
Abstract
Purpose
The purpose of this study was to investigate the effect of laparoscopic left colectomy (LLC) and laparoscopic sigmoidectomy (LSD) on short-term outcomes and prognosis of sigmoid colon cancer (SCC) patients using propensity score matching (PSM).
Methods
In this retrospective study, the SCC patients who underwent LLC or LSD surgery were collected from a single clinical center from Jan 2011 to Dec 2019. Short-term outcomes and prognosis were compared between patients who received LSD surgery and LLC surgery.
Results
A total of 356 patients were included in this study. After 1:1 PSM analysis, there were 50 patients who underwent LLC surgery and 50 patients who underwent LSD surgery left in this study. No significant difference was found in baseline characteristics after PSM (P > .05). In comparison with the LLC surgery group, the LSD surgery group had shorter operation time (P = .003) after PSM. Moreover, the surgical procedure was not an independent predictor for overall survival (OS) (P = .918, 95% CI = .333–2.688) and disease-free survival DFS (P = .730, 95% CI = .335–2.150), but age (OS: P = .009, 95% CI = 1.010–1.075; DFS: P = .014, 95% CI = 1.007–1.061) and tumor stage (OS: P = .004, 95% CI = 1.302–3.844; DFS: P < .01, 95% CI = 1.572–4.171) were the independent risk factors for OS and DFS in SCC patients.
Conclusion
There was no significant difference between the two surgical procedures for prognosis of SCC patients. However, the possible reasons for changing the surgical procedures should be cautious by surgeons.
Introduction
Colorectal cancer (CRC) has the third most incidence rate in the world and is one of the common leading causes of mortality. Moreover, the mortality and morbidity of CRC are increasing in the world. 1 Sigmoid colon cancer (SCC) is one type of CRC, which is located between the descending colon and rectum. 2 SCC is not easy to detect timely because of the mild symptoms in the early stage. However, the advanced SCC can result in persistent abdominal discomfort, pain, and even intestinal obstruction. 3 The sigmoid was the most common site of CRC and had a higher risk of CRC than other sites. 4
Since laparoscopic colectomy was first used to treat CRC patients in 1991, 5 increased studies demonstrated that the efficacy of laparoscopic surgery had more advantages to get a better prognosis for CRC.6,7 Although the 5-year survival rate of SCC-received laparoscopic surgery was only about 60%, laparoscopic surgery was still the most common treatment by surgeons currently. 8 The main laparoscopic surgical technique to treat SCC included the laparoscopic left colectomy (LLC) and laparoscopic sigmoidectomy (LSD). 9
Although laparoscopic operation is a mature technique, lack of experience in laparoscopic CRC surgery may still increase operative risk. 10 The LSD is the most common operation for resecting SCC. However, surgeons would have to extend the range of surgical resection because of intestinal pathological damage in adjacent tissue, 11 intestinal ischemia caused by ligation of an anatomic variant branch of a vascular, 12 or serious diverticular disease encountered during the operation. 13 Therefore, lack of laparoscopic operation experience and extensive surgical excision were associated with surgical changes.14-18 In consideration of these influence factors, some SCC patients would have to receive LLC surgery ultimately.
However, there were no related studies comparing the two surgical procedures to identify the difference in prognosis and analyze the possible causes of changing LSD to LLC. Therefore, the purpose of this study was to analyze the effect of two operations on short outcomes and prognosis of SCC patients using PSM analysis and to analyze why surgeons perform LLC but not LSD for SCC.
Methods
Research Design and Patients
The study was retrospective-designed research and confirmed to STROBE guidelines. 19 All 356 adult SCC patients who underwent LLC or LSD surgery in a single clinical center from Jan 2012 to Dec 2019 were retrospectively included. All patients’ details were de-identified in this study. And the medical records were collected as well. This study was approved by the Ethics Committee of The First Affiliated Hospital of Chongqing Medical University (K2023-308).
Inclusion and Exclusion Criteria
Patients who underwent elective LLC or LSD surgery and were pathologically diagnosed with SCC after surgery were included in this study (n = 532). Patients were excluded according to the following exclusion criteria: (1) stage IV SCC (n = 53); (2) incomplete medical records (n = 117); (3) non-R0 resection (n = 6). Finally, all 356 patients were included.
