
Abstract
Background
COVID-19 forced a delay of non-essential health services, including lung cancer screening. Our institution developed a single-encounter, telemedicine (SET) lung cancer screening whereby patients receive low-dose CT in-person, but counseling regarding results, coordination of follow-up care and smoking cessation is delivered using telemedicine. This study compares outcomes of SET lung cancer screening to our pre-COVID, single-visit, in-person (SIP) lung cancer screening.
Methods
A retrospective cohort study was performed we recorded independent variables of gender, race/ethnicity, age, educational attainment, smoking status and dependent variables including cancer diagnosis, stage and treatment between March 2019 to July 2021. Using retrospective analysis, we compared outcomes of SIP lung cancer screening before COVID-19 and SET lung cancer screening amid COVID-19.
Results
There was a significant difference in number of patients screened pre- and amid COVID-19.673 people were screened via SIP, while only 440 were screened via SET. SIP screening consisted of 52.5% Black/African American patients, which decreased to 37% with SET lung cancer screening. There was no significant difference in gender, age, or educational attainment. There was also no significant difference in Lung–RADS score between the 2 methods of screening or diagnostic procedures performed. Ultimately telemedicine based screening diagnosed fewer cancers, 1.6% diagnosed via telemedicine vs 3.3% screened by in person.
Conclusion
We implemented SET lung cancer screening to continue lung cancer screening during a global pandemic. Our study established feasibility of telemedicine-based lung cancer screening among our predominantly African American/Black population, though fewer patients were screened. We found no difference in distribution between age, or educational attainment suggesting other factors discouraging lung cancer screening amid COVID-19.
Introduction
Lung cancer screening with low dose computed tomography (LDCT) decreases lung cancer death by 20-26%.1-3 There is also a well-known health care disparity in the treatment of lung cancer with African American patients being disproportionately affected. 4 Furthermore, African American patients are more likely to be diagnosed at a more advanced stage compared to white patients, and have the highest incidence as well as mortality related to lung cancer. This is coupled with the lowest rates of treatment. 5 The CHEST expert panel report for lung cancer screening during COVID stated it was “Appropriate to defer enrollment in LCS…due to the added risk from potential exposure”. In order to resume lung cancer screening, our program had to address limited radiologic services, reduced clinic and personnel resources as well as the need to minimize risk of COVID-19 exposure to patients and care providers. We aspired to preserve our Single-visit, In-Person (SIP) lung cancer screening protocol developed to facilitate access for our underserved population. 6 Amid COVID-19, we developed a Single-Encounter Telemedicine (SET) lung cancer screening whereby eligible patients receive LDCT in our radiology facility and return home for a telemedicine visit that includes discussion of results, coordination of follow-up care and smoking cessation counseling on the same day. This study sought to examine performance of SIP vs SET lung cancer screening in terms of uptake and screening outcomes. We hypothesized that there would be no difference between SIP vs SET lung cancer screening in terms of cancer detection or staging for patients diagnosed. Ours is the first study to report lung cancer screening among an underserved population during COVID-19 achieved through a novel use of telemedicine.
Material and Methods
Consent and study protocols were approved by Temple University Health System Institutional Review Board (Protocol #23085, 2014-2021). In a safety-net health system, 7 primary care physicians, pulmonologists and specialists referred patients for lung cancer screening. A trained nurse screened referred patients for study eligibility consistent with United States Preventive Services Task Force (USPSTF) 8 or National Comprehensive Cancer Network (NCCN) 9 guidelines for lung cancer screening, and eligible patients received informed written consent for collection of medical data, outcomes, and a patient survey.
Patients were consecutively enrolled from March 2019 to March 16, 2020 received SIP lung cancer screening. COVID-19 compelled a transition to telemedicine from March 16, 2020 to July 2021 using SET lung cancer screening, whereby eligible patients received LDCT scan within our radiology facility, but returned home for discussion of results, coordination of follow-up care and smoking cessation with a lung cancer screening specialist within the Department of Thoracic Medicine and Surgery. (Figure 1) study size was based on patient enrollment in the lung cancer screening program. Visual abstract for single- encounter telemedicine (SET) lung cancer screening reveals lower rates of screening but preserves access to minorities.
