
Abstract
Background
Southeast Asian immigrant women in the U.S. have high rates of breast and cervical cancer, yet they are the least likely of all racial/ethnic groups to get screened. To address this disparity, we adapted the evidence-based Tailored Intervention Messaging System© (TIMS©), which uses tailored messages and navigation by culturally and linguistically matched community health advisors to overcome barriers to cancer screening.
Objectives
This study describes the cultural and linguistic adaptation of TIMS© to improve breast and cervical cancer screening among Southeast Asian immigrant women in the U.S.
Methods
Guided by Stirman et al.’s adaptation framework, we conducted focus groups and in-depth interviews to identify key constructs related to cancer screening (knowledge, perceived barriers, perceived risk, benefits, self-efficacy). Using the TIMS© and the thematic content from qualitative data, we modified messages for content and context. Messages were divided into three categories: 1) existing messages identified in thematic analyses, 2) existing messages not identified in thematic analyses, and 3) new messages that emerged from thematic analyses.
Results
Contextual and content modifications were made to the TIMS© message library. Messages were translated into Lao, Khmer, and Vietnamese. Through an iterative process, the investigator, community health advisors, and cultural community advisory board members reviewed and revised the messages for translation accuracy, relevance, and clarity.
Conclusion
Using relatable language and context is critical to engaging women from Southeast Asian communities in improving breast and cervical cancer screening uptake. This adaptation approach can be applied to tailor interventions for other languages, cultures, and underrepresented groups.
Plain Language Summary
Southeast Asian women in the United States face a critical health challenge. Despite having high rates of breast and cervical cancer, they are the least likely of all groups to get screened for these cancers. To address this problem, we adapted an evidence-based program called TIMS© that uses personalized messages and community health workers to help women get cancer screenings. To make TIMS© more effective for Southeast Asian women, we needed to ensure it was culturally appropriate and available in their languages. We conducted group discussions and one-on-one interviews to understand what women knew about cancer screening, what barriers they faced, and their views on risks and benefits. Using what we learned, we reviewed the program's messages. Some original messages matched well with the women's experiences, while others did not fit their cultural context. We also created new messages based on what we learned from the community. All messages were then translated into Lao, Khmer, and Vietnamese languages. Working with community health advisors and a cultural community advisory board, we carefully reviewed each message to ensure they were accurately translated, clear, and meaningful to Southeast Asian women. This collaborative process helped us create messages that truly resonated with the community. To encourage people to get screened for cancer, programs must speak their language. This approach to adapting health programs could serve as a model for improving healthcare access for other communities as well.
Keywords
Introduction
Screening recommendations have led to early detection and reduced mortality from breast and cervical cancer in the United States (U.S.). 1 However, Asian American women have low cancer screening rates and are at significant risk for both cancers.2,3 They are less likely to adhere to screening recommendations compared to other groups.4,5 Breast cancer ranks first for cancer incidence and second in cancer mortality in Asian American women.6,7 They also have significantly lower Pap test rates (70%) compared to that of Non-Hispanic White women (81%), 8 and screening trends are decreasing. 5
Of all Asian Americans, Southeast Asian women, including Cambodians, Lao, and Vietnamese, have the highest cancer mortality rates and the lowest screening rates. 9 Barriers to screening include limited access to healthcare services, lack of health insurance, language barriers, cultural beliefs and misconceptions about cancer, fear of the screening process, and competing priorities such as family responsibilities and financial constraints.4,10-12
While interventions promoting breast and cervical cancer screening have been tested, a recent systematic review found that none of the interventions employed novel strategies targeting this population. 13 Patient-centered communication strategies can mitigate concerns, fears, and beliefs about cancer screening, 14 but questions remain about existing programs’ cost-effectiveness and long-term sustainability.
