
Abstract
Introduction
Breast and cervical cancers represent two important causes of cancer-associated deaths in females. Uptake in prevention towards these cancers remains low in the United Arab Emirates.
Objectives
This study aimed to understand the knowledge, attitudes and practices of females residing in the Al Ain city, UAE, towards cervical and breast cancer prevention.
Methods
This cross-sectional survey was conducted with 300 women, aged 30 years and above. The primary outcome measure was cervical and breast cancer prevention knowledge. The knowledge was queried through a number of items, with the resulting aggregate scores categorized into good and low knowledge. Chi-square test was conducted to investigate the association between prevention knowledge and sociodemographic factors. Additional outcomes included attitude towards and uptake of cervical and breast cancer screening.
Results
Of the participants surveyed, 36.7% had good knowledge on breast cancer prevention, while 5.3% on cervical cancer prevention. Although the majority of the participants believed that prevention methods could save lives, they reported negative attitudes, considering screening unnecessary and painful. The self-reported screening uptake was 23% and 31.3% for mammography and Pap smear, respectively.
Conclusions
The study reported that the knowledge and uptake of women was low for both breast and cervical cancer prevention. Targeted campaigns not only to increase knowledge but also to resolve misconceptions to change negative attitudes may lead to an increase in uptake.
Introduction
Two leading causes of cancer-associated morbidity and mortality among women globally are breast and cervical cancers. Breast and cervical cancer are ranked as the first and fourth causes of cancer-associated deaths, respectively, among women worldwide. Although the age-standardised incidence (45.5/100,000 for breast cancer and 6.2/100,000 for cervical cancer) and mortality (16.6/100,000 for breast cancer and 3.5/100,000 for cervical cancer) rates in the Middle East and North Africa (MENA) region as estimated in 2020 1 are lower than other WHO regions, evidence suggests that women present at very advanced stages of the disease and at younger age.2-4 Advancements in health research have led to the development of several prevention options that have reduced the burden of these cancers significantly. Modalities such as breast self-examination (BSE), clinical breast examination (CBE) and mammography can lead to early detection of breast cancer, thus preventing mortality.5,6 In the UAE, it is recommended for women aged 40–69 years to have clinical breast examination annually and mammography every two years. 6 Similarly, for cervical cancer prevention, options such as Papanicolaou (Pap) smear, that is, microscopic examination of abnormal cells, Human Papilloma Virus (HPV) test and HPV vaccination (HPVV) have been introduced. In the United Arab Emirates (UAE), Pap smear is offered to sexually active women aged 25–49 years every three years and those of 50–65 years every 5 years. 7 Whereas the vaccination is available for women aged 13–26 years. Despite the opportunistic availability of these options in the UAE, participation of women remains low, that is, 13.9% for mammography and 28.0% for Pap smear. 8
Evidence suggests that knowledge and perceptions about preventive health increase the likelihood of practice and health services uptake. 9 It is therefore essential to have proper knowledge and positive behaviour for the perusal of preventive health activities. Studies have been carried out previously in certain Gulf Cooperation Council (GCC) countries such as Qatar, Oman, Saudi Arabia and Jordan to understand breast and cervical screening knowledge and uptake among women populations.10-12 Few studies conducted in the UAE suggest mixed results indicating low-moderate levels of breast screening knowledge about BSE, CBE and mammography among women.13,14 Similarly, limited studies carried out on assessment of cervical cancer and its screening knowledge in the UAE indicate low awareness and uptake levels in the women as well as the health care practitioners (HCPs).15-17 Similar findings on awareness and uptake of HPVV were reported. 18 This cross-sectional study was conducted to understand knowledge, attitude and practices of women living in Al Ain, UAE, towards breast and cervical cancer prevention, including screening as well as HPV vaccination.
Methods
Participant Recruitment and Sample Size Estimation
This observational cross-sectional study is being reported in conformation with STROBE guidelines. 19 It was conducted with participants that were conveniently sampled from waiting areas of primary health care clinics in the city of Al Ain during 2016. Women aged 30 years and above, able to speak English or Arabic, from Emirati as well as non-Emirati background and able to provide consent were eligible.