Radiologists interpreted LDCT using Lung-Reporting and Data System (Lung-RADS) during this visit. 10 Patients with lung-RADS category 0 received coordination of a repeat CT scan. Patients with Lung-RADS category 1 and 2 interpretations, defined as negative screens, received recommendation for annual lung cancer screening. Patients with Lung-RADS 3 or 4, defined as positive screens, discussed results with the lung cancer screening specialist who arranged follow-up care including additional imaging, diagnostic procedures and consultations with pulmonology, interventional radiology, thoracic surgery, medical oncology, radiation oncology, and palliative care given that one of our primary results was based on objective radiographic findings, we did not feel that there were any obvious potential sources of bias that had to be addressed for this study.
We recorded independent variables of age, gender, race, highest educational attainment, smoking status and smoking history in terms of pack years using a patient survey completed with a research nurse. All patient details were de-identified so that the identity of any person could not be ascertained. The dependent variable of Lung-RADS interpretation was measured. For those with Lung-RADS category 3 or 4, follow-up care including diagnostic imaging, diagnostic procedure, type of procedure (CT guided biopsy, Endobronchial Ultrasound (EBUS)-guided biopsy, surgery), lung cancer diagnosis, stage of cancer diagnosed, early (I/II) vs late (III/IV) stage, lung cancer treatment, treatment option (radiation, surgery, chemotherapy or combination), major complications, complication type and mortality were evaluated. Patient-reported and electronic medical record (EMR) documentation of major complications, defined by NLST supplementary appendix, 1 were recorded. Mortality was measured by review of EMR and Social Security Death Index. The reporting of this study conforms to STROBE guidelines. 11
Statistical Analyses
We retrospectively analyzed and compared SIP and SET lung cancer screening participants using Chi-square test, and Student T-test; P value < .05 was considered significant.
Results
