
Abstract
Background
Lung cancer (Lca) is the leading cause of cancer morbidity and mortality worldwide. This study examines the Lca incidence and trends in Lebanon and compares them to regional and global ones. It also discusses Lca risk factors in Lebanon.
Methods
Lung cancer data from the Lebanese National Cancer Registry for 2005 to 2016 was obtained. The age-standardized incidence rates (ASRw) and age-specific rates per 100 000 population were calculated.
Results
Lung cancer ranked second for cancer incidence in Lebanon from 2005-2016. Lung cancer ASRw ranged from 25.3 to 37.1 per 100 000 males and 9.8 to 16.7 per 100 000 females. Males 70-74 and females 75+ had the highest incidence. Lung cancer ASRw in males increased significantly at 3.94% per year from 2005 to 2014 (P > .05), then decreased non-significantly from 2014 to 2016 (P < .05). Lung cancer ASRw in females increased significantly at 11.98% per year from 2005 to 2009 (P > .05), then increased non-significantly from 2009 to 2016 (P < .05). Males' Lca ASRw in Lebanon was lower than the global average in 2008 and became similar in 2012 (34.1 vs 34.2 per 100 000); However, females' Lca ASRw was almost comparable to the global average in 2008 and exceeded it in 2012 (16.5 vs 13.6, respectively, per 100 000). Males’ and Females’ Lca ASRw in Lebanon were among the highest in the Middle East and North Africa (MENA) region but lower than those estimated for North America, China and Japan, and several European countries. The proportion of Lca cases attributed to smoking among Lebanese males and females was estimated at 75.7% and 66.3% for all age groups, respectively. The proportion of Lca cases attributed to air pollution with PM10 and PM2.5 in Lebanon was estimated at 13.5% for all age groups.
Conclusion
Lung cancer incidence in Lebanon is among the highest in the MENA region. The leading known modifiable risk factors are tobacco smoking and air pollution.
Keywords
Background
Lung cancer (Lca) has been the leading cause of cancer morbidity and mortality for several decades, bypassed only by female breast cancer in 2020.1-5 Men have approximately twice the Lca-related morbidity and mortality rates as women, though this proportion varies wildly across regions.1,2 In men, Lca remains the most commonly diagnosed cancer and the leading cause of cancer-related deaths.1,2 In women, Lca is the third cancer-related morbidity (after breast and colorectal cancer) and the second leading cause of cancer-related deaths (after breast cancer).1,2 Lung cancer incidence has increased over the years, reaching around 2.2 million new cases in 2020 (i.e., increased by 36.6% since 2008).1-3 Lung cancer-related mortality reached approximately 1.8 million deaths in 2020, with an increase of 30.4% since 2008.1-3 Although the number of Lca cases has increased over time, the projected age-standardized incidence rate adjusted to the world population (ASRw) per 100 000 person-years has decreased in 2018 and 2020 (13.1 and 13.3, respectively) compared to 2012 and 2008 (14.0 and 15.2, respectively).1-5
Behavioral, environmental, and genetic risk factors are all known to contribute to the formation of Lca tumors.6,7 The leading cause of the global epidemic of Lca is active tobacco smoking.6-9 Lung cancer incidence and mortality rates show a substantial geographic disparity worldwide.1,2 They are 3 to 4 times greater in developed/transitioned regions (e.g., North America and Europe) than in transitioning/developing regions (e.g., Africa).1,2 They follow the chronological patterns of the cigarette smoking epidemic, with around 20-year lag time from a change in smoking prevalence to modification in Lca incidence and mortality rates. 1,2 Radon exposure, classified by the International Agency for Research on Cancer (IARC) as carcinogenic to humans in 1988 (IARC Group 1), is considered the second leading cause of Lca in North America.7,10 In 2013, the IARC concluded that exposure to outdoor air pollution, mainly Particulate Matter (PM), is carcinogenic to humans (IARC Group 1) and causes Lca. 11 Drinking water and food pollution particularly with Arsenic increases the risk of Lca.12-14
According to data from the IARC/World Health Organization, the MENA region’s ASRw of Lca in 2018 was lower than the international rate, ranging from 4.2 per 100 000 in Yemen to 23 per 100 000 in Lebanon. 15 Lebanon is a small Middle Eastern developing country (population estimated at 6 million in 2016). 16 At the time corresponding to the analyzed data in this manuscript, Lebanon had health indices comparable to the Western world 12 and a high-population standard human development index (HDI: .757 in 2017) calculated using the standard HDI formula (i.e., through measuring a country’s average achievement in 3 key dimensions of human development: long and healthy life, being knowledgeable, and having a decent standard of living). 17 Lebanon is a highly urbanized country, with most of the population living in cities and large urban agglomerations. In 2004, Lca was the second most common cancer in men in the country (ASRw: 28.3) slightly behind prostate cancer (ASRw: 28.5), and the third most common cancer in women (ASRw: 11.87) marginally behind colorectal cancer (ASRw: 11.90). 18
This study examines the incidence rates and temporal trends for Lca in Lebanon over 12 years. In addition, it compares incidence rates in Lebanon to those in its geographic region, namely the Middle East and North Africa (MENA) region, as well as other countries/regions worldwide. This study also investigates the impact of smoking and air pollution on the incidence of Lca in Lebanon and discusses the various risk factors that have contributed to the Lca ASRw in Lebanon over time. It concludes with recommendations for effective Lca prevention and screening.