Surgery Management and Follow-Ups
All SCC patients underwent elective radical LLC or LSD surgery according to the AJCC 8th Edition. 20 And these patients were followed up with regular blood and imaging tests every three months for the first three years after surgery and every six months for the next two years. The median follow-up time was 28 (3–101) months.
Definitions
Patients were divided into the LLC and LSD groups, depending on the surgical procedure. All operations were performed by CRC surgery specialist group in our hospital, and all surgeons in this group had more than 10 years of surgical experience. And the tumor node metastasis (TNM) stage was diagnosed in accordance with the AJCC 8th edition as well. Clavien-Dindo classification was used to grade the postoperative complications. 21 And major complication was defined as ≥ grade III. Overall survival (OS) was defined as the time from surgery to death or last follow-up. Disease-free survival (DFS) was defined as the time from surgery to tumor recurrence, metastasis, death, or last follow-up.
LLC Surgery
During the surgery, an ultrasonic scalpel was used to cut along the descending colon groove to open the sigmoid mesentery. The descending colon was separated from the outside along a loose, avascular space to the splenic flexure of the colon, and the splenic colonic ligament was cut. And the root of left colonic vessels (including arteries and veins) and the first branch of sigmoid vessels were clamped and severed. The sigmoid colon was then separated until 5 cm above the sigmoid-rectal junction. The transverse mesocolon and gastrocolic ligament were identified, and the ultrasonic scalpel was used to cut the gastrocolic ligament in the avascular zone at the middle part, removing the gastrocolic ligament leftward until the splenic flexure, freeing the entire splenic flexure. Then, the transverse mesocolon was exposed and separated. The middle colonic vessel was identified, and then the left branch of the middle colonic vessel was clamped and cut. The transverse mesocolon was separated to completely free the left half of the transverse colon. The left half of colon was cut about 10 cm away from the tumor at both ends. The remaining transverse colon was then anastomosed with the sigmoid colon. The main part of the surgery was completed.
LSD Surgery
During the surgery, an ultrasonic scalpel was used to cut along the right side of the sigmoid mesentery at the junction of the rectum and sigmoid colon. The mesentery was separated along a loose, avascular space down to the root of the inferior mesenteric artery (IMA). Then cleaning adjacent lymphatic fatty tissues, the IMA and left colonic artery (LCA) were exposed. The IMA away from LCA was clipped and severed and the LCA was preserved. The inferior mesenteric vein (IMV) was exposed and severed in the left of IMA. And the mesentery of the sigmoid colon and mesorectum were exposed and isolated, and the sigmoid colon was laterally dissociated. The sigmoid colon was then separated along the posterior side of the tumor until 10 cm away from the distal end of the tumor, and the colon was cut at this point. The proximal end of the sigmoid colon was cut at a point 10 cm away from the tumor. The remaining bowel segments were anastomosed. The main part of the surgery was completed.
Data Collection
The medical records were retrospectively collected from electronic medical system, and the follow-up records were collected via telephone interviews. The baseline information included age, sex, body mass index (BMI), smoking, drinking, hypertension, type 2 diabetes mellitus (T2DM), surgical history, hemoglobin, albumin, tumor size, and tumor stage. The short-term postoperative outcomes included operation time, blood loss, hospital stay, overall complications, and major complications. OS and DFS were included in the prognosis information.
Propensity Score Matching
To minimize the selection bias between the two groups, PSM was performed to match the LSD group patients to the LLC group patients in this study. Nearest neighbor matching was performed without replacement at a 1:1 ratio, and a caliper width with a .1 standard deviation (SD) was specified. The baseline information and surgical outcome information were matched including age, sex, BMI, smoking, drinking, hypertension, T2DM, surgical history, hemoglobin, albumin, tumor size, tumor stage, operation time, blood loss, hospital stay, major complications, and overall complications.
Statistical Analysis
Continuous variables, including age, BMI, operation time, blood loss, and hospital stay, were calculated by the mean and standard deviation (SD). Independent-sample t-tests were used to compare continuous variables between the LLC group and the LSD group, and Chi-square test or Fisher’s exact test was used to compare the other parameters between the two groups. The Kaplan–Meier curve was performed to compare OS and DFS between the LSD group and the LLC group. The Cox regression analyses were conducted to identify independent risk factors for OS and DFS. The SPSS (version 22.0) statistical software was used to analyze these data. A bilateral P-value <.05 was considered statistically significant.