Between March 2019- March 16, 2020, 673 patients were screened with SIP lung cancer screening. From March 16, 2020 - July 1, 2021, 440 patients were screened using SET lung cancer screening. (Figure 2) From March 2019 - March 2020 prior to COVID-19 shutdown, an average of 52 patients received SIP lung cancer screening per month. From March 2020 - July 1, 2021, an average of 26 patients received SET lung cancer screening per month. There were significantly fewer patients screened via SET lung cancer screening compared to SIP. Number of Patients Screened Via SIP (Pre-Pandemic) compared to SET LCS.
Patient characteristics of lung cancer screening participants.

Lung cancer screening results and diagnostic procedures as a result of screening.

Lung cancer diagnosis and treatment as a result of lung cancer screening.
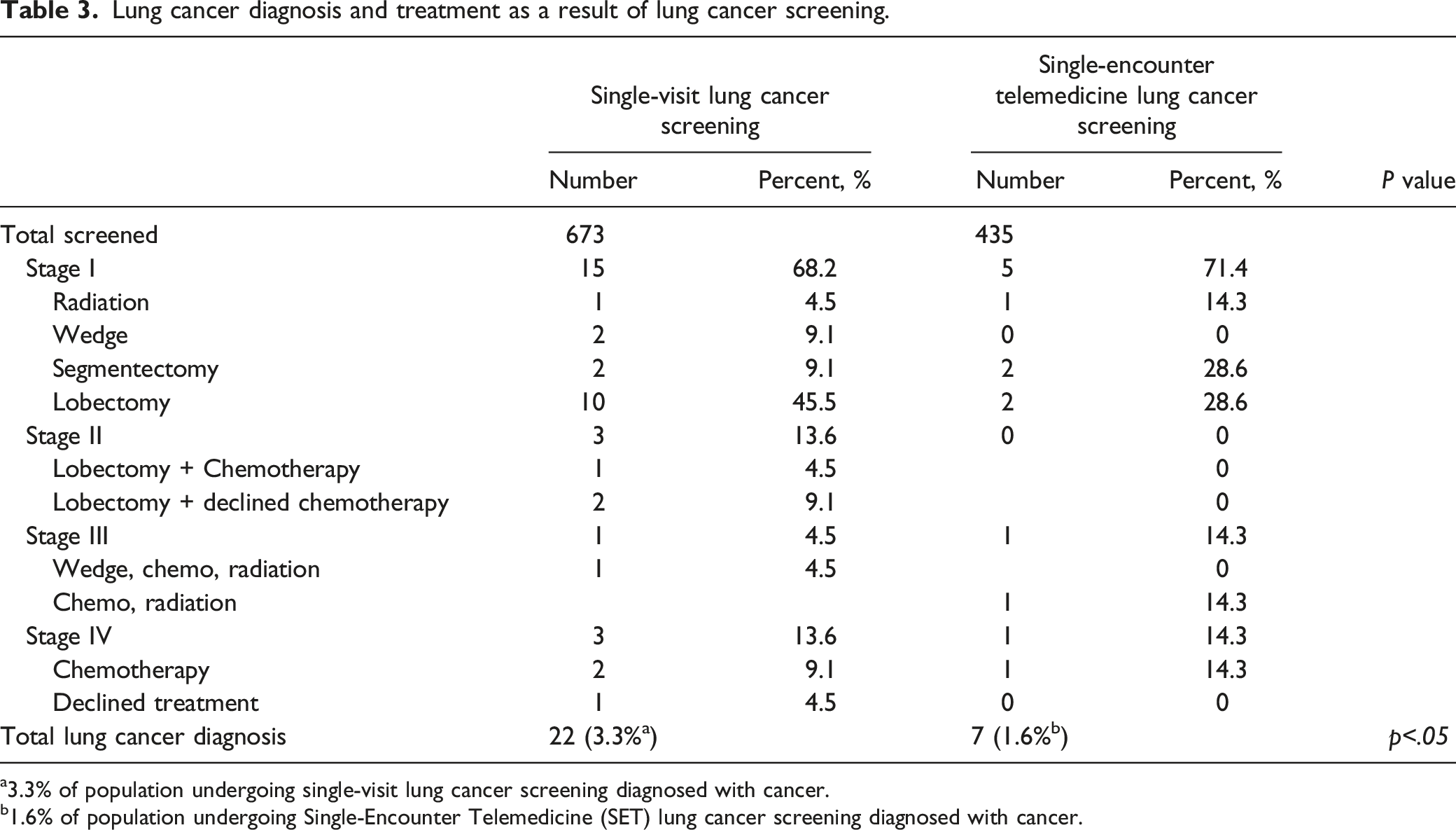
a3.3% of population undergoing single-visit lung cancer screening diagnosed with cancer.
b1.6% of population undergoing Single-Encounter Telemedicine (SET) lung cancer screening diagnosed with cancer.
For people undergoing SIP lung cancer screening, 54 people had positive screens (Lung-RADS 3 or 4) but did not receive a lung cancer diagnosis. Two declined diagnostic procedures. One person died of sepsis, and 1 person died of a stroke before completion of diagnostic work-up. One person died after a diagnosis of metastatic lung cancer. One person who underwent segmentectomy for stage I lung cancer, had no complications from surgery but committed suicide 1 year after surgery. Overall mortality for those screened for lung cancer using SIP was .6% with only .1% attributable to lung cancer. The follow-up of SET participants is not comparable to those undergoing SIP because of the lack of time for interval follow-up. However, of people undergoing SET lung cancer screening, 1 major complication of a pneumothorax requiring chest tube placement and hospitalization occurred after CT guided biopsy. There were no procedural or treatment-related deaths as of the time of this report. One person undergoing SET lung cancer screening has declined further diagnostic work-up. This proportion (.4%) is not significantly different from the 4 (.4%) failing to participate in diagnostic work-up with SIP lung cancer screening.