Materials & Methods
The Lebanese National Cancer Registry
Following the civil war, the Lebanese National Cancer Registry (NCR) was restarted formally in 2002; this registry maintains an almost absolute sum of all incident cancer cases nationally. The capture system (data collected passively from physicians' reports) and the recapture system (data collected actively from histopathological and hematological laboratories) are constantly assembling NCR data.18,19 The NCR includes most cancer cases (more than 90%) in Lebanon 18 but lacks the in-situ lesions. The Lebanese NCR soft data are available on the Ministry of Public Health (MoPH) Website; the available data covers the years 2005 to 2016. 19
Analysis of Twelve-Year Trends From 2005 to 2016
In this cohort study, Lca data include diagnoses with the International Classification of Diseases, 10th revision (ICD-10) codes C33 and C34 (i.e., lung & bronchus cancer). The age-standardized incidence rate adjusted to the World standard population by Doll as the reference population (ASRw), 20 and the age-specific incidence rates expressed per 100 000 population 21 were retrieved from the Lebanese NCR data hosted on the MoPH website 19 for twelve consecutive years (from 2005 to 2016).
The ASRw is a weighted average of the age-specific incidence rates per 100 000 persons, whereby weights are the proportions of persons in the corresponding age groups of a standard population. It is important to use standardization when comparing different populations with different age structures. The world standard population is the most commonly used standard population, which is drawn from a pooled population of several countries. In this study, the ASRw was computed using the modified world standard population by Doll as the reference population. 20 The age-specific incidence rate is the number of new cancer cases occurring during a specific period, in a population of a specific age and sex group, divided by the number of mid-year population of that age and sex group. 21
For the ASRw and the age-standardized rates, the annual percent change (APC) of Lca incidence rates over the years were computed by the Joinpoint Regression Program (JRP) 4.7.0.0 with a statistical significance level defined at a P-value <.05. 22
Projections of the Lca Incidence Using Population Growth and Lca Trends
The Nordpred software package 23 (a package of R and S-PLUS functions) available from the Cancer Registry of Norway Web site (kreftregisteret.no/software/nordpred) was used to estimate future Lca incidence in Lebanon. Nordpred is a statistical software that is used most commonly worldwide for projecting Lca rates using Age-Period-Cohort models. 24 This software employs a special version of the Age-Period-Cohort regression model (Poisson regression method) and population growth to forecast trends in Lca incidence. 23 The first age group considered for analysis is the 1 with more than 3 cases per block per year (i.e., 35-39 years in this study). Predictions for age groups below this limit is based on average rates from the last 10 years. Also, for each period, ASRw was calculated based on the standard world population. 23
Comparison of Lca Incidence Rates in Lebanon to Other Countries
Lung cancer ASRw and age-specific rates in Lebanon were then compared to age-standardized and age-specific incidence rates from other countries with cancer data available for a comparable time-period, including a few countries from the MENA. These figures were obtained from the Cancer Incidence in 5 Continents Time Trends (CI5plus), 25 Cancer Incidence in 5 Continents Volume XI (CI5XI), 26 or the Regional or Country National Cancer Registry.27-29
The CI5plus and CI5XI rates are computed based on high-quality population-based cancer registries. For comparison, we included countries geographically nearby Lebanon and randomly selected countries from the MENA region and other parts of the world.
Estimation of the Population Attributable Fraction of Smoking and Air Pollution on Lca Incidence in 2016 in Lebanon
The population attributable fraction (PAF) is the percentage of disease cases that could be prevented if the population had no exposure to a risk factor. It evaluates both the prevalence of exposure and the elevated risk brought on by it. Therefore, measures to lower the burden of cancer in the population can be planned and prioritized using PAF estimations.
To quantify a risk factor’s contribution to cancer burden (PAF), 2 major values are required: the prevalence of the population exposed to the risk (i.e., the prevalence of exposure or Pe) and the relative risk of cancer attributed to that exposure or risk factor (RRe). Cancers caused by a risk factor are usually the result of a long period of exposure to that risk factor (i.e., lag time); for most cancer risk factors, a latent period of 10 years is considered adequate. 30
In the case where the risk factor presents 1 exposure level, the following classic formula was applied: 31 PAF = Pe (RRe-1)/[1+ Pe (RRe-1)].
We primarily relied on World Health Organization estimates or population-based reports or studies with a representative sample of the Lebanese population that identified the population proportion at risk around 10 years ago because the risk impact is not immediate and we require at least a 10-year lag to draw any conclusions. 30 The World Health Organization estimate of current tobacco smoking prevalence in Lebanon in 2005 was used in the analyses. 32 Studies on air pollution conducted between 2003 and 2007 measured PM10 and PM2.5 the annual averages concentrations (for 24 hours every 6-days) at different points around Lebanon’s Greater Beirut area, and the average of the annual averages were used to determine the prevalence of Lebanese exposure to PM (PM10 and PM2.5) air pollution.33,34 Analysis also counted that the Greater Beirut area is home to more than two-thirds of the Lebanese population and that the World Health Organization’s annual standard averages for PM10 and PM2.5 are 20 g/m3 and 10 g/m3, respectively. 33
Multiple adjusted Lca relative risks for each Lca risk factor (i.e., smoking and air pollution with PM) were obtained from meta-analyses of epidemiological studies to complete the figures required for analysis.35,36
Results
Over the 12-year study period (2005-2016) in Lebanon, Lca ranked second in males and females after prostate cancer and breast cancer, respectively. During the study period, a total of 11 570 incident cases of Lca were reported (an average of 964 new cases per year), with 91.2% and 85.6% of cases affecting men and women aged 50 years or more, respectively. There was a male-to-female ratio of 2.2. During the study period, Lca ASRw fluctuated between 25.3 and 37.1 (average: 32.2) per 100 000 males, and between 9.8 and 16.7 (average: 14.4) per 100 000 females. The historical dynamics of Lca in Lebanon revealed that this cancer incidence has significantly increased since 1964 when the Lca ASRw was around 8.8 in males and 1.5 in females.