Results
Baseline Characteristics
Baseline Characteristics Before and After PSM.
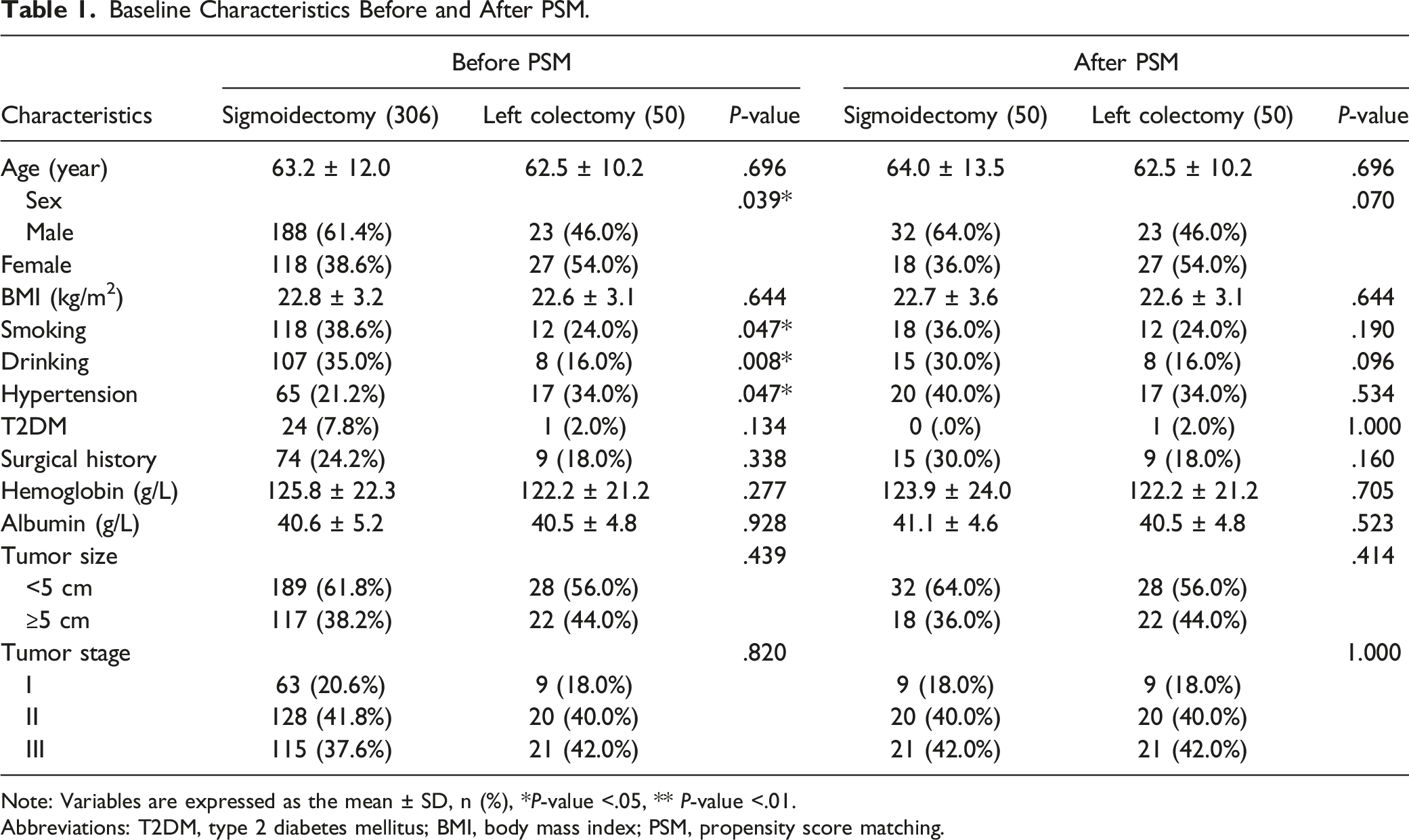
Note: Variables are expressed as the mean ± SD, n (%), *P-value <.05, ** P-value <.01.
Abbreviations: T2DM, type 2 diabetes mellitus; BMI, body mass index; PSM, propensity score matching.

Flow chart of patient’s selection.
Short-Term Outcomes
Short-Term Outcomes Before and After PSM.

Note: Variables are expressed as the mean ± SD, n (%), *P-value < .05.