Discussion
Health Disparities of Populations at Risk for Lung Cancer
Lung cancer remains the most common cause of mortality in the US. 12 Studies have found that certain groups are disproportionately affected by lung cancer, namely black patients, and those from socioeconomically disadvantaged groups.13,14 Black/African American patients are known to be affected by lung cancer at a higher incidence than white patients, be diagnosed at a later stage, have lower rates of treatment and have higher rates of mortality. 15 Lung cancer screening confers a 20-26% reduction of death 1 with Black/African American benefiting more than other racial groups. Recent recommendations of United States Preventive Task Force Services and Center for Medicaid and Medicare for lung cancer screening will likely increase the number of Black/African Americans eligible for screening.16,17 However, uptake in this population is particularly low. 18 The barriers to lung cancer screening such as access to health care, health care literacy, and trust in the healthcare system disproportionately impact populations from lower socioeconomic groups.19,20 Added to these known disparities, the global COVID-19 pandemic further exacerbated existing health care disparities. 20
Response to COVID, an Added Barrier to Lung Cancer Screening
In the spring of 2020 the Center for Disease Control recommended deferring all non-urgent healthcare to minimize risk of COVID-19 exposure and propagation. Guidelines from CHEST Expert Panel also supported delay of screening during the COVID-19 pandemic, but failed to suggest criteria for resumption of screening. 21 Relying on data from our lung cancer screening experience, we predicted that failure to screen 600-700 patients per year at our institution would result in missed opportunity to diagnose and treat 12-14 lung cancer patients. 22 We expedited resumption of lung cancer screening by creating a telemedicine protocol and preserving our single visit concept. Lung cancer screening resumed at our institution by May 2020 using a single-encounter telemedicine (SET) model.
Feasibility of Telemedicine Counseling for Lung Cancer Screening
We proved feasibility of lung cancer screening using telemedicine counseling among our underserved population with 435 patients screened with SET between March of 2020 and July of 2021. Additionally, we demonstrated feasibility among our Black/African American patients as they comprised the largest racial demographic (37.3%). We successfully detected early lung cancer with few complications. Our study demonstrates that the stage of detection is not significantly different using 2 different screening paradigms. This differs from others demonstrating more advanced cancer detected with screening during the pandemic. 23 We did however find that we diagnosed fewer patients with cancer via telemedicine based screening (3.3% vs 1.6%). It possible that with COVID-19 and its radiographic sequelae confounded interpretation of lung cancer screening studies. Nodule detection may be deferred with a repeat CT scan in the setting of infection or inflammation following COVID-19. This is particularly problematic among our population as we have reported poor follow-up after negative screening. 22
In our study there were no differences in compliance with follow-up care after positive lung cancer screening (Lung-RADS 3 and 4). Follow-up care after a positive screen is critical to decreasing lung cancer mortality. If patients do not adhere to follow-up care after a positive screen, they incur all the risks of screening such as false positives, over diagnosis, incidental finding, anxiety, but no potential benefit of lung cancer detection and treatment. 24 Further study into long-term outcomes of both SIP and SET lung cancer screening are needed to determine other screening outcomes including differences of false positive results and survival.
Patients with screen-detected cancer were all adherent to treatment including surgery, radiation and chemotherapy with exception of 1 patient diagnosed with metastatic cancer with SIP lung cancer screening. There was no significant difference in treatment choices with SIP lung cancer screening and SET lung cancer screening. There were no deaths or complications from diagnosis or treatment with exception of 1 patient participating in SET screening who had a pneumothorax after biopsy. Overall, the data suggest that care of patients after screening is not significantly different between SIP and SET.
Although we were able to preserve screening among Black/African American patients, uptake is still at an unacceptably low and will compound late diagnosis of lung cancer and increased mortality among Black/African Americans. Though we screened 435 patients with SET between March 2020 and July 2021, this was drastically lower than lung cancer screening using SIP protocol between March of 2019 to March of 2020 before the COVID-19 pandemic. Like other institutions that have reported reduction in screening. 18 We believe that health care providers in our safety-net health system experienced disproportionate limitations of healthcare resources during the pandemic, and declined or delayed referral for lung cancer screening.
Even if referred, patients failed to seek care for symptomatic illnesses, and were even more likely to decline care for lung cancer screening. 23 Additionally lung cancer screening patients are likely to have comorbidities that confer high risk for COVID-19, influencing their decision to decline lung cancer screening appointments. Declining lung cancer screening is consistent with other harmful health behaviors including low activity, alcohol and smoking. 24 Of note, 62.6% of those participating in SIP lung cancer screening before COVID-19 were active smokers compared to only 33% those participating in SET lung cancer screening during COVID-19 (p<.5). Further study into the reasons for this significant decline of active smokers participating in lung cancer screening is needed, especially as active smokers are more likely to benefit from screening than non-smokers. 25
Our study showed a decline in screening African American population enrollment in lung cancer screening. The exact cause of this is difficult to discern however we believe that this may be a reflection of the disproportionate effects of COVID-19 on African American population. 25 Additionally, other factors related to patients ease of accessing screening such as mode of transportation, and access to health care providers may have played a role in the decline in African American enrollment.