37
Over the 12-year study period (2005-2016), the age-specific incidence rates increased with age, peaking in the age groups 70-74 for males and 75+ for females (Figure 1). Age-specific incidence rates (per 100 000 population) for lung cancer (C33-C34), Lebanon 2005-2016.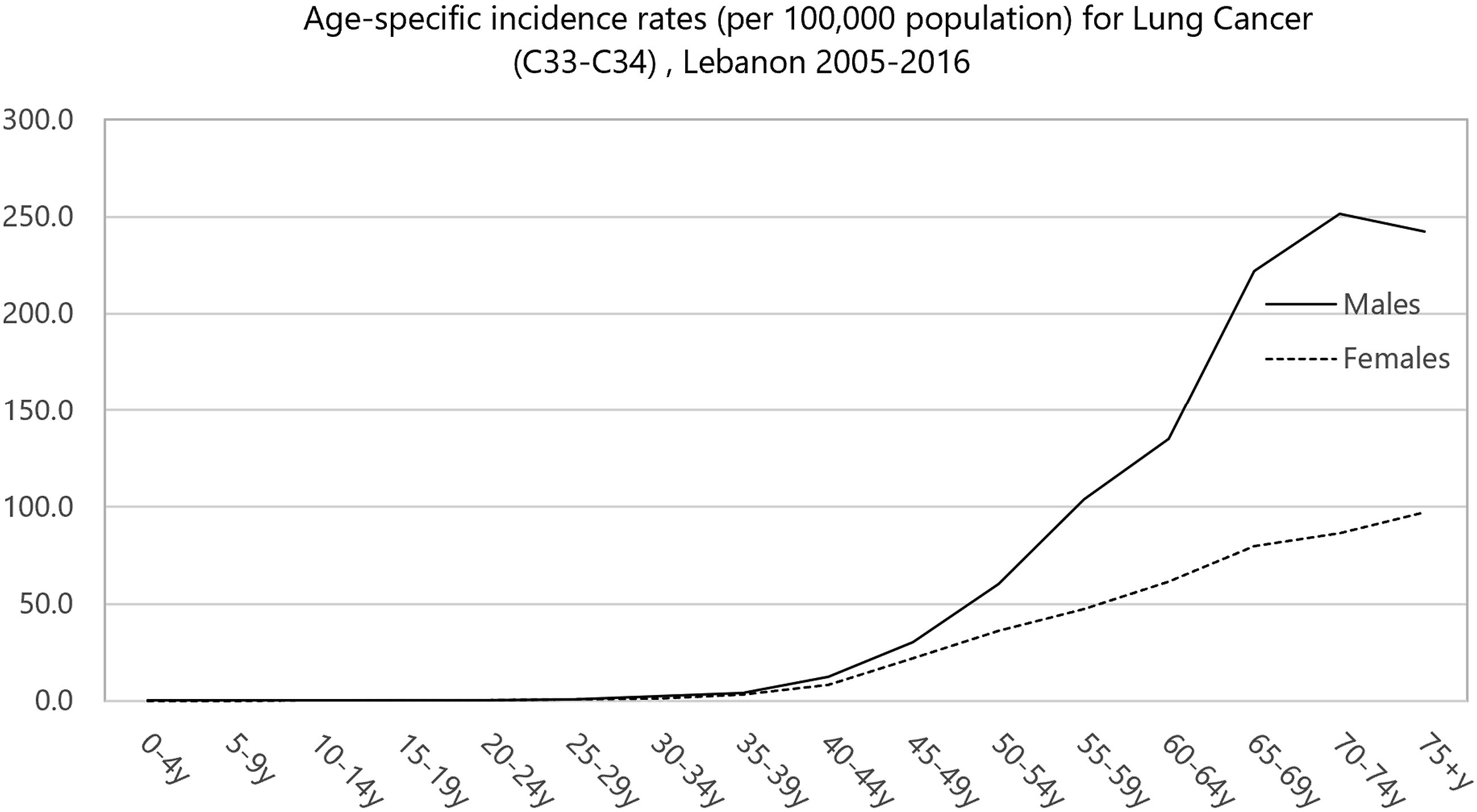
Lung and Bronchus Cancer Age-Standardized Incidence Rate (World Population) and Age-Specific Incidence Rates among Males and Females in Lebanon in the Years 2005-2016.

^ASRw: Age Standardized Rate (world); *APC (Annual Percent Change) significantly different from zero.

Age-standardized incidence rates (ASRw) of lung and bronchus cancer in males and femles, Lebanon 2005-2016:0 Joinpoints.
