
Abstract
Background
In non-small cell lung cancer (NSCLC), patients with extrathoracic metastases typically have a poor prognosis, with systemic chemotherapy being the standard care. The full potential of primary resection therapy (PRT) in these patients, especially during the immunotherapy era, is not fully established. Additionally, the effectiveness of systemic preoperative therapy in this context is unclear.
Methods
This retrospective study identified NSCLC patients with extrathoracic metastases from the Surveillance, Epidemiology, and End Results (SEER) database from 2010 to 2019. We compared the survival rates of those treated with just chemotherapy vs those receiving both chemotherapy and PRT.
Results
In a study of 41 909 patients with extrathoracic metastatic NSCLC receiving chemotherapy, we found that adding PRT significantly increased overall survival (median OS post-PSM: 18 months vs 11 months, P < 0.001). However, in the immunotherapy era, its effectiveness was less pronounced (HR: 0.56 vs 0.7, P for interaction = 0.011). For patients who have metastases to multiple distant organs, combined distant organ and distant lymph node metastases, or lung metastases, no additional survival benefit from PRT was observed (all P > 0.05). Patients receiving systemic preoperative therapy before PRT had significantly better outcomes than those who did not (HR = 0.69, P < 0.001). A predictive nomogram was developed and validated, showing AUCs of 0.751 and 0.766 in the training and test sets.
Conclusion
In both pre- and post-immunotherapy eras, patients with extrathoracic metastatic NSCLC benefit more from adding primary tumor resection to chemotherapy, especially those with preoperative systemic therapy. We created a precise nomogram to identify the best candidates for PRT among patients with extrathoracic NSCLC metastases.
Keywords
Introduction
Lung cancer is the leading cause of cancer-related deaths globally, 1 accounting for approximately 18% of all cancer fatalities with an estimated 1 796 144 deaths in 2020. Despite advances in treatment, about 75% of non-small cell lung cancer (NSCLC) patients are diagnosed at advanced stages, 2 often with a poor prognosis due to distant metastases, resulting in a median survival of only 5 months. 3 Notably, patients with extrathoracic metastases tend to have a poorer survival rate compared to those with intrathoracic metastases. 4
For these patients, systemic chemotherapy is commonly the primary treatment, but unfortunately, the overall prognosis remains poor. A small number of studies indicate that Primary Resection Therapy (PRT) may offer a survival benefit in patients with extrathoracic metastases, particularly for those with a limited number of metastases.5-7 However, the effectiveness of local surgical resection in advanced NSCLC continues to be debated and is not yet clearly established. 8 As a result, it is crucial to select patients carefully for surgical resection, especially in cases of lung cancer with extrathoracic metastases. 9 This consideration becomes even more significant in the context of immunotherapy, where the role and efficacy of surgery might be lessened.10,11
Moreover, the necessity of preoperative systemic therapy or neoadjuvant therapy to stabilize the disease in patients with extrathoracic metastases undergoing PRT remains uncertain. Limited retrospective studies suggest that preoperative neoadjuvant therapy is an independent factor in stage IV resection of the primary tumor. 12 Larger studies are urgently needed to demonstrate the role of neoadjuvant and postoperative systemic therapy in patients with distantly metastatic NSCLC.
Therefore, we analyzed the most recent data from the SEER database to explore the differences in prognosis between patients with extrathoracic metastases treated with chemotherapy combined with PRT vs chemotherapy alone. Additionally, our study examined the impact of PRT in both pre- and post-immunotherapy eras. To accurately determine the NSCLC patient group most likely to benefit from this combined treatment approach, we developed a detailed and precise nomogram.