Previous studies have shown that Black/African American and Latino patients have lower rates of telemedicine utilization. 26 It remains unclear if the telemedicine based platform contributed to fewer patients screened overall, and if so, whether that was due to lack of access or familiarity to technology. We had initially hypothesized that telemedicine based platform may alienate older patients, less educated or those of lower socioeconomic groups based on results from other studies. 26 Based on our results there was no significant difference in the age groups screened with 60-64 years old being the majority in both groups. Likewise, there was no significant difference in the educational attainment of those screened between the 2 delivery methods with high school graduate or GED being the most screened, and no significant difference between patients with lower educational achievement levels. As previously stated Black/African American patients were disproportionally affected by COVID-19, thus a component of fewer patients screened may have been due to fear of exposure during LDCT. Future studies will focus on this and other potential barriers to lung cancer screening amid COVID-19.
In comparing our outcomes to previous published studies we found confirmation that halting screening altogether would have led to a backlog of patients, who would likely be screened at a more advanced stage. 23 Centers that shut down screening due to COVID-19 found decreases in new patients screened, and evidence of stage migration once screening resumed. One study found 818 screening visits cancelled, 40% “no-show” rate and 29% of patients with Lung RADS 4 compared to 8% pre-pandemic. 23 Our study provides an alternative form for screening that may help other centers continue to provide access to their patients.
Lastly, during this study, feasibility of telemedicine lung cancer screening and potential expense to patients were unknown. This uncertainty may have contributed to reluctance of referring physicians and patients to participate in lung cancer screening. Hopefully the results of this study will reassure health care providers and patients about the safety of telemedicine screening. We also believe that our study is reproducible at other institutions and applicable to other centers that provide lung cancer screening.
Study Limitations
Our study has limitations. In our comparison of SIP vs SET lung cancer screening, it is not known if differences are a result of the context of COVID-19, or the process of screening, namely in-person vs telemedicine. Future study of simultaneous in-person vs telemedicine would not only help define differences between the methods, but possibly further uptake of screening by offering the choice of both. Ours is a single institution study with limitations of a unique patient population and resources, which may not be applicable to other screening programs. Given limited resources during pandemic and hospital system further information regarding how many patients were offered screening was not available, making it difficult to comment on patient uptake of screening. Furthermore, more work is warranted in regards to patient experience with screening as well as ease of pursuing screening. An additional limitation to our study was that a power calculation was not performed. Finally, though our data identifies a disparity of SET lung cancer screening uptake among patients in the setting of COVID-19, our study was not designed to understand causes of disparity. Further, multi-level study is needed to understand mechanisms of this disparity.
Conclusion
In response to COVID-19, we implemented a single encounter telemedicine (SET) lung cancer screening paradigm with successful detection and treatment of lung cancer comparable to pre-COVID-19, single-visit, in-person (SIP) lung cancer screening (Figure 1). We were successful in engaging our predominantly Black/African Americans population, but overall fewer people participated in screening. Further study into barriers to screening amid COVID-19 are needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by TUFCCC/HC Regional Comprehensive Cancer Health Disparity Partnership, Award Number U54 CA221704(5) (Contact PIs: Grace X. Ma, PhD and Olorunseun O. Ogunwobi, MD, PhD) from the National Cancer Institute of National Institutes of Health (NCI/NIH). The content is the responsibility of the authors and does not represent the official views of the NCI/NIH. This study was partially supported by Pfizer-American Cancer Society Grant Addressing Systemic Race-Related Barriers that Contribute to Disparities in Care among Black Men and Women with Cancer (Contact PI: Cherie P. Erkmen, MD) The content is the responsibility of the authors and does not represent the official views of Pfizer or the American Cancer Society. Publication of this article was funded in part by the Temple University Libraries Open Access Publishing Fund
Ethics Statement
Consent and study protocols were approved by Temple University Health System Institutional Review Board (Protocol #23085, 2014-2021). Eligible patients received informed written consent.