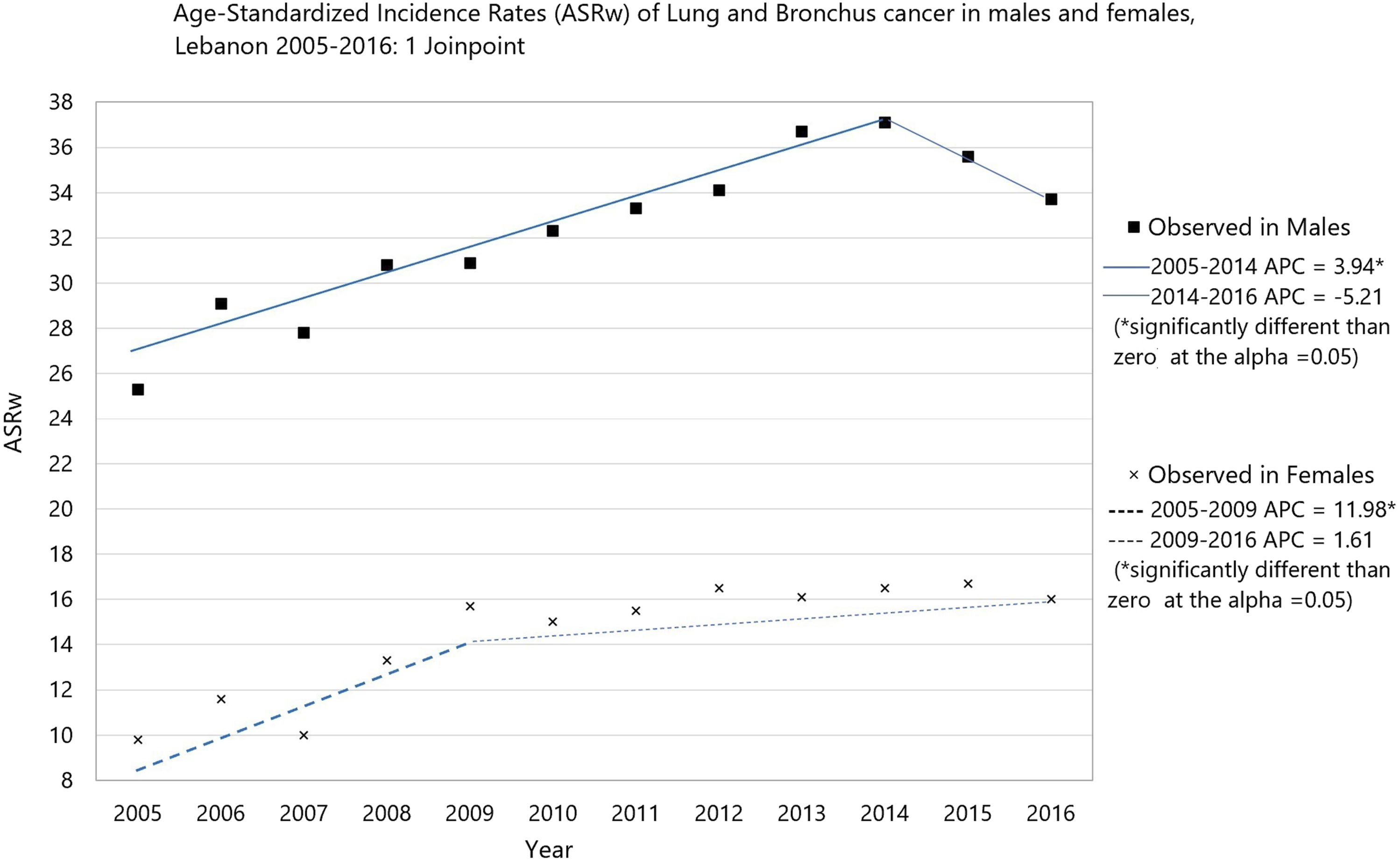
Age-standardized incidence rates (ASRw) of lung and bronchus cancer in males and femles, Lebanon 2005-2016:1 Joinpoints.
Projected Lca ASRw in 2020
Using the Nordpred software package, 23 the Lca ASRw per 100 000 population in 2020 was estimated to be 28.5 in males and 14.0 in females, i.e., lower than the estimated figures reported by Globocan 2020 for Lebanon (24.4 in males and 13.5 in females). 1
Comparison to Countries in Different Regions of the World
Annual Incidence Rates (per 100 000) of Lung Cancer in Males of Different Middle East and North Africa (MENA) and Non-MENA Countries.

ASRw: Age Standardized Rate (world); MENA: Middle East and North Africa.
Annual Incidence Rates (per 100 000) of Lung Cancer in Females of different Middle East and North Africa (MENA) and non-MENA countries.

ASRw: Age Standardized Rate (world); MENA: Middle East and North Africa.
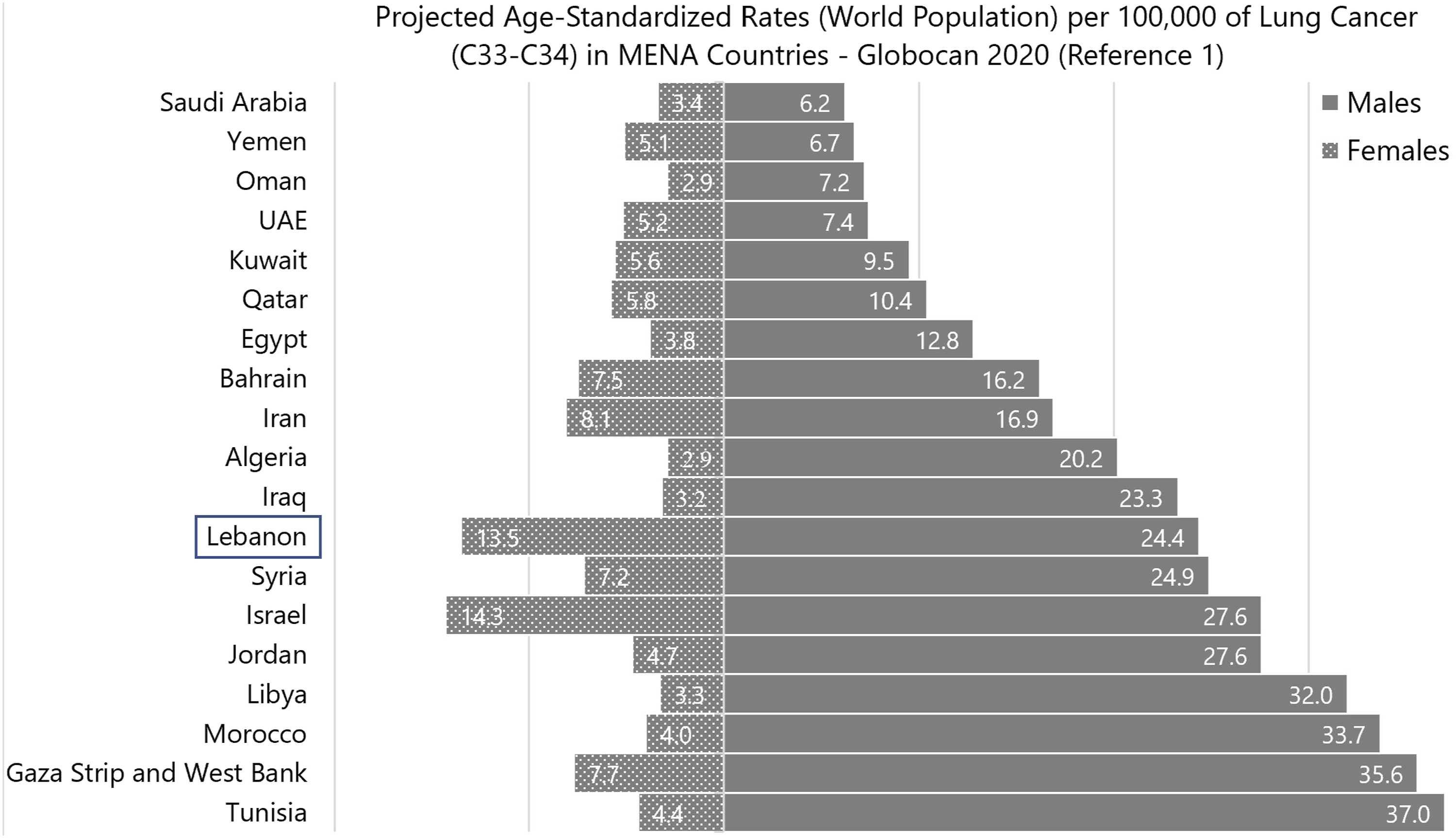
Projections from published reports of the IARC/Global Cancer Statistics (IARC/Globocan) revealed an increase in Lca ASRw over the years in both males and females in the Western Asia region (Figure 4). Lebanon’s estimated figures in 2020 were relatively high-intermediary in males (ASRw: 24.4) and the top second in females (ASRw: 13.5) compared to other countries in the MENA region (Figure 5). Saudi Arabia and Yemen had the lowest estimated male figures in the MENA region (ASRw: 6.2 and 6.7, respectively), while Algeria and Oman had the lowest estimated female figures (ASRw: 2.9). (Figure 5). Lebanon’s Globocan projections of Lca ASRw for 2020 (ASRw: 24.4 in males and 13.5 in females) were lower than our projections based on NCR data for the same year (ASRw: 35.2 in males and 17.1 in females) (Figure 5). Projected-age-specific incidence rates (per 100 000 population) of lung cancer by regions based on Globocan 2008, 2012, 2018 and 2020. Projected-age-standardized rates (world population) per 100 000 of lung cancer (C33-C34) in MENA countries-Globocan 2020 (Reference 1).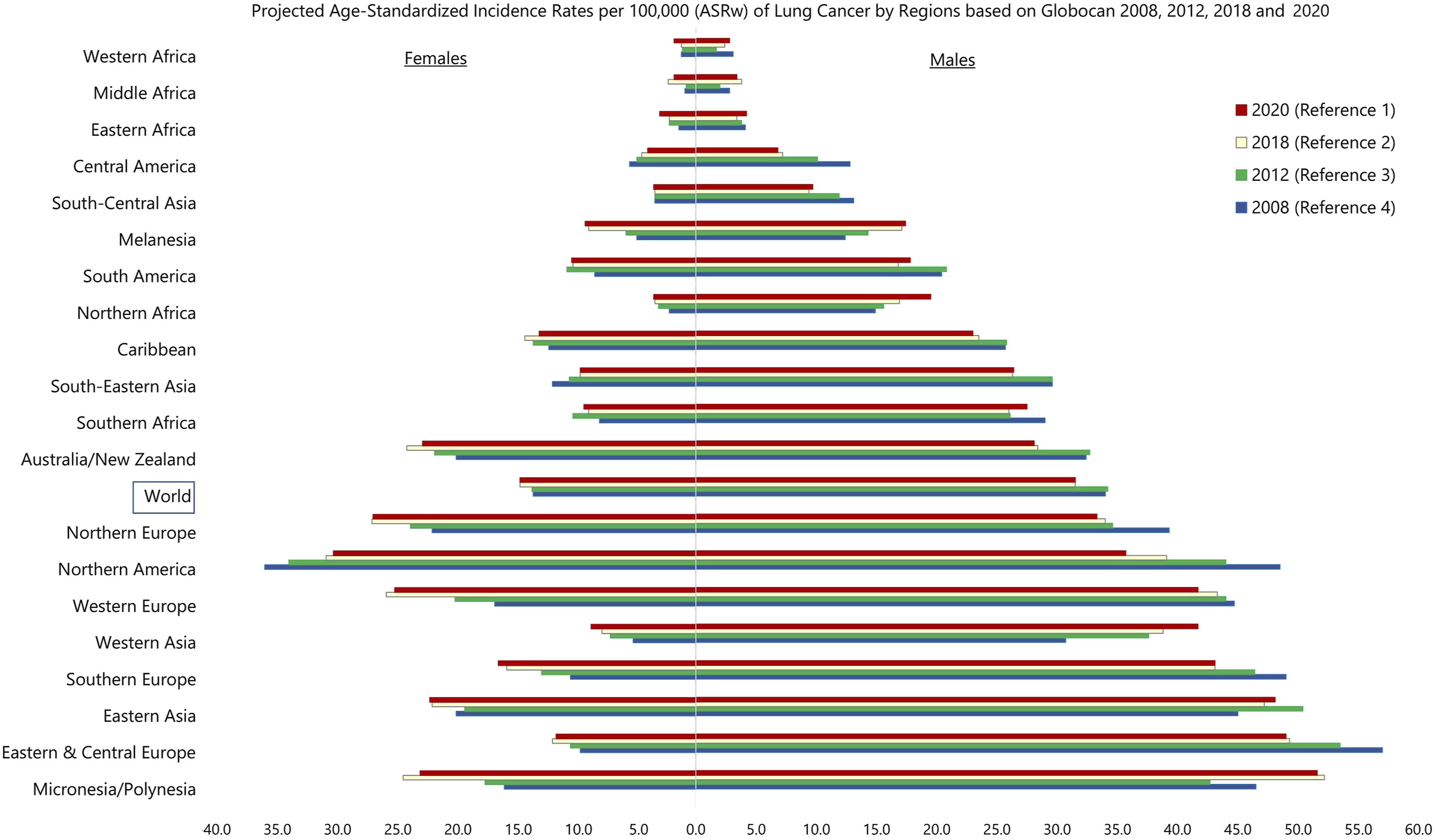
Estimation of the Population Attributable Fraction of Smoking and Air Pollution on Lca Incidence in 2016 in Lebanon
Smoking