Abbreviations: PSM, propensity score matching.
Long-Term Prognosis
In whole cohort, both the median survival time and the median follow-up time were 28 (3–101) months. The comparison of OS and DFS was performed between the LSD and LLC groups. And the results were demonstrated by the Kaplan–Meier survival curves (Figure 2). There were no significant differences between the two groups in OS (P = .917) and DFS after PSM (P = .729). OS and DFS after PSM. (a) The comparison of OS between the two groups. (b) The comparison of DFS between the two groups. Abbreviations: OS, overall survival; DFS, disease-free survival; PSM, propensity score matching.
Risk Factors for Prognosis
Univariate and Multivariate Analyses of Overall Survival of the Whole Cohort.

Note: *P-value < .05, ** P-value < .01.
Abbreviations: HR, hazard ratio; CI, confidence interval; BMI, body mass index; T2DM, type 2 diabetes mellitus.
Univariate and Multivariate Analyses of Disease-free Survival of the Whole Cohort.
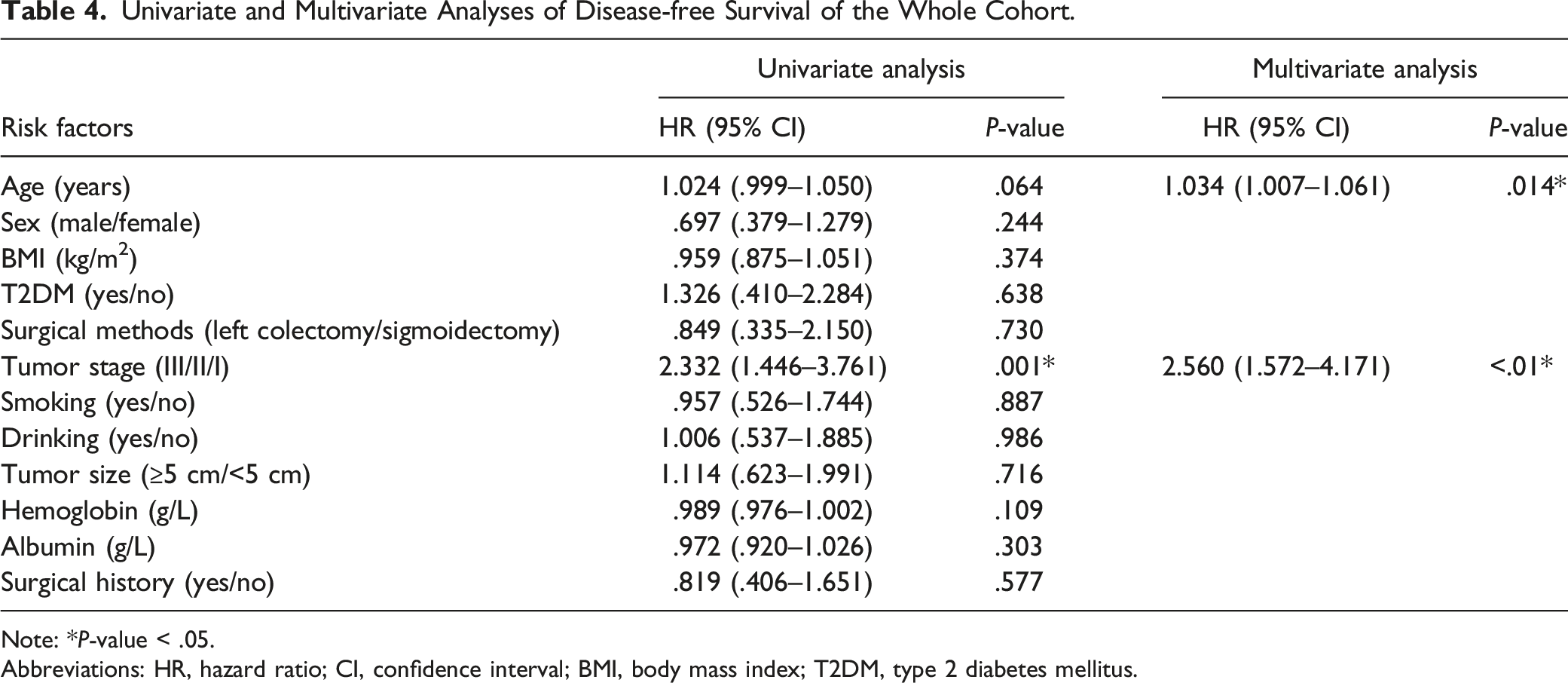
Note: *P-value < .05.