Materials and Methods
Data Source and Research Design
This retrospective study analyzed data representing approximately 27% of the U.S. population, derived from the SEER database [SEER 17 Regs Research Data, Nov 2022 Sub (2000-2020)]. Our focus was on NSCLC patients diagnosed with extrathoracic metastases. The inclusion criteria were: (1) Diagnosis of at least one of the following metastases: brain, liver, bone, or distant lymph nodes; (2) Histological confirmation of NSCLC, with specific types including Adenocarcinoma (AD), indicated by SEER histologic codes 8140, 8144, 8230, 8250, 8255, 8260, 8290, 8310, 8323, 8333, 8401, 8480, 8490, 8550, 8570, 8571, 8574; Squamous Cell Carcinoma (SQCC), defined by histology codes 8052, 8070-8075, 8083, 8084, 8123; Large Cell Carcinoma (LCC), identified by histology codes 8012-8014, 8031-8033, 8046, 8082; and other NSCLC types coded as 8022, 8200, 8240, 8430, 8560, 8562, 8980; (3) Lung as the primary cancer site, confirmed by international standards. Exclusion criteria encompassed cases with indeterminate T and N stage classification, non-lung primary cancer sites, ambiguous race, treatment status, survival time, primary site details, laterality, uncertain metastasis resection status, and patients below 20 years of age (Figure 1). The reporting of this study conforms to TRIPOD guidelines.
13
Flowchart of the study.
Variable Selection
In this study, we meticulously gathered and analyzed patient data, encompassing the year of diagnosis, demographic details like age, gender, and race, as well as crucial medical information. This medical data included the histological type of the tumor, tumor grading, and TNM stage, which was reassigned in accordance with the eighth edition criteria. Additionally, we considered the site and laterality of the tumor, surgical interventions, and recommendations for surgery, type of surgery performed, lymph node clearance, metastasectomy procedures, chemotherapy, radiotherapy, and the sequence of systemic therapy in relation to surgery. We also recorded the specific locations of metastases, the number of metastatic sites, marital status, and overall survival (OS) as outcome variables. The number of distant metastases was defined as the number of distinct metastatic sites (e.g., brain, liver, bone, distant lymph nodes). In this study, distant lymph node metastases were defined as the spread of cancer to lymph nodes that are not part of the primary regional nodes associated with the primary lung tumor. For lung cancer, examples include supraclavicular and para-aortic nodes, while lymph nodes near the primary tumor (e.g., hilar nodes) were considered regional and not classified as distant metastases. Additionally, we evaluated cancer-specific survival (CSS) as an outcome to further validate the model. CSS was defined as the time from diagnosis to death directly attributed to lung cancer, excluding deaths from other causes. Moreover, aligning with the FDA’s approval of Nivolumab in 2015, our study distinguished between the immunotherapy era (2016 and later) and the pre-immunotherapy era (before 2016).
Statistical Analysis
In this study, all data processing, visualization, and statistical evaluations were conducted using R Studio, version 4.2.1. We compared the group receiving chemotherapy alone to those receiving a combination of chemotherapy and PRT using the chi-square test to assess differences. To enhance comparability, we employed propensity score matching (PSM) to balance the data between the chemotherapy + PRT group and the chemotherapy group in a 1:4 ratio. The P-values from the chi-square tests were greater than 0.05, ensuring no significant differences in clinical characteristics between the matched groups. The Kaplan-Meier method and log-rank test were utilized for survival analysis regarding OS. For logistic and Cox regression analyses, we deemed a Variance Inflation Factor (VIF) of 5 or lower as indicative of no significant multicollinearity. We randomly divide the entire set into 7:3 training and testing sets using the “caret” package. The development of nomograms and calibration plots involved the use of R’s “rms” package. Additionally, Receiver Operating Characteristic (ROC) curves were generated via the “timeROC” package. The determination of statistical significance was based on two-tailed tests, setting the significance threshold at P < 0.05.
Results
Characteristics and Prognosis of Patients Before and After PSM
Our analysis showed notable differences in survival times among extrathoracic metastatic NSCLC patients based on treatment type: palliative care (1 month, N = 4 1538), PRT alone (6 months, N = 778), chemotherapy alone (9 months, N = 4 1909), and Chemo-PRT (18 months, N = 1225) (Figure 2(A)). These findings highlight the limited efficacy of palliative care and PRT alone, with the latter showing poorer outcomes than chemotherapy alone and not aligning with standard treatment guidelines. Therefore, the study focused on patients receiving either chemotherapy alone or in combination with PRT. Kaplan-Meier curves illustrating survival outcomes in NSCLC with extrathoracic metastases (A) Patients with different treatment modalities (B) Patients receiving chemotherapy at different metastatic sites (C) Patients from the chemotherapy group recommended for Primary Resection Therapy (PRT) but not receiving it vs those who received PRT (D) Chemotherapy alone group vs chemotherapy in combination with PRT after Propensity Score Matching (PSM).