By applying the modified Levin formula, we used Pe to represent the percent of males’ current tobacco smokers 32 (41.1%), and RRe to represent the relative risk due to current smoking 35 (7.33). Lung cancer estimate cases attributed to current tobacco smoking among Lebanese males in 2016 were 72.23% of cases for all age groups. Similarly, we applied the formula for females considering that the used Pe and RRe were 28.7% and 6.99%, respectively.32,35 Therefore, Lca estimate cases attributed to current tobacco smoking among Lebanese females in 2016 were 63.22% of cases for all age groups. However, these rates are underestimated since they did not account for the Lca relative risks associated with former and second-hand (passive) smoking, respectively.
Air pollution with PM
By applying the same formula, the Pe1 and Pe2 were the percent of the Lebanese population exposed to air pollution with PM10 and PM2.5 (85.0% and 85.0%, respectively),33,34 while the RRe1 (1.08) and RRe2 (1.09) were the relative risks due to exposure to PM10 and PM2.5, respectively. 36 Lung cancer cases attributed to air pollution with PM10 and PM2.5 in Lebanon in 2016 were estimated to be 6.37% and 7.11% of cases for all age groups of both genders, respectively (i.e., a total of 13.48% of all Lca cases).
Discussion
In Lebanon, both males and females' Lca ASRw increased significantly over the years. These rates are not far from worldwide estimates but higher than the rates of Arab countries in the MENA region.
The etiology of Lca is not yet clear, and is multifactorial.6-11 Exposure to tobacco smoke, including second-hand smoke, is the most common cause of Lca. In high-income countries, around 90% and 80% of Lca cases among men and women, respectively, are attributable to tobacco use,12,38,39 i.e., higher than the estimates in Lebanon which did not count for the Lca relative risks associated with solo Arguileh (water pipe) without cigarettes smoking and passive (secondhand) smoking, respectively. A systematic review and meta-analysis concluded that around 15.5% of Lca cases among never smokers in China are potentially attributable to passive smoking. 