Tailored messaging systems allow healthcare providers to assess individual health beliefs and deliver patient-centered health messages that enhance motivation and support positive health behaviors. These systems have successfully changed health behaviors 14 and improved cancer screening rates in primary care settings, 15 but their effectiveness in addressing the unique barriers faced by Southeast Asian women remains untested. Menon et al. 16 demonstrated that combining tailored messages with patient navigators improved appointment scheduling and a four-fold increase in colorectal cancer screening in a multicultural sample.
We adapted the evidence-based Tailored Intervention Messaging System© (TIMS©), which incorporates a combination of tailored messages delivered by community health advisors (CHAs) to overcome cancer screening barriers. CHAs, also known as community health workers, promotoras, or lay health workers, are members of the communities they serve. They provide health promotion and education and link communities to services.17,18 Bilingual CHAs from the Southeast Asian community, specifically Cambodian, Lao, and Vietnamese, delivered the tailored navigation intervention. Navigation activities included scheduling clinic appointments, appling for insurance, and arranging transportation to clinic appointments. Given the low screening adherence among Southeast Asian immigrant women and the success of adapted versions of the TIMS©, we believed a similar program could address cultural and language barriers and improve cancer screening rates.
This paper describes the cultural and linguistic adaptation of a tailored navigation intervention to improve breast and cervical cancer screening uptake among Southeast Asian women in the Midwest. We describe our process and recommendations for future studies. This study was approved by the Institutional Review Board at the Ohio State University (IRB protocol number: 2018B0521).
Methods
TIMS©
The TIMS© is an educational program based on the Health Belief Model, delivered by phone, in-person, or computer15,19 The TIMS© was initially designed to increase colorectal cancer screening among African American and non-Hispanic White adults.15,19 The TIMS© uses a library of messages tailored to constructs of knowledge, perceived risks, barriers, benefits, and self-efficacy to change health behavior, specifically cancer screening. The tailored message library is contained within the evidence-based TIMS© program and incorporates a combination of tailored messages delivered either online or in person and navigation by a community health advisor to overcome barriers to complete cancer screenings. The intervention has been subsequently adapted, translated, and tested in trials with diverse populations, including Hispanic/Latino (colorectal screening), 16 Chinese American (breast cancer screening),20,21 and Korean American (breast and colorectal screenings) populations, 22 and American Indian. 23
Areas of Adaptation Using the FRAME. 26

Adaptation of TIMS© for the Southeast Asian Population
Adapting the tailored navigation intervention, TIMS©, for Southeast Asian women involved two distinct studies. In our first study, our exploratory study, we conducted focus groups and in-depth interviews with Khmer and Lao women. Qualitative methods and results have been previously published.24,25 In brief, we first conducted focus groups with women from two Southeast Asian communities about their barriers and facilitators in getting Pap testing.
25
Dyadic interviews were then conducted with mothers and daughters to understand how these women converse about women’s health issues, specifically cancer and getting screened.
24
We selected constructs for tailoring based on data from the focus groups and interviews (details are described below). The current study encompassed adapting the tailored messages and working with the study’s CCAB and CHAs to check for relevance, accuracy, and clarity.
28
Figure 1 illustrates our intervention adaptation process. TIMS© Adaptation Process for Southeast Asian Women.
Cultural Community Advisory Board (CCAB)
We drew on the strength of our previous work with the Southeast Asian community and garnered assistance from our established CCAB to guide our research design and procedures. 29 The CCAB represents key leaders, healthcare professionals, and advocates from the local Lao, Khmer, and Vietnamese communities. The study investigators worked closely with the six-member CCAB from study conception to dissemination to ensure that the study was culturally responsive to the Southeast Asian community. Longstanding engagement with our CCAB members has been described elsewhere.29,30 The CCAB’s role in this study was to identify community assets to support the study, serve as a liaison between the research team and community members, provide guidance on culturally appropriate and relevant measures and data collection procedures, verify the accuracy of professionally translated materials, engage in problem-solving with the research team, and participate in the dissemination of findings.
