 Researchers constructed this factor score using confirmatory factor analyses to develop a structural racism index that quantifies Black and White disparities across five domains signifying societal systemic disadvantages Black people experience in the United States. The index domains include residential segregation, incarceration, unemployment, economic status/wealth, and educational attainment. 43 In the current analysis, structural racism factor scores ranged from −2.38 to 4.65; where counties with positive scores indicate greater than national average levels of structural racism and counties with negative scores indicate lower than national average levels of structural racism. Details on the development of the index can be found elsewhere. 43
To account for county levels of environmental quality, data on county measures of environmental quality were taken from the United States Environmental Protection Agencies (EPA) 2006-2010 Environmental Quality Index (EQI). 44 We included the five domains of the Environmental Quality Index: air quality; water quality; land use; the built environment; and sociodemographic environment. Each domain comprises multiple variables that represent hazardous or poor conditions that are not conducive for health. The air quality domains included 43 variables representing hazardous air pollutants. The water quality domain includes 51 variables assessing water contamination, waste, drinking and domestic use water quality, atmospheric deposition, and drought. Land use includes 18 variables representing agricultural activity, pesticide use, facilities, radon zones, and mining activity. The built environment domain is comprised of 15 variables measuring a range of factors related to transportation, subsidized housing, walkability, green space, food, recreation, and education facilities. The sociodemographic domain includes 12 variables accessing education, employment, poverty, housing values, vacancy, and tenancy household income, income inequality, crime, creative class employment, and political valence. Lower index scores represent better environmental quality, whereas higher values represent worse quality. Details on the development and composition of the EQI and its respective domains are published elsewhere. 45
The 2023 County Health Rankings data were used to capture county-level behavioral and healthcare access statistics associated with lung cancer, specifically adult smoking rates, access to healthcare, and rurality. 46 Smoking rates were measured as the percentage of adults who were current cigarette smokers, taken from the 2020 Behavioral Risk Factor Surveillance System (BRFSS). We also accounted for the percent of adults ages 18-64 without health insurance, taken from the 2020 US Census Bureau’s Small Area Health Insurance Estimates, and the primary care physician to population ratio taken from the 2020 Area Health Resource File. We also accounted for the percent of the county population living in rural areas, taken from the 2010 US Census.
Finally, because of the potential prolonged period between exposures and cancer diagnosis, we estimated the level of geographic mobility within counties, by creating a variable for the percentage of the county population that lived in a different county in the past year. These data were taken from the 2015-2019 US Census American Community Survey. 47
Analysis
The aforementioned datasets were linked using the Federal Information Processing System (FIPS) Codes for US Counties, which were included in each dataset. Our primary analytic sample included US counties with data on lung cancer rates, scores from the structural racism index, and scores from the EQI. Given differences in cancer and lung cancer rates by sex,48,49 we examined the county lung cancer incidence and mortality rates for males and females separately, among Black populations. We conducted the same descriptive analysis among counties that were excluded from our analytic sample (i.e., those with lung cancer data, but without structural racism or environmental quality scores), and performed t-tests to determine if there were substantive differences in lung cancer rates among counties in our analytic sample and those not included in our analyses. There were no statistically significant differences in the incidence and mortality rates among counties in our analytic sample and the counties with data on lung cancer rates but missing data for structural racism or environmental quality.
To examine associations between county-level structural racism and county lung cancer incidence and mortality rates among Black populations, we utilized linear regression analyses. First, we conducted bivariate analyses to explore the relationship between structural racism factor scores and lung cancer incidence and mortality rates. Then we conducted multivariable linear regression analyses to account for county environmental quality using EQI scores, and then EQI score and the percentage of adult smokers, the percent of adults without health insurance, the primary care physician to population ratio, the percent of the population living in rural areas, and our measure of county-level of geographic mobility. The adult smoking, adult uninsured percentage, and physician-to-population ratio were centered at the mean level for all counties with lung cancer incidence and mortality data. We present beta coefficients and 95% confidence intervals. All analyses were conducted using STATA.18 statistical software. 50
Results
2016-2020 Average US County-Level Lung Cancer Incidence and Mortality Rates for Non-Hispanic Black Populations.