40 Other modifiable Lca risk factors include preexisting lung diseases such as tuberculosis, indoor air pollution with radon gas or from wood and coal burning for cooking and heating, environmental or outdoor air pollution, Arsenic in drinking water, and occupational exposure to asbestos, crystalline silica, radioactive ores such as uranium, diesel exhaust, and inhaled chemicals (such as arsenic, beryllium, cadmium, silica, vinyl chloride, nickel compounds, chromium compounds, coal products, mustard gas, and chloromethyl ethers).6-9,12-14 Non-modifiable Lca risk factors include age, gender, race, and genetic susceptibility.6-8 In addition to genetic susceptibility, environmental risk factors are reported to play a predominant role in Lca in never-smokers, including second-hand smoke exposure, environmental PM, occupational exposures, indoor air pollution, and radon. 7
Tobacco Smoking
Tobacco Smokers are 22 times more likely to develop Lca than nonsmokers.
41
Cumulative tobacco smoking increases Lca risk (i.e., number of pack-years).
42
Nonsmokers exposed to secondhand smoke at home or work have a 30% higher Lca risk.
42
Tobacco use is declining worldwide, mostly in high-income countries like the UK, but at a rate not high enough to reduce cancer incidence.41,43 The goal of reducing worldwide adult tobacco use by 30% by 2025 probably won’t be met.
41
The prevalence of tobacco use in Lebanon (49.3% in adult males and 36.5% in adult females in 2010) is among the top twenty in males and top 7 in females worldwide.44,45 In MENA region, it is the second-highest rate among males, just behind Tunisia (average in the region: 37.8% in males), and the highest rate among females (average in the region: 4.2% in 2010 in females) mainly because of cultural prohibitions against women smoking in other Arab countries.
44
In the past decade, tobacco use has declined in Morocco, Tunisia, and Turkey while it has remained stable in Lebanon and Egypt.
44
However, the prevalence of tobacco smoking among persons aged ≥15 years in Lebanon is on the rise (Figure 6) and the projections for the year 2025 are 55.4% in males and 37.7% in females.
45
Moreover, previous surveys show that cigarette and waterpipe smoking is prevalent among Lebanese adults, especially men.46-49 Lebanese adults smoke heavily, consuming 12.4 packs per month on average.