Development of TIMS© Message Library
We developed themes based on focus groups and in-depth interviews with Southeast Asian women participants.21,22 Guided by Menon et al.’s process for adaptation of the TIMS© message library, 23 we divided the messages into three categories: (1) Messages in the existing library also identified in the current thematic analysis; (2) Messages in the existing library that were not identified in the current thematic analysis; and (3) Messages not in the existing library that emerged in the current thematic analysis.
The messages are as follows: Category (1) Messages in the existing library also identified in the current thematic analyses. For this category, we reviewed the messages with the study team (investigators and CHAs) and CCAB and made suggested revisions to phrasing and vernacular specific to Lao, Khmer, and Vietnamese to be included in the final message library. Common constructs that existed in both libraries included: knowledge, barriers, benefits, perceived risks, self-efficacy, and high-risk status. Example of message: Perceived Risk: Does not have relative with breast cancer Message: Being a woman and growing older puts you at risk for getting breast cancer. Many women who get breast cancer are like you – they don’t have a history of it in their family. In fact, 3 out of 4 women who get breast cancer don’t have a family history. Category (2) Messages in the existing library that were not identified in the current thematic analyses Example of message: Benefits: Check symptoms (get screened to check symptoms) Message: Symptoms should always be checked by a healthcare provider. By checking symptoms, you can find out what maybe wrong and what you need to do. Most conditions, if caught early can be handled more easily. Not all symptoms are cancer either, so you may find out you don’t have cancer which can give you peace of mind. Category (3) Messages not in the existing library that emerged in the current thematic analyses. This category includes issues that are unique to Southeast Asian women that were identified from the qualitative study. New themes included refugee experience, post-resettlement experience, relationship dynamics, and social networks. We developed new messages, which were then reviewed and modified by CHAs and CCAB members. Example of message related to Refugee Experience: Mistrust of Medical System: Mistrust of medical provider Message: It can be scary to go to the doctor if you’ve had bad experiences in the past. If it makes you feel more comfortable, you can take a family member or friend with you to your appointment. I can also help you find a healthcare provider or clinic that you’ll be comfortable going to. Example of message related to Post-resettlement Experience: Communication: Language as a barrier Message: When healthcare providers don’t speak your language, it can be really frustrating. Sometimes, even if they are talking in English, it can be hard to understand all the medical language. You have a right to an interpreter when you go see a doctor. You can always ask to have a female interpreter during your Pap test appointment.
Results
Type of Modifications
Stirman et al.26,27 outline the types of content modification, which are changes made to the intervention procedures, materials, or delivery. We adapted the intervention originally designed for African American men to improve colorectal cancer screening to specifically address the beliefs and barriers faced by Southeast Asian women in obtaining breast and cervical cancer screening. See Table 1. These modifications were made at the population level, targeting a particular cultural, ethnic, clinical, or social group (contextual modifications). 26 In addition, we created culturally relevant participant profiles, including eligibility information, screening status, knowledge about cancer and screening, beliefs, and barriers, which we used during recruitment role-play training with CHAs.
The content modifications encompassed both cultural and linguistic tailoring of the messages. For example, we included the construct of the unique experiences of refugees and addressed issues related to mistrust of healthcare providers. To encourage mother and daughter dyad communication with each other, we incorporated personal reminder notecards in which a dyad partner would handwrite a personal message of reminder to get a mammogram or Pap test. Additionally, we lengthened the time CHAs would contact participants from the TIMS© of only one touch point to 10 weeks. We understood from our prior research the potential need to extend the amount of time to navigate women to screening in these communities.31,32
Message Translation
Tailored Message Development Process – Vietnamese Language Example.