Clinical Characteristics of the Chemotherapy Group and Chemotherapy + PRT Group Before and After PSM.

PRT: Primary Resection Therapy; AD: Adenocarcinoma; SQCC: Squamous Cell Carcinoma; LCC: Large Cell Carcinoma.
Our study showed that NSCLC patients with multiple or combined organ and lymph node metastases had poorer prognosis compared to those with single organ and lymph node metastases (Figure 2(B)). Additionally, we compared patients recommended for PRT during chemotherapy but who didn’t receive it, against those who underwent PRT. The prognosis was significantly better in the latter group (11 months vs 18 months, P < 0.001) (Figure 2(C)).
To further compare the prognostic differences between the chemotherapy alone and Chemo-PRT groups, we performed PSM analysis. After PSM, we matched 4798 patients who received chemotherapy alone, ensuring comparability with the Chemo-PRT group (chi-square test P > 0.05) (Table 1). The analysis showed better survival in the Chemo-PRT group compared to the chemotherapy alone group (18 months vs 11 months, P < 0.001) (Figure 2(D)), mirroring outcomes in patients advised for but not receiving PRT.
Subgroup Analyses
Our subgroup analyses comparing patients receiving combined chemotherapy and PRT to those with chemotherapy alone showed that nearly all subgroups had a better prognosis with the combined treatment, except for those with tumors in the main bronchus, bilateral locations, of unknown size, with lung metastases, more than two extrathoracic organ metastases, or distant lymph node metastases alongside a single extrathoracic organ metastasis, where no significant benefit from PRT was observed (All P > 0.05) (Figure 3). Subgroup analysis of chemotherapy alone vs chemotherapy combined with Primary Resection Therapy (PRT) after Propensity Score Matching (PSM) in NSCLC patients with extrathoracic metastases.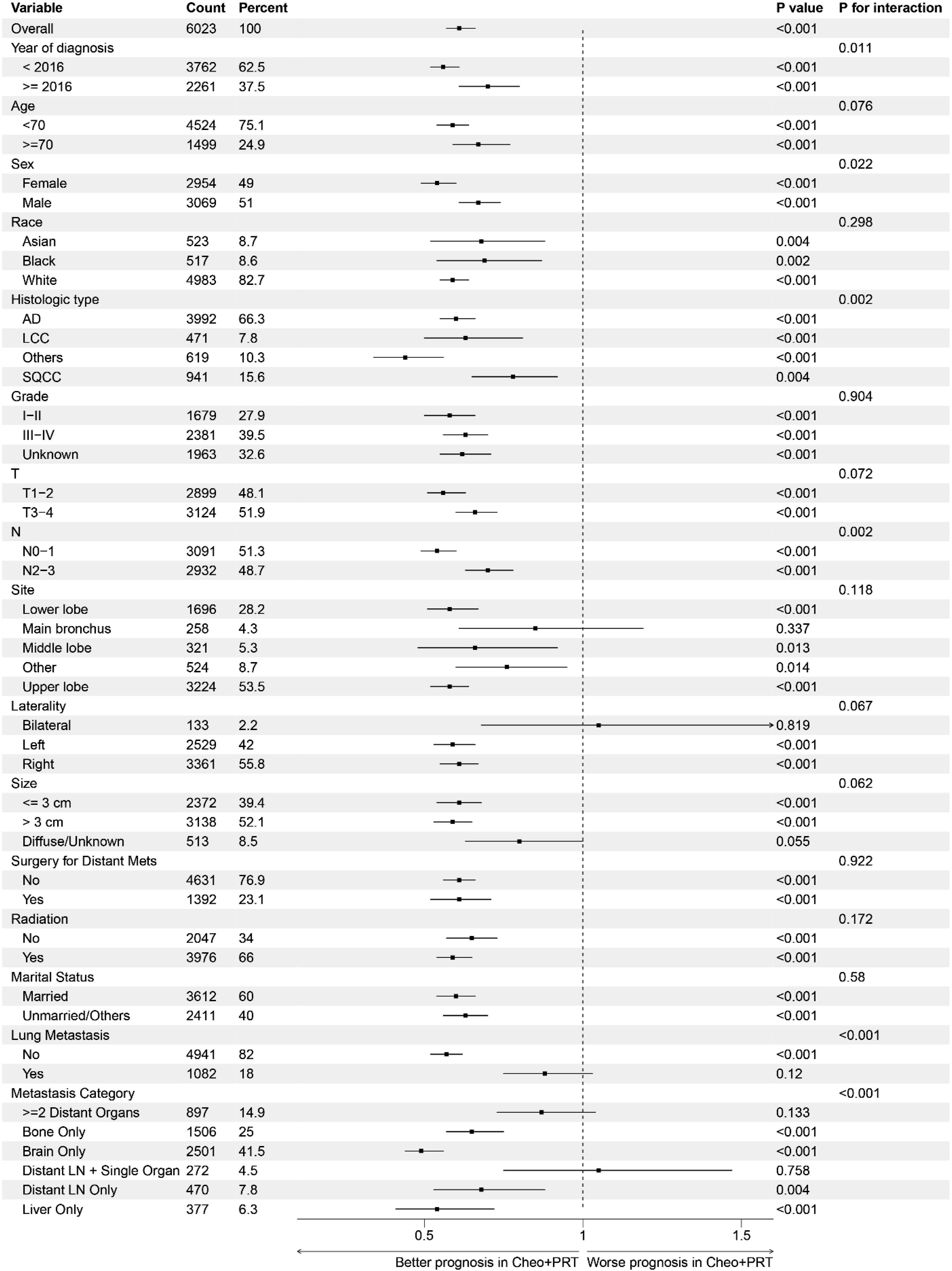
While the effectiveness of combined chemotherapy and PRT vs chemotherapy alone varied between the immunotherapy and non-immunotherapy eras, the impact was notably less pronounced in the immunotherapy era compared to the earlier period (HR 0.56 vs 0.70, P for interaction = 0.011). PRT showed greater appropriateness in patients with fewer lymph node metastases, as evidenced by a more favorable hazard ratio (N0-1 VS N2-3, HR 0.54 vs 0.70, P for interaction = 0.002). Combined PRT for single brain (HR = 0.49) metastases and liver metastases (HR = 0.54) is the best among distant metastases in oligo organs. Detailed Kaplan-Meier curves and median survival times for each subgroup are presented in Figure S1.