49
The 2016 WHO STEPS survey revealed that 38.0% of Lebanese adults (18 to 69 years) are tobacco smokers (47.6% in men and 29.0% in women).
48
Furthermore, many citizens are former smokers (6.9% men and 3.3% women),
46
and many others are at risk of passive or secondhand smoking due to unsafe indoor air pollution from smoking in Lebanon’s homes, workplaces, and public places.
50
A recent cross-sectional study assessed Lebanese adults' knowledge and beliefs about cancer risk factors and found that while high knowledge scores were associated with low-risk behavior for some risk factors, this was not the case for cigarette smoking.
51
It is important to notice that Lebanon has very weak tobacco control regulatory environments where smoking prevails in youth and adults. Lebanon signed the WHO Framework Convention on Tobacco Control (WHO FCCT) in 2004 and ratified it in 2005. Lebanon’s Tobacco Control Law went into effect at the end of 2011 to ban smoking in public places, ban tobacco advertising, and increase health warnings on cigarette packs by 40%.
52
The WHO’s April 2016 Lebanon needs assessment mission found that tobacco industry interference has weakened the Tobacco Control Law.
52
Age-standardized estimates of current tobacco use and tobacco smoking in Lebanon (% of adults).
Environmental Risk Factors for Lca
Exposure to radon
Another major risk for Lca is radon, a radioactive gas naturally formed by the breakdown of uranium-containing rocks and soils.6,10,12,53 Outdoor radon is diluted quickly by atmospheric mixing and poses no threat to human health. Humans' primary natural radiation source is indoor radon. Indoor radon is the primary source of natural radiation for humans. 54 The major sources of indoor radon are soil around the foundation, building materials, fuels, and domestic water.53,54 Even low indoor radon levels contribute to Lca, according to studies.53,54 Soil, building foundations, and ventilation affect indoor radon levels. Basements and lower floors can accumulate unsafe levels. 7 Radon causes an estimated 3 to 14% of Lca, varying with the average level of radon in the country and the tobacco smoking prevalence. 54 Regardless of sex, radon exposure increases Lca risk in smokers compared to nonsmokers. 54 Despite seasonal variation, indoor radon in Lebanon does not appear to be a public health risk, and its concentrations (median and maximum concentrations of 17.8 and 80 Bq/m3, respectively) remain significantly below the International Commission on Radiological Protection’s lowest reference level (100 to 300 Bq/m3).55,56
Air pollution
Air pollution, including petrochemical air pollutants, is a risk factor for Lca.10,57-62 Air pollution and tobacco smoking may have a synergistic, multiplicative effect on Lca rates. Particulate matter from urban air has been the most studied Lca risk factor. International Agency for Research on Cancer classified outdoor air pollution and PM10 (PM with a diameter of less than 10 microns) as carcinogenic to humans in 2013. This classification was made in light of several high-quality epidemiologic studies conducted in North America, Europe, and Asia that consistently found a robust association between PM exposure and Lca, even after adjusting for major Lca risk factors like tobacco smoking.10,57 A systematic review and meta-analysis found consistent evidence of an association between Lca and NO2, as a proxy for traffic-related air pollution exposure. 61 Also, a large prospective study in the UK Biobank found that long-term exposures to air pollution (PM2.5, PM10, NOx) may raise the incidence of Lca, particularly in individuals with high genetic risk. 57 Multiple studies in Greater Beirut revealed high annual average concentrations of PM10, PM2.5, and, NO2 which surpass WHO recommendation standards.33,34,63 Lebanon’s air pollution sources emit carbon monoxide (CO) and dioxide (CO2), nitrogen oxides (NOX: NO and NO2), sulfur dioxide (SO2), fine PMs (mainly PM10 and PM2.5), and polycyclic aromatic hydrocarbons (PAHs).62-73 The national air quality monitoring network (AQMN) was installed in 2013 and expanded in 2017 by the Lebanese Ministry of Environment in coordination with university researchers. The levels of various air pollutants in Lebanon reported intermittently by the AQMN over the past decade show that levels of gas pollutants including NO2, PMs and their chemical contents, and Volatile Organic Carbons exceed WHO recommended limits for annual averages.64,65 Lebanon air pollution is among the highest in the MENA Region. 72 Unregulated private diesel-fueled power generators in Lebanon’s streets and buildings, which cause petrochemical-based air pollution in residential areas, along with heavy traffic in Greater Beirut are the leader sources. Small businesses ignoring precautions and uncontrolled power plants are the following sources. In recent years, new events have increased air pollution in Lebanon, especially after the Ammonium Nitrate Beirut blast in August 2020, private Diesel generators working almost 24/7 to meet power demand after the government power grid failed, and environmental health degradation. Regional transportation affects Lebanon’s ozone levels. 68 In 2018, Lebanon’s 1996 air quality law was replaced by a new one (Law no.78 of 2018 on Air Quality Protection). 74 The new legislation set annual PM2.5, PM10, CO, NOx, O3, etc. standards based on WHO guidelines. So far, little has been done to reduce the air pollution.