Adequate sample for this study was statistically estimated using sample size estimation formula for prevalence study with absolute precision, n = z 2 p (1−p)/d 2 , where n is the estimated sample size, p is the expected prevalence of people with good knowledge of breast cancer, obtained from a similar study, 20 and d is the desired margin of error. The value of z used was 1.96 (at a 5% level of significance); anticipated prevalence of BSE practice of 23% as reported by a study in the region by Ravichandran et al 20 was used and margin of error was pegged at 5 percentage points. The calculated sample size was 276. The final sample size was rounded up to a total of 300 participants in order to accommodate for anticipated non-response. Ethical approval for the study was taken from Ambulatory Health Services (AHS) Ethics Research Committee.
Data Collection Measures
Data was collected using a structured survey (refer to the Supplementary Material) developed after careful literature review. It was based on validated tools such as breast and cervical cancer awareness measures (CAM), and questionnaires used in previous studies,20-23 tailored according to recommendation of breast and cervical screening within the UAE.6-8 It consisted of four sections: The first section addressed questions on sociodemographic (age, marital status, residence, nationality, residence, socioeconomic and educational status) and health related (pre-existing medical conditions, medication and alternative medicine usage history, family history of cancer, regular visit to a doctor and previous invitation by a doctor for screening test) characteristics. The next section assessed their breast cancer prevention knowledge (screening, i.e. BSE, CBE and mammography), practices (uptake and doctor’s recommendation) and attitudes. It was followed by a section on cervical cancer prevention knowledge (Pap smear and HPVV), practices (uptake of screening and doctor’s recommendation of screening and vaccination) and attitudes. The last section enquired about the participants’ sources of information on prevention of both cancers. The main outcome measures were breast and cervical cancer prevention knowledge, uptake and attitudes. The questionnaire was reviewed by experts and pilot tested by 10 participants to ensure clarity, readability and cultural suitability, followed by use for actual data collection. Data was collected by medical students verbally and face to face from participants after obtaining written consent from participants. The details of participants were de-identified, and the identity of any participant could not be ascertained in any way.
Data Analysis
Descriptive statistics were used to summarize variables including the characteristics of the participants, those related to attitude towards cancer screening and practice of cancer screening, among others. Using descriptive analysis, categorical variables were summarized by frequencies and percentages while continuous variables were presented as mean and standard deviation. Knowledge of breast and cervical cancers was computed separately. Each knowledge item question was assigned a score of 1 if correctly answered. Overall scores were then computed by adding all the scores for each participant. The total scores were further computed by calculating the percentage score for each participant. A percentage score of 50 and above was regarded as having good knowledge and otherwise was considered low knowledge for both breast and cervical cancers. Participants with incomplete data were excluded from the analysis. The categories of knowledge were summarized and presented as frequencies and percentages. Further inferential statistics were employed to investigate the association between knowledge of breast and cervical cancers with sociodemographic factors. Chi-square test and Fisher’s exact test were used for the purpose as appropriate.
Results
Demographic Characteristics of the Participants
Demographic Characteristics of Respondents (N = 300).

Knowledge of Breast and Cervical Cancers
Breast and Cervical Cancer Prevention Knowledge Among the Participants.
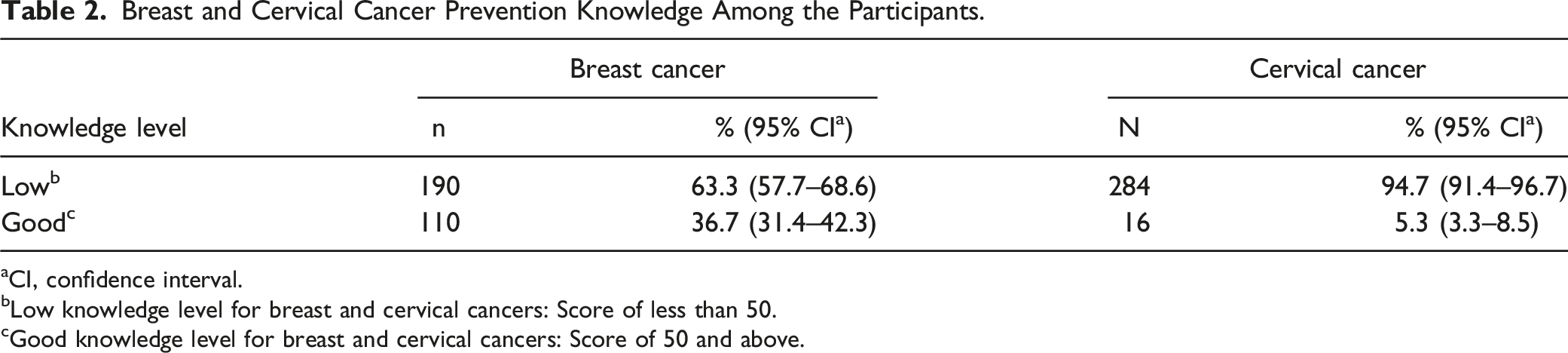
aCI, confidence interval.
bLow knowledge level for breast and cervical cancers: Score of less than 50.
cGood knowledge level for breast and cervical cancers: Score of 50 and above.