Abbreviations: HR, hazard ratio; CI, confidence interval; BMI, body mass index; T2DM, type 2 diabetes mellitus.
The Reasons to Convert Operative Method
Reasons to Convert Surgery Style.

Discussion
There were 306 patients who underwent LSD surgery compared with 50 patients who underwent LLC surgery in this study. After PSM, there were 50 patients in the two groups, respectively. In terms of short-term outcomes, only operation time had a significant difference between the two groups. Additionally, there was no significant difference between the two groups in baseline information and prognosis.
Laparoscopic surgery is the main treatment for SCC currently, and 9 then the efficacy of surgery correlates with patient’s prognosis. The different effects of laparoscopic surgery vs open surgery in CRC were explored, 22 and an association between CRC and specified surgery in terms of prognosis was found. 23 In a randomized-controlled trial comparing extended complete mesocolic excision (CME) vs standard CME in SCC, Planellas P et al 24 found the total number of lymph nodes, DFS, and OS had no significant difference in the comparison of the two surgical procedures. Our results were similar with their outcomes. However, they found more urinary and sexual dysfunction in men in the extended-CME group. Unlike in our study, although there was no significant difference in patients’ prognosis between the two groups, we analyzed the possible reason to convert surgical procedure. Despite the effect of different CMEs in SCC was explored, no study compared the effect of LLC vs LSD in SCC treatment and identified possible reasons to convert surgical procedures in SCC. Therefore, this is the first study to compare the curative effect of two surgical procedures in SCC and analyze the possible reasons to convert surgical procedure. And the PSM was conducted in this study to control the selection bias and improve the level of evidence. 25
The LSD group had shorter operation time and less intraoperative blood loss than the LLC group in this study. It was clear that LLC surgery had larger resected extent than LSD surgery. The operation time might be influenced by the difficulty of surgical procedure and the complexity of surgical resection extent. In terms of blood loss, Hartwig W et al suggested that the malignant disease might be an indication to predict a longer operative time and a higher blood loss. 26 And Katz et al. found that the extent of surgical procedure could also influence blood loss. 27 In addition, previous studies demonstrated that metabolic diseases could cause cardiovascular disease and visceral vascular disease;28-30 therefore, the SCC patients concurrent with metabolic diseases might increase difficulty of surgery and influence the surgical outcomes. As a common complication of gastrointestinal surgery, anastomotic leakage (AL) should be paid attention to in all surgery-related studies. Sciuto A et al reviewed that the colorectal leak rates ranged from 0 to 20%. 31 Before and after PSM, the prevalence of AL was 2.0% and .0% in the LSD group, respectively, in this study. Although there was no statistically significant difference in prevalence of AL between the LSD and LLC surgery groups, the relatively small number of patients in this study might have an impact on the results, potentially limiting and influencing the outcomes. Carannante F et al showed that stoma method was often performed to reduce the prevalence and severity of AL. 32 However, all patients received complete bowel preparation and elective surgery. Therefore, no stoma was performed in this study.