Water and vegetables pollution
South America compelling evidence suggests that drinking water containing Arsenic, a naturally occurring metalloid in the earth’s crust, increases the risk of Lca.12,13 Most high-income countries use a 10 μg/L drinking water standard, consistent with the WHO’s provisional maximum concentration. 14 Even at low concentrations, chronic Arsenic in drinking water has been linked to cancer and other health problems in humans. 14 Moreover, Cadmium exposure is also associated with Lca. Cadmium exposure in non-smokers is primarily through food and, to a lesser extent, air, water, soil, and dust. 13 Lebanon chlorinates drinking water at the source (bore holes and springs) or at a centralized plant. Its quality deteriorates during distribution (cross contamination by wastewater network, rusting water conduits, and sometimes by pollution/waste from industries and thermal power plants, dumpsters, etc.) to contain fecal coliforms (mainly Escherichia coli), pesticides, and heavy metals including Arsenic and Cadmium.75-77 Population growth and Syrian refugees, urbanization, economic crisis, and climate change have increased water demands and wastewater generation in Lebanon. 64 Lebanon’s water is polluted and poorly conserved, causing chronic water shortages, a lack of safe and improved water resources, and unconventional water sources. 64 Moreover, numerous environmental components (coastal water near industrial sites, agricultural soil, vegetables, etc.) in Lebanon are polluted with Arsenic and Cadmium, according to studies. 64
Asbestos
Occupational carcinogen exposure accounts for around 5-10% of Lca. 7 Asbestos is a naturally occurring mineral silicate fiber of amphiboles (actinolite, amosite, anthophyllite, crocidolite, tremolite) and serpentine (chrysotile) used in construction since the 19th century.7,13 The six forms of asbestos are lung carcinogens, but chrysotile’s potency may be lower.7,13 Chrysotile fibers have the strongest association with thoracic cancer, particularly mesotheliomas. 7 Asbestos exposure increases Lca risk 5-fold. 7 Asbestos and smoking increase Lca risk and have a synergistic effect.7,13 The entire amount of asbestos used in Lebanon is imported. Half of the 235 tons imported in 1996 went to the Chekka Eternit factory. Since 1962, this factory has made pipelines and construction materials with cement and asbestos. In 1998, Lebanon banned all asbestos imports (i.e., raw materials) except chrysotiles. Meanwhile, the factory took steps to reduce fiber levels in the manufacturing air until it closed permanently in 2000 due to financial issues. 78 Nowadays, there are asbestos-containing pipes that were imported and installed to irrigate some areas of the Beqaa region, promoting the consumption of asbestos fibers by people who consume Beqaa food. 78 Furthermore, the Beirut blast in August 2020 damaged many of the heritage-vulnerable buildings, resulting in illegally dumped debris and hazardous substances (such as asbestos) that were not properly handled. 64
Chronic Inflammation of Lungs From Infection
Lung cancer is associated with a history of lung tuberculosis (TB), and with positive Chlamydia pneumoniae antibodies regardless of smoking status and with significant delay.6,7 In developed countries, the prevalence of tuberculosis has declined. Lebanon has a low TB burden, with around 13 cases per 100 000 people, and a treatment coverage of 76%. 79 The trend of TB notification increased in 2012 onwards with the influx of Syrian refugees and the migrant workforce present in the country, to drastically drop in 2020-2021 mainly because of the decline in notification among migrants. 79 The rate of TB cases among non-Lebanese gradually increased between 2006 and 2020 then dropped to 50% in 2021. 79 There is no published data about the prevalence of people with positive Chlamydia pneumoniae antibodies in Lebanon.
Genetic Susceptibility
Based on the Genome-wide association studies (GWAS), many acquired genetic mutations (susceptibility loci) are associated with Lca with different strengths of evidence.7,80,81 These mutations are mainly triggered by tobacco smoking and environmental pollution. Molecular genetic analysis of epidermal growth factor receptor (EGFR) and Kirsten rat sarcoma viral oncogene (KRAS) mutations in non-small-cell Lca (NSCLC) are nowadays essential aspects of cancer diagnosis and management and are utilized in Lebanon. 82
Moreover, a genetic predisposition to Lca is confirmed since not all tobacco smokers develop Lca.7,83 A positive family history of Lca, mostly in first-degree relatives, was reported to be associated with an increased risk of developing Lca by 2 to 4-folds after controlling for personal smoking history. 7 Studies revealed several genes associated with inherited Lca syndromes (e.g., EGFR T790M, TP53 (Li-Fraumeni syndrome), BRCA mutations, Human epidermal growth factor 2 (HER2), YAP1, CHEK2, etc). 83 However, genetic testing options for Lca are very limited, and there are no guidelines for genetic testing yet. 83
Limitations of the Study
Because of the unavailability of data, the analysis only considered smoking and air pollution as potential risk factors for Lca; it did not account for other risk factors (e.g., secondhand smoke, water and vegetables pollution, cooking smoke, previous radiation therapy, exposure to other carcinogens such as radon gas and asbestos, family history of Lca, etc.) or covariates (e.g., dietary habits, body mass index, socioeconomic status, etc.), which could have introduced bias.
Our study is based on the cancer data published by the MoPH on its official website. Despite the improvements done in data collection for the NCR, information on collected cases is still incomplete lacking precancerous and in-situ conditions, risk factors, as well as mortality and survival rates. The Lebanese government is yet to play its role in limiting the burden of Lca in Lebanon, through: (1) implementing preventive measures and regulations that decrease the smoking rate, air and water pollution in Lebanon; (2) making screening/early detection with low dose helical computed tomography (LDCT) accessible at an affordable price to high‐risk populations as recommended by the United States Preventive Services Task Force (USPSTF); 84 (3) organizing an annual national awareness campaign, along with a national screening/early detection program to Lebanon.
Conclusion
The growing Lca incidence in Lebanon is among the highest in the region. Tobacco smoking and air pollution are the most significant modifiable Lca risk factors in Lebanon. The Lebanese government should revisit, update, and strengthen the existing tobacco control laws. In the meantime, it should fund a comprehensive national tobacco control program and a national Lca early detection program. Monitoring and improving air quality in Lebanese urban communities is another crucial governmental task to be achieved in the next few years.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval is not applicable for this article. There are no human subjects in this article and informed consent is not applicable.
Availability of Data and Materials
Data is available for the public on the website of the Ministry of Public Health, Republic of Lebanon.