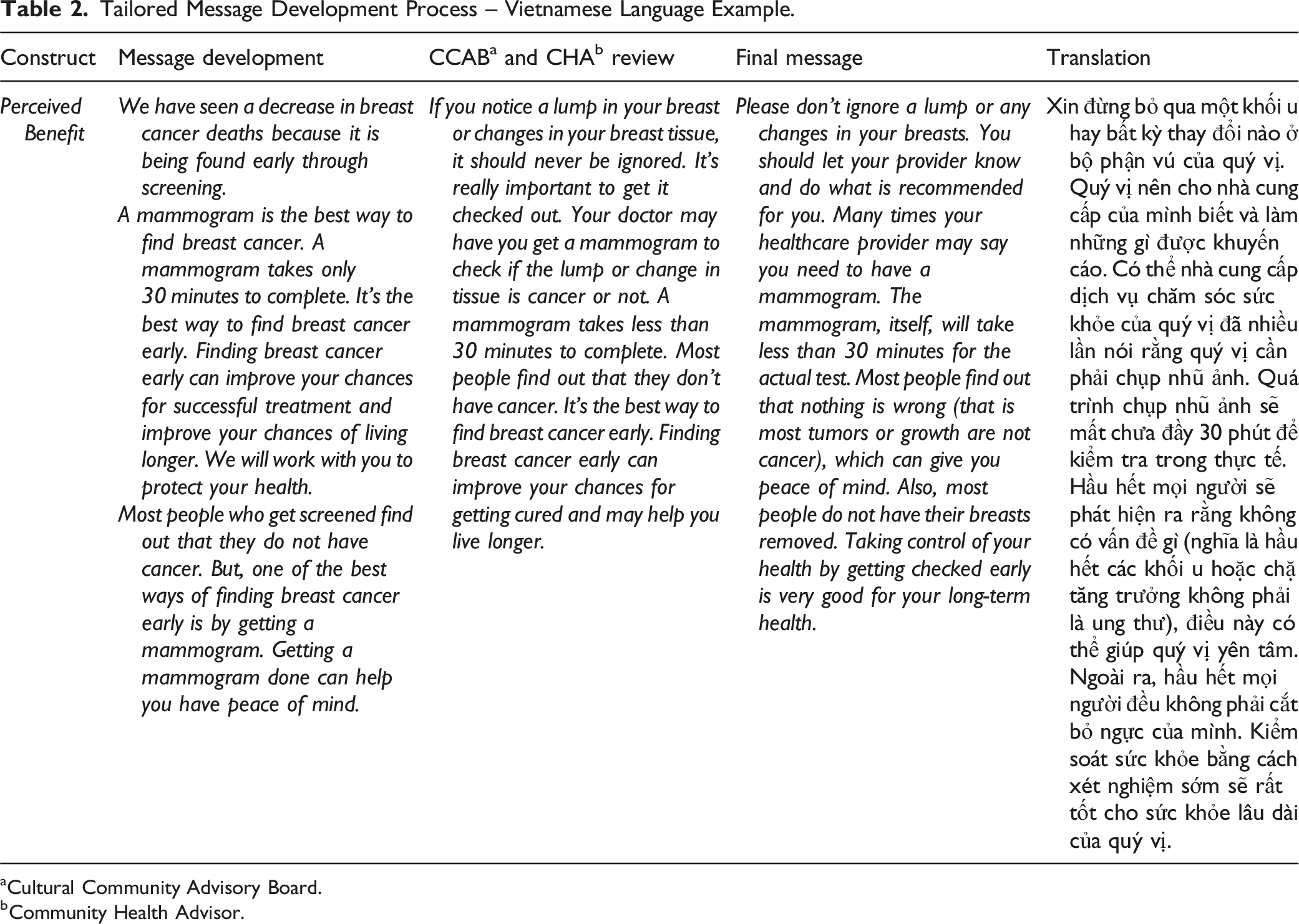
aCultural Community Advisory Board.
bCommunity Health Advisor.