Summary of Responses to Breast and Cervical Cancer Prevention Knowledge Testing Questions (N = 300).

Association Between Demographic Factors and Breast and Cervical Cancer Knowledge.

aLow knowledge level: Score of less than 50.
bGood knowledge level: Score of 50 and above.
cP value statistically significant: ≤0.05.
Attitude
Most of the participants showed positive attitudes regarding the importance of doctor visits for a regular breast health exam (78.3%), lifesaving ability of early screening and early detection of breast cancer (84.4%) as they agreed with these statements (Figure 1). A considerable proportion of the participants showed a poor attitude towards mammogram as they agreed that a mammogram can cause unnecessary fear and panic among women (56%), a mammogram is a waste of resources (48.6%) and that a mammogram can be painful (49.3%). Nevertheless, most of them (80.7%) still agreed that they would perform mammogram based on doctor’s advice. Additionally, a majority of the participants (67.4%) believed that visiting a doctor for breast clinical examination may lead to unnecessary fear and anxiety, a woman cannot detect breast cancer by herself (67%), a breast self-exam is painful and unnecessary (61.7%) and that a breast self-exam can lead to necessary fear and anxiety among women (68.3%). Participants’ responses (%) to breast and cervical cancer attitude statements (N = 300).
With regards to cervical cancer, the majority believed that screening and early detection for cervical cancer can save lives (80.6%) and that they will perform a Pap smear if the doctor advises (71.3%). Slightly more than half believed that women and girls should receive HPVV (54%) and that they will give their daughter the HPVV if the doctor advises (58%). However, many (42.3%) agreed that HPVV can cause unnecessary side effects. The majority, nevertheless, agreed with negative statements such as a Pap smear can be painful (59%), a Pap smear is a waste of resources (53%) and a Pap smear can cause unnecessary fear and panic among women (60.7%).
Practice
Proportion of Participants’ Responses to Questions on Practices Regarding Breast and Cervical Cancer Screening (N = 300).

Regarding cervical cancer screening-related practices, only a few of the participants responded in the affirmative that they ever had a Pap smear (31.3%), been advised by a health professional to have a smear test (30.7%), been advised by a health professional to receive HPVV (12%) and consented to give HPVV to own daughter (15.7%).
Sources of Information