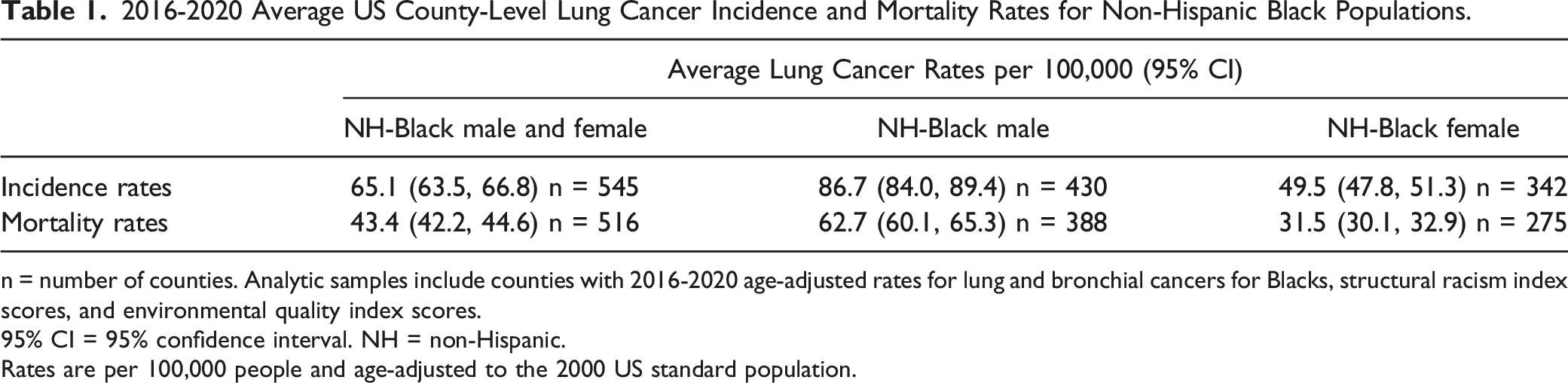
n = number of counties. Analytic samples include counties with 2016-2020 age-adjusted rates for lung and bronchial cancers for Blacks, structural racism index scores, and environmental quality index scores.
95% CI = 95% confidence interval. NH = non-Hispanic.
Rates are per 100,000 people and age-adjusted to the 2000 US standard population.
Descriptive Characteristics of US Counties in Study Sample (N = 545).

N = number of counties in sample. Analytic sample includes counties with 2016-2020 age-adjusted incidence rates for lung and bronchial cancers for Blacks, structural racism index scores, and environmental quality index scores.
Sd = standard deviation. NH = non-Hispanic.
Structural Racism Index factor scores represent the number of standard deviations that a particular county’s structural racism score is away from the mean for all counties.
EQI Domain Index scores represent average quality measures of the domains for each US county, higher scores indicate poorer environmental quality.
Geographic mobility represents the percent of the population not living in the county 1 year ago.
Primary care physician-to-population ratio represents the number of individuals served by one physician in a county (i.e., 2500:1).
Linear Regression Analyses of Associations Between County Level Structural Racism and 2016-2020 County Lung Cancer Incidence Rates Among Black Populations.

n = number of counties. 95% CI = 95% confidence interval. EQI = Environmental Quality Index. NH = non-Hispanic.
Rates are per 100,000 people and age-adjusted to the 2000 US standard population.
Model 1 presents bivariable linear regression results of the association between county lung cancer incidence rates and structural racism index factor score.
Model 2 presents multivariable linear regression results, accounting for each Environmental Quality Index Domain.
Model 3 presents multivariable linear regression results, accounting for each Environmental Quality Index Domain and adjusting for county levels of adult smoking, uninsured adults, primary care physician to population ratio, the percent of population living in rural areas, and county geographic mobility.
Bold values indicate statistically significant associations between the correlate at lung cancer incidence rates, at a 95% confidence level.
Linear Regression Analyses of Associations Between County Level Structural Racism and 2016-2020 County Lung Cancer Mortality Rates Among Black Populations.