There was no significant difference in surgical procedure and other parameters between the two groups; however, age and tumor stage might have a predictive value for prognosis of SCC patients in this study. Older patients typically had more metabolic disease comorbidities, which had been shown to have a negative correlation with patient prognosis.14,33 Liu XY et al found that younger CRC patients undergoing primary surgery had a better prognosis than older CRC patients. 33 This outcome was similar with this study. In terms of tumor stage, higher tumor stages required more comprehensive treatments, including surgery, radiotherapy, and chemotherapy. Meanwhile, these treatments would affect the quality of life of patients, and tumor with higher stage or malignancy was less sensitive to chemotherapy or other treatments, leading to worse prognosis of patients.34,35
As for the possible causes to convert surgical procedure, although no significant difference in tumor size was found between the two groups before and after PSM in this study, larger tumor diameters were found to be the reason for switching to LLC surgery in 44% SCC patients. Cai S et al demonstrated that tumor size was usually used to be an indicator to predict the degree of the tumor malignancy. 36 Furthermore, tumor infiltration depth and width were part of the major concern in the preoperative diagnosis of SCC. 37 And the extensive tumor infiltration might reveal that there were more lymph node metastases and larger tumor size in the pathogenic site. However, preoperative examination could not reflect all aspects of SCC, and surgeons sometimes would change prearranged surgical procedure due to differences in tumor size and tumor malignancy in the internal abdominal conditions during the intraoperative time. And to ensure the radical resection of the malignant tumor, it was crucial to extend resection to reduce the risk of malignant metastasis. 38
Moreover, when larger tumor reached or located in the descending sigmoid junction, especially in stage II or higher stage SCC, the LLC surgery was often performed to ensure the sufficiency of radical resection. 39 In addition, Bertrand MM et al found that individuals had wide variations in the division branches of IMA, 40 becoming difficult for surgeon to reproduce standard surgical procedure. Therefore, it was difficult for surgeon to ensure the standard low ligation of IMA in LSD surgery for different SCC patients. And SCC patients with anatomical variation of division branches of IMA who underwent LSD surgery might be at a risk of unnecessary vessel injury, leading to poor intestinal motility and loss of function after intestinal reconstruction, and the deactivated bowel had to be extended resected to rejuvenate the reconstructed bowel and ensure bowel function.
Meanwhile, most SCC patients could not be easily diagnosed in early tumor stage. Due to the long-term tumor infiltration and malignant pathological changes in bowel tissues, the surrounding bowel wall of the tumor might suffer injury. The intestinal damage including intestinal edema, luminal distention, and ischemia was the common pathologic process. 41 Young J et al found that intestinal edema might delay intestinal transit, prolong patient’s recovery time, and even lead to death. 42 The intestinal edema might pose an obstacle to the functional recovery of the reconstructed bowel, thereby increasing the risk of anastomotic leakage formation after surgery. Therefore, to reduce and avoid the risk of anastomotic leakage or other severe complications, surgeons might convert LSD surgery to LLC surgery for resecting the intestinal edema. Furthermore, the anatomy of the sigmoid colon could vary among individuals. Surgical techniques would be changed when surgeons found that the sigmoid colon was too short 43 because prearranged surgery might lead to increased anastomotic tension in the reconstructed bowel, even anastomotic leakage or other complications. 44 Although there was no significant correlation between surgical procedure and prognosis of SCC patients, it is important to note that changes in the surgical approach may still pose potential surgical risks for patients. Therefore, further studies are still needed to explore and reduce the potential risk of surgery.
There were several limitations in this study. First, this was a retrospective study with 356 patients collected from a single medical center, which is a relatively small data. Therefore, the prevalence of AL, stoma, and stoma complications in SCC patients were relatively small as well, potentially limiting and influencing the outcomes. Second, there was no definition to standardize the short sigmoid colon, and the surgical strategy might be different in other medical center. And we did not use indocyanine green (ICG) fluorescence to assess the bowel perfusion, which might influence surgical outcomes. Therefore, multicenter prospective randomized-controlled trials with large samples should be performed.
Conclusion
In conclusion, although there was no significant difference between two surgical procedures for prognosis in SCC patients, the age and the tumor stage might be the independent risk factors for OS and DFS in SCC patients. Moreover, the possible reasons for changing surgical procedures were analyzed in this study, and surgeons should be cautious about the potential risks of difference between various surgical procedures.
Footnotes
Acknowledgments
We acknowledge all the authors whose publications are referred in our article. We thank Xun Lei, a statistician, for the substantial work in the statistical methods. And we thank Melissa Davis for linguistic editing and proofreading during the preparation of this manuscript.
Authors’ Contributions
Wei Tao: Conceptualization, formal analysis, software, and writing—original draft. Fei Liu: Data curation, formal analysis and investigation, and resources. Yu-Xi Cheng: Data curation, project administration, and resources. Bin Zhang: Data curation, project administration, and resources. Xiao-Yu Liu: Data curation, project administration, and resources. Wei Zhang: Conceptualization, supervision, and writing—review and editing. Dong Peng: Conceptualization, project administration, supervision, and writing—review and editing. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This study is supported by CQMU Program for Youth Innovation in Future Medicine (W0190).
Ethical Approval
This study was conducted in accordance with the World Medical Association Declaration of Helsinki and was approved by the Medical Ethics Committee of The First Affiliated Hospital of Chongqing Medical University (K2023-308).