A wide range of sources of information were reported by the participants (Figure 2). The highest reported sources were internet (44.7%), doctor (41%), social media (36.3%) and television (31%). While the least sources of information included sources such as books (9.7%) and posters (9.3%), among others. Proportion of participants by sources of information (N = 300).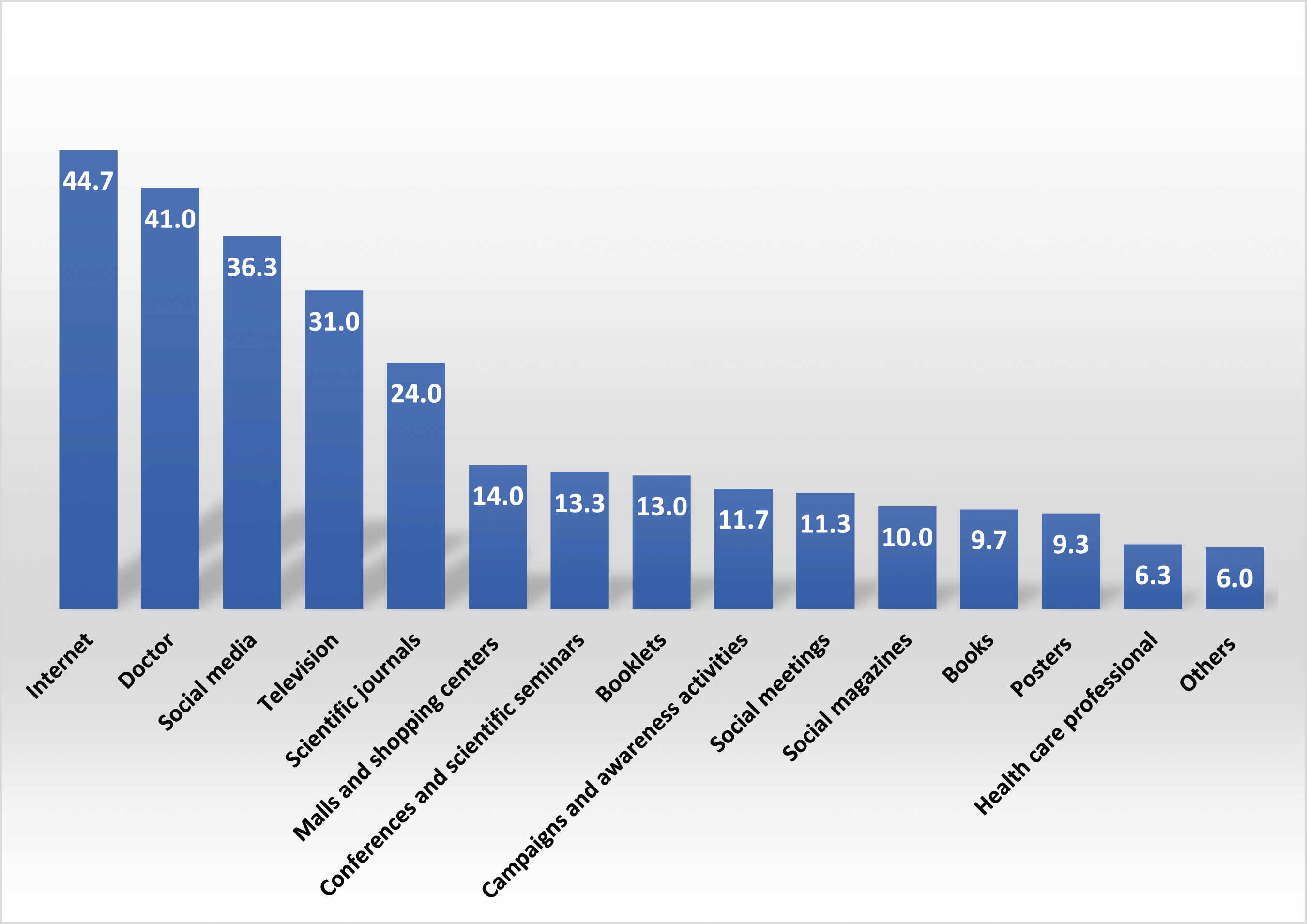
Discussion
This study aimed to understand the knowledge, attitudes and practices of women in the UAE regarding breast and cervical cancer prevention. It was found that the majority of women had low level of breast cancer prevention knowledge (63.3%) with lower uptake (36% for BSE, 30.6% for CBE and 23% for mammography). Same was the case for cervical cancer prevention with the majority having low knowledge (94.7%) and uptake (31.3%) of Pap test and not being recommended by HCP to get HPVV (12%). The attitudes exhibited by the participants were also less positive, perceiving screening as a waste of resources and source of fear. The study also reported internet, health care practitioners and social media to be the main sources of information.
Low levels of breast cancer prevention knowledge evident from our study are similar to findings from other studies conducted in the UAE and other GCC countries, indicating inadequate information of women specifically on mammography.10,12,13 Our results indicating low levels of cervical prevention information also affirm to the findings obtained from two other studies conducted in the UAE, suggesting detailed knowledge levels to be low, despite high awareness of Pap smear.15-17 Similarly, a previous study carried out to assess information on HPVV in 2013 in the UAE indicated it to be 22%, nearly similar to as reported in our study (19%). 18 A systematic review summarizing the knowledge and acceptability of HPVV in countries of MENA region highlighted lack of awareness on the topic. 24 Persistent low levels of knowledge among UAE women population regarding breast and cervical cancer prevention indicate requirement of effective measures to disseminate proper information to reach the targeted groups. Numerous interventions utilising knowledge provision have been successful in enhancing screening uptake for breast and cervical cancers.25,26 The significant association of certain sociodemographic factors with breast cancer knowledge as indicated in our study implies that older, unmarried women and those not accessing the health care regularly need to be focused for education delivery.