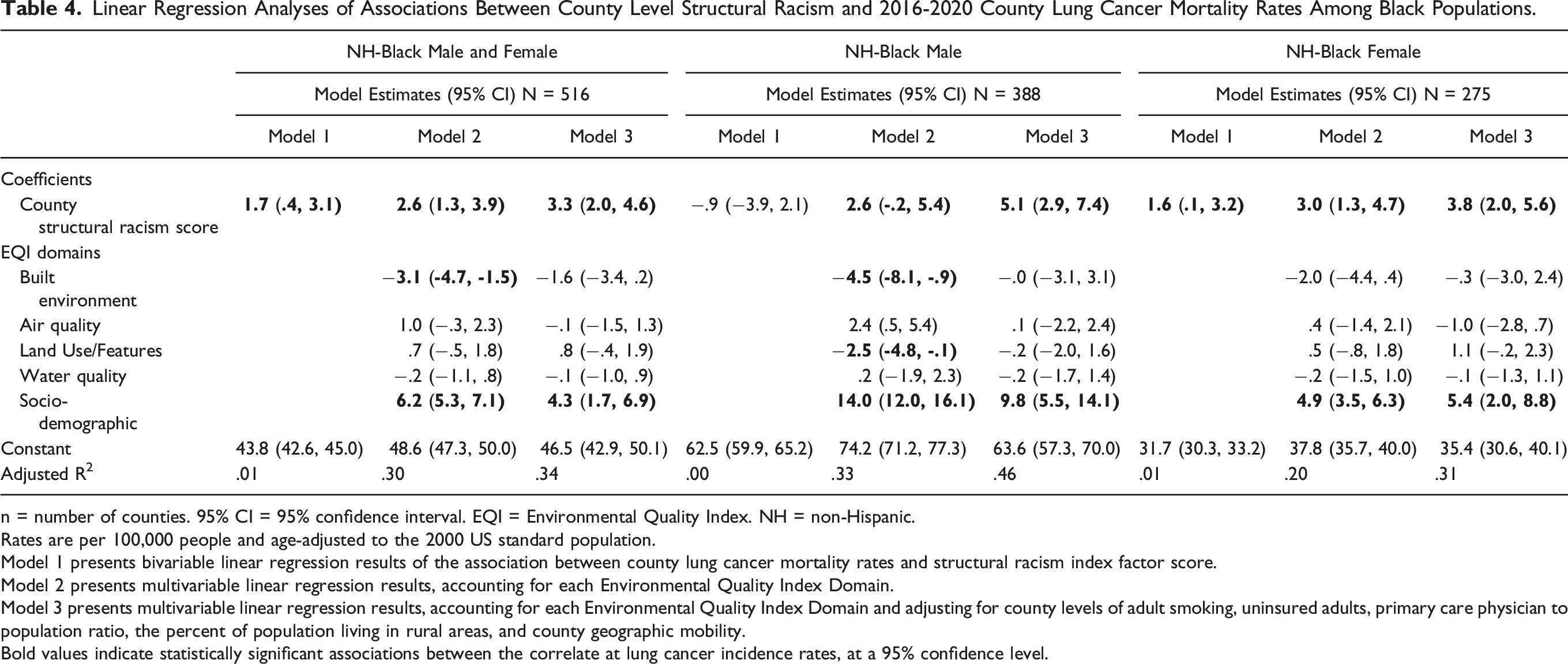
n = number of counties. 95% CI = 95% confidence interval. EQI = Environmental Quality Index. NH = non-Hispanic.
Rates are per 100,000 people and age-adjusted to the 2000 US standard population.
Model 1 presents bivariable linear regression results of the association between county lung cancer mortality rates and structural racism index factor score.
Model 2 presents multivariable linear regression results, accounting for each Environmental Quality Index Domain.
Model 3 presents multivariable linear regression results, accounting for each Environmental Quality Index Domain and adjusting for county levels of adult smoking, uninsured adults, primary care physician to population ratio, the percent of population living in rural areas, and county geographic mobility.
Bold values indicate statistically significant associations between the correlate at lung cancer incidence rates, at a 95% confidence level.
Discussion
In this study we examined the relationship between a multi-dimensional index that attempts to quantify structural racism at the county level and county lung cancer incidence and mortality rates among Black populations, in the United States. We found that higher county structural racism index scores were associated with statistically significant higher county lung cancer incidence and mortality rates among Black populations overall, and that the associations were stronger after accounting for county environmental quality, including sociodemographic characteristics, and other factors related to lung cancer. Specifically, among Black males, every standard deviation increase in county structural racism score was associated with 8.1 additional new lung cancer cases and 5.1 additional lung cancer deaths per 100,000. Our results suggest that structural racism is a contributor to both the number of new lung cancer cases and the number of deaths caused by lung cancer among Black populations.
This study adds to the existing body of research which has demonstrated how communities’ social characteristics influence the health of the people residing there. In the context of lung cancer specifically, several studies have highlighted how higher amounts of residential segregation, and neighborhood deprivation are associated with lung cancer incidence and mortality.37,51-54 These predictors are often considered indicators of structural racism, reflecting the contemporary and historical ways power and privilege have systematically limited access to resources, particularly for Black people in the United States. Our findings align with this previous work. Studies examining racial disparities in lung cancer have noted a variety of contributing factors including adverse social determinants of health and inequities in receipt of guideline concordant treatment for lung cancer, healthcare utilization, and clinical trial participation, among Black people compared to Whites.5,9,55 However, these factors are rooted in historical and contemporary ideologies, practices, and policies that disadvantage certain race groups (i.e., structural racism). Thus, assessing the role of structural racism as a root cause of lung cancer disparities further illuminates it as a key determinant and helps move towards the eradication of racism and other connected systems of oppression that promote poor health. Our study advances this body of research through the inclusion of a structural racism index that explicitly captures race-based differences across multiple social determinants of health at a population level, while also accounting for the overall quality of social and physical environment, through the numerous variables represented in the Environmental Quality Index.