Based on the success of our previous work, we took a consensus approach to translating materials. 33 It was essential for us to include CHAs and CCAB members to assist in this process rather than relying on back translation. By including native language speakers, we captured the nuances of not only the language and culture but also the intended approaches and meaning of messages. This insider knowledge from multiple individuals enabled us to be culturally mindful and inclusive of differing perspectives and language variations.
Navigation Training Using Adapted Tailored Message Library
The CHAs practiced extensively using the tailored message library with one another and other volunteers, both in English and their native language. We utilized mock participant profiles for role-play exercises. Each of these profiles contained potential scenarios CHAs could encounter in their respective communities. Using the tailored messages with a role-play volunteer, the CHAs addressed the barriers highlighted in the mock participant profiles. CHAs were evaluated on their performance using a standardized process evaluation form developed and implemented by the study team in prior studies. 15 Each CHA role-play was video recorded on Zoom and used for training. The investigators used the standardized rubric to evaluate the CHA’s ability to properly identify barriers, respond to barriers and beliefs, and maintain overall conversation flow and professionalism. 15 A score above 90% indicated that the CHA was ready to begin recruitment and data collection. A score below 90% indicated that the CHA needed additional training or practice. After a week of review and practice the CHA could then be re-evaluated using the same process. The evaluation process was a critical part of our standardized intervention delivery and fidelity monitoring procedures. We incorporated refresher trainings for CHAs as needed.
The results of the clinical trial will be reported in a forthcoming publication. The efficacy of the tailored navigation will be evaluated through completion rates of Pap tests and/or mammograms. This outcome will be assessed through both self-reports by participants and verification of medical record checks. These results will provide critical evidence regarding the intervention’s efficacy in improving cancer screening rates among this population.
Discussion
The purpose of this paper was to describe the cultural and linguistic adaptation of a tailored navigation intervention to improve breast and cervical cancer screening uptake among women from three Southeast Asian communities in the Midwest. Southeast Asians are a heterogeneous population that makes up 14% of U.S. Asian American population and is one of the fastest-growing populations in the U.S. 34 Still, they may be overlooked when examining overall cancer morbidity and mortality and engagement in cancer screening intervention research. There is also a tendency to group all Asian immigrants under a ubiquitous rubric of Asian Americans discounting the differences between the many countries that comprise South and Southeast Asia.
From 1988-2013, breast cancer incidence rates among Asian Americans steadily increased at 1.5% annually with Southeast Asian women experiencing the sharpest increase in breast cancer incidence among all Asian American groups. 35 As rates of breast and cervical cancer continue to rise substantially in Southeast Asian Americans,9,35 early detection and preventive screenings are more important than ever to reduce cancer deaths. Evidence points to the efficacy of culturally tailored navigation interventions to improve cancer screening and early detection among individuals who face obstacles in accessing preventive care.14,36,37 The benefits of tailored navigation interventions are well documented, offering enhanced personalized strategies to address the unique challenges individuals face in accessing cancer screening. 38 However, implementation of tailored navigation interventions in Southeast Asian communities, specifically Lao and Khmer is still lacking.
Our study’s success was largely due to our bilingual and bicultural CHAs who were integral in the adaptation process and later in the study implementation. Our CHAs were fluent in their native language, and all but one of them was a lifelong member of the local communities. The CHAs had little to no research experience; thus, exposure to community-engaged research provided opportunities for them to expand their knowledge and skills and be involved in research in the future. By engaging CHAs to intervene at the individual level, we expected to set a course to make behavior change happen. CHAs who share the same language and cultural background as the priority population can help overcome language barriers and cultural differences, facilitating community engagement in research.16,29 Participants from communities that do not normally engage in research may feel more comfortable and trusting when interacting with CHAs who understand their cultural norms, beliefs, and health practices. This rapport can foster community collaboration and buy-in from the target population, leading to greater participation in research and impactful research outcomes. CHAs can also provide valuable insights into culturally appropriate research methods, helping researchers to design studies that are respectful and relevant to the population’s cultural context. Importantly, involving CHAs can build research capacity within the community by providing training and skill development opportunities for its members. 33 Research capacity building further fosters the sustainability of community-academic partnerships and future research collaborations.