Prognostic Analysis in the Chemotherapy Combined PRT Group
We explored the effect of stratified preoperative administration of systemic therapy on prognosis in the subgroup with the addition of PRT, and we found that in the group with the addition of PRT, compared to chemotherapy alone, the median OS was prolonged by only 5 months if no systemic therapy was administered preoperatively (11 to 16 months , after PSM), whereas the median OS was prolonged by 30 months if systemic therapy was administered prior to the operation (11 to 30 months, after PSM) (Figure 4). After adjusting for various factors in a multifactorial Cox regression analysis, systemic therapy before was identified as an independent prognostic factor for improved outcomes (HR = 0.69, 95% CI 0.57-0.84, P < 0.001) (Table 2). Regarding surgical procedures, wedge resection is associated with a poorer prognosis compared to lobectomy (HR = 1.63, 95% CI 1.33-2.02). Additionally, patients who had three or more lymph nodes examined demonstrated a better prognosis compared to those with fewer than three lymph nodes removed (HR = 0.74, 95% CI 0.62-0.89). Patients with metastases at more than two distant sites or a combination of a single distant site and distant lymph node metastases have a significantly worse prognosis. Among those with oligometastatic extrathoracic metastases, the best prognosis is seen in patients with only distant lymph node metastases, followed by liver, brain, and then bone metastases. Key prognostic factors include age, gender, histological type, N stage, and marital status (all with P < 0.05). However, in the group receiving combined chemotherapy and PRT, neither additional radiotherapy (HR = 1.04) nor resection of distant metastases (HR = 0.97) showed a significant survival benefit. Kaplan-Meier survival curves were generated for three treatment groups in NSCLC patients with extrathoracic metastases: Chemotherapy Alone, Chemotherapy Combined with Primary Resection Therapy (PRT) without Preoperative Systemic Therapy, Chemotherapy Combined with PRT and Preoperative Systemic Therapy. Univariable and Multivariable Cox Analysis for Overall Survival (OS) in Chemotherapy + PRT Patients. PRT: Primary Resection Therapy; AD: Adenocarcinoma; SQCC: Squamous Cell Carcinoma; LCC: Large Cell Carcinoma.