However, this study has some potential limitations. As this study was conducted at the county-level rather than an individual level our estimates of lung cancer incidence and mortality rates differ from other national estimates. The data used in our analyses reflect the average annual adult age-adjusted rate of lung cancer incidence or mortality in a given county from 2016 to 2020. Our descriptive reporting of lung cancer incidence and mortality among all races and Black populations are higher overall than what is reported elsewhere,41,56 but follow the same pattern as the other reports. It is possible that variability in state-level political and social context may have also influenced county-level outcomes. However, our analyses did not account for this. Our analytic sample included the 545 and 516 counties with structural racism index scores, environmental quality index scores, and lung cancer incidence and mortality rates for Black populations, respectively. Although this only reflects a sample of the total 3143 US counties, the counties included in our incidence analyses had combined populations of 159,000,000, and populations of 166,000,000 for our mortality analyses. The 2021 US population was 331,900,000, so the counties included in these analyses had populations that represent half of the total US population. With this in mind, our ecological study design presents a valid and fairly representative way of examining a macro-level exposure (i.e., structural racism) on population-level outcomes.
The goal of cancer control is to reduce the incidence, morbidity, and mortality of cancer in a defined population. 57 Fortunately, as tobacco use rates continue to decline in the US, we also observe parallel declines in lung cancer incidence. While it is critically important to continue ongoing work to advance this downward trend, our analysis highlights some potential other factors that may contribute to both lung cancer incidence and mortality, particularly in populations with persistently higher rates (i.e., Black males). Our study shows that the systems comprising the structural racism index used in our analysis (i.e., housing/residential segregation, incarceration, employment, economic, education) are more strongly associated with adverse lung cancer rates among Black male populations. Existing research on how these different systems unjustly target Black males is often found in disparate fields of study and practice. Future research and practice aiming to address disparities in cancer among Black populations should consider how these and other systems, such as healthcare, reinforce inequalities by privileging whiteness, and how this varies by gender and across the life course. This study represents a step towards further illuminating the detrimental impacts of racial oppression by employing measures that explicitly examine the extent of racial disparities for key social determinants of health, across geographies. As measures of structural racism become more refined, we anticipate that they will help to elucidate how racism operates, but also point to areas for intervention. Additionally, by linking them to specific health outcomes (cancer) we may be able to galvanize a wider variety of stakeholders who will advance efforts to address the various ways racism operates within our social systems.
Conclusion
Race refers to social rather than biological categories, forged by systems of oppression.58,59 Structural racism is a system of oppression that can be considered a cause of causes, reflecting the embedded conditions that lead to many of the disparities observed between race groups. Although individual and community level socioeconomic status intersects with race, the use of socioeconomic measures alone to understand racial disparities in health is insufficient. This is seen in the fact that racial disparities in health remain even after accounting for socioeconomic status. 60 This study contributes to the literature that examines racism as a determinant of disparities in lung cancer incidence and mortality. Our intention is that this study will stimulate additional research and promote the development of interventions that target systems and structural-level drivers of cancer disparities. Doing so will require a willingness to critically question how all aspects of the work to advance cancer control may or may not uphold systems of racism and white supremacist ideologies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors of this manuscript were supported by the following funding. Dr. Robinson-Oghogho was supported by the Cancer Epidemiology, Prevention, and Control Training Program NCI grant T32 CA009314. Dr. Alcaraz was supported by NCI grant P30CA006973. Dr. Thorpe was supported by NIA K02AG059140, DP1AG069874, and NIMHD U54MD000214. The funding entities had no role in the study design, analysis, or writing of this publication.
Ethical Statement
Data Availability Statement
The county structural racism index data that support the findings of this study are available from the corresponding author, JNRO, or the original study author upon reasonable request. The data that support the findings of this study were derived from the following resources available in the public domain: • United States Cancer Statistics (USCS) Data Visualization Tool - https://www.cdc.gov/cancer/uscs/dataviz/download_data.htm • United States Environmental Protection Agencies (EPA) 2006-2010 Environmental Quality Index (EQI) - https://www.epa.gov/healthresearch/environmental-quality-index-eqi • 2023 County Health Rankings and Roadmap - https://www.countyhealthrankings.org/explore-health-rankings/rankings-data-documentation • 2015-2019 US Census American Community Survey Geographic Mobility Data – https://data.census.gov/table/ACSDT5Y2019.B07204?q=B07204:+GEOGRAPHICAL+MOBILITY+IN+THE+PAST+YEAR+FOR+CURRENT+RESIDENCE--STATE,+COUNTY+AND+PLACE+LEVEL+IN+THE+UNITED+STATES