This study also reports lower participation of women in BSE and CBE which is lower than what was found in another study in the UAE in 2014 14 but higher than an earlier study conducted in 2001. 27 However, the lower uptake for mammography is found to be similar as in other studies. 14 Research has indicated that women tend to report at advanced stages of breast cancer, thus avoiding screening, possibly due to influence of cultural and behavioural factors. 28 Another possible reason could be lack of awareness of the breast cancer risk factors among women, as revealed in a recent study. 29 The Pap smear uptake was also found to be lower to what other studies had reported within the UAE and other GCC countries.12,15,16 The reasons behind lower cervical screening warrant need of further exploration, as evidence indicates the effect of sociocultural barriers on uptake. 30 The lower uptake of HPVV as evident in our study, demonstrated through low recommendation rates by HCPs and consent provision levels of mothers, is concerning. Literature suggests that HPVV acceptability within the region, governed by diverse social, religious, cultural and financial domains, can be enhanced by providing more information to HCPs and general public on the role of vaccination in cervical cancer prevention.24,31 Another noteworthy aspect is that recent studies have indicated a decrease in the cancer screening rates during COVID-19 pandemic in various regions of the world.32-34 Thus, it would be of value to investigate breast and cervical cancer screening uptake during and post-COVID period within the MENA region that has not been conducted till now.
Another interesting result from the study regarding attitudes towards cancer prevention was that women perceived the role of screening, especially Pap smear and mammography, as unnecessary and means of causing unnecessary worry and anxiety. Similarly, the majority had the perception that these screening tests can be painful. Such attitudes can be a possible reason to deter women from screening uptake as shown in previous studies. 35 Behavioural counselling by health care practitioners and use of role modelling by women who had already taken the test can possibly encourage women and lead to mindset change. 30 However, it is encouraging that the majority of the women were of the view to take the screening tests if recommended by their doctors, although less towards HPVV.
Among the information resources, the majority of participants informed that they had received information from the internet, followed by the doctor and social media. A recent qualitative study also reported the role played by internet and social media in breast cancer and its prevention awareness in the UAE. 36 Thus, targeted digital media campaigns can effectively enhance screening, but it should also be noted that misleading information presented on the internet can be harmful. Similarly, it can also be inferred from the results that the health care practitioner has a crucial part in persuading and encouraging women for screening. Although a majority of the women reported that they had not been recommended to take the tests or get HPVV by the doctors. Active participation of doctors could be beneficial towards improving cancer screening practices among women.37,38
A limitation of the study can be lack of generalization of results for overall UAE population, due to convenience sampling method. Additionally, the questionnaire employed was not validated, emphasizing the requirement for development of a validated breast and cervical screening questionnaire in the Arabic language. Further investigation for reasons of low proportion of women with good knowledge and practice levels is also warranted through future in-depth qualitative exploration.
Conclusion
In conclusion, this study adds to the existing literature on breast and cervical cancer prevention by encompassing a wide range of topics including assessment of women’s knowledge, behaviours and attitudes. It may provide important findings that may be used to design tailored health promotion strategies focussing on the knowledge gaps and misconceptions prevalent in the women. Future research to explore the barriers in detail is warranted, as is the practical intervention implementation to enhance the uptake by involvement of social media and health care practitioners.
Supplemental Material
Supplemental Material - Knowledge, Attitudes and Practices of Women in the UAE Towards Breast and Cervical Cancer Prevention: A Cross-Sectional Study
Supplemental Material for Knowledge, Attitudes and Practices of Women in the UAE Towards Breast and Cervical Cancer Prevention: A Cross-Sectional Study by Iffat Elbarazi, Zufishan Alam, Aminu S. Abdullahi, Shamma Al Alawi, Manal Al Khanbashi, Asma Rabaa, Aysha Al Aryani, Luai Ahmed and Fatma Al-Maskari in Cancer Control.
Footnotes
Acknowledgements
We would like to acknowledge all the participants of the study for their contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by SUREPLUS grant, provided by United Arab Emirates University.
Ethical Statement
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article and the consent forms were confidentially stored.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Abu Dhabi Health Services Company (SEHA)-Ambulatory Health Services (AHS) Ethics Committee (APPROVAL NUMBER: N/A)-approved protocols.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.