Together with our CCAB, with whom we have had a long-standing relationship, CHAs and investigators created a culturally and linguistically relevant and acceptable library of tailored messages in three different Southeast Asian languages. The translation, interpretation, and message development process demanded careful attention and dedication, which took some time to complete thoroughly, as evidenced by an iterative process between investigators, research staff, CCAB, and professional translators. We approached translation through a consensus process between all stakeholders to develop the most relevant and impactful tailored messages. In our prior studies, we found this to be an effective and more inclusive method33,39 and an adaptable approach for other languages.
Implications for Future Interventions and Research
The potential to adapt this approach to other underserved populations facing significant challenges in obtaining cancer screening is substantial. Expanding its application across different cancers and health areas could further enhance its impact. The process used in adapting and implementing the TIMS© should serve as a model for other investigators working with diverse populations. Future research should focus on long-term follow-up studies with the women who participated in the tailored navigation using TIMS© to assess its sustained impact. This will provide valuable insights into the long-term efficacy for broader application of the intervention.
Strengths and Limitations
There are notable strengths worth mentioning. We worked alongside medically underserved communities that have been largely left out of cancer screening engagement and research, particularly Lao and Cambodian populations, in this community-engaged study, first through the exploratory phase and then on adapting this tailored navigation intervention. The collaboration has spanned more than a decade. This is a testament to the commitment of the study team to engage community stakeholders in research and build capacity in these communities. By taking a community-engaged approach to the adapted TIMS©, we enhanced our research efforts’ cultural relevance and acceptability.
This study is not without limitations. Our study population was based in Ohio; thus, some messages may not be relevant to Southeast Asian women outside of this geographic location. The population in Ohio may have differing perspectives and experiences related to mammography and Pap testing than other areas where Southeast Asian populations are more extensive and more diverse.
Conclusion
Overall, increasing cancer screening for underserved populations is essential for achieving health equity, improving health outcomes, and ensuring that all individuals can benefit from early cancer detection and treatment. Testing culturally tailored approaches to cancer screening involves critical areas to improve the accessibility, acceptability, efficacy, and effectiveness of these interventions for diverse populations. Several promising directions for this work include enhanced community engagement and collaboration, integration of technology, development of culturally tailored risk assessment tools, adaptive trial designs, training and capacity building, and focus on high-risk populations.
Supplemental Material
Supplemental Material - Cultural and Linguistic Adaptation of an Evidence-Based Tailored Navigation Intervention to Increase Cancer Screening Uptake Among Southeast Asian Women
Supplemental Material for Cultural and Linguistic Adaptation of an Evidence-Based Tailored Navigation Intervention to Increase Cancer Screening Uptake Among Southeast Asian Women by Jennifer Kue, Judith A. Tate, Bárbara Piñeiro, Laura A. Szalacha, Bounthanh Phommasathit, Somany Pich, and Usha Menon in Cancer Control
Footnotes
Acknowledgments
We thank the Southeast Asian Women’s Health Project Community Health Advisors, Paula Chanhmany, Anh Thu Thai, Chantra Phom, and Patch Wetzel, and Cultural Community Advisory Board members, Vanh Sivixay, Bounthanh Phommasathit, Yan Ke, and Somany Pich, for their invaluable contributions to this study. We are also grateful to the Khmer, Lao, and Vietnamese communities in Central Ohio for their support and participation.
Statements and declarations
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the American Cancer Society Research Scholar Grant [RSG-CPHPS 131811, PI: Kue].
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Jennifer Kue, upon reasonable request. However, due to ethical considerations and participant confidentiality, access to data is limited to ensure the privacy of participants involved in the research. Aggregated and anonymized data may be provided upon request for research purposes.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.