Creation and Validation of a Predictive Nomogram
In the chemotherapy-alone group, since both the patients who were recommended but did not undergo PRT and the patients after PSM have a median survival time of 11 months, we categorize patients with a survival time exceeding 11 months as the PRT benefit group and those with a survival time of 11 months or less as the PRT non-benefit group. In the training set, we utilized multifactor logistic regression to identify variables that are associated with the benefit of PRT (Table S1).
We used specific variables in our analysis to identify patients with extrathoracic metastatic NSCLC who would most likely benefit from combined chemotherapy and PRT. The probability of benefit from PRT is evaluated using a nomogram (as shown in Figure 5) that calculates a total score based on these variables, with corresponding markers indicating the likelihood of benefit from the combined treatment. In the ROC curve analysis, the AUC for the training set is 0.751 and the AUC for the test set is 0.766 (Figures 6(A) and 6(B)). The calibration curve (Figures 6(C) and 6(D)) demonstrated the stability of the model’s predictive performance. We then performed prognostic stratification for the best cutoff through the ROC curve of 288.1523 points (corresponding to a probability of benefit of 62.7%). Further validation of the nomogram’s discriminative ability was conducted in the train and test sets (Figures 6(E) and 6(F)). The results indicated discrepancies in OS between the surgical benefit group and the surgical non-benefit group, as well as between the surgical benefit group and the chemotherapy-only group, in both the training and test sets. However, there were no significant differences in OS between the surgical non-benefit group and the chemotherapy-only group (Figures 6(E) and 6(F)). Using CSS as the outcome, the PRT-beneficial group demonstrated a clear survival advantage compared to both the PRT-non-beneficial group and the chemotherapy-only group, further confirming the robustness of the model in distinguishing favorable from unfavorable groups (Figure S2). PSM-based nomogram for predicting NSCLC patients with extrathoracic metastases who are best suited for chemotherapy combined with PRT. Receiver Operating Characteristic (ROC) curves with area under the curve (AUC) for the nomogram in training (A) and test sets (B). Calibration curves in training (C) and test (D) sets for nomogram accuracy. KM survival curves of OS comparing PRT-beneficial/non-beneficial and chemotherapy-alone groups in training (E) and test (F) sets.

Discussion
Recent research shows a decrease in the frequency of surgeries at the primary sites of advanced lung cancer. 14 This trend is likely due to the rising use of targeted therapies and immunotherapy, which have brought more personalized treatment plans and substantially enhanced the prognosis for advanced-stage diseases. 15 Therefore, the prognostic value of primary site resection in patients with extrathoracic metastases merits further exploration, considering its potential significance in improving outcomes for these patients.
Our analysis of extrathoracic metastases NSCLC cases from the SEER database from 2010 to 2019 indicates that, regardless of whether comparing outcomes of patients recommended for but not receiving PRT or analyzing post-PSM outcomes of the chemotherapy-alone group vs the chemotherapy combined with PRT group, the prognosis in the combined therapy group is consistently better than that in the chemotherapy-alone group. In accordance with existing literature, which suggests surgery is typically not recommended for multiple metastases but may be suitable for oligometastases,16-18 our findings support this view. We found that for patients with oligometastatic disease, PRT is most effective for certain types of metastases, with a specific hierarchy of efficacy: brain metastases show the greatest benefit from PRT, followed by liver, and then bone metastases. However, there is limited research on the effectiveness of surgery in patients with distant lymph node metastases. Our findings suggest that while surgery may not be beneficial for those with additional distant organ metastases, it could improve outcomes for patients with only distant lymph node metastases.
A wealth of research has delved into the impact of neoadjuvant and adjuvant chemotherapy in advanced, limited-stage lung cancer.19,20 Yet, the rarity of lung cancer cases involving extrathoracic metastases, coupled with the resection of primary lesions, has led to a scarcity of studies examining the optimal sequencing of systematic therapy and PRT for patients with extrathoracic metastatic NSCLC. This highlights a significant area for future investigation. Although a single-center, retrospective study with a small sample size suggested neoadjuvant chemotherapy as an independent prognostic factor in surgical treatment for stage IV primary lung cancer, 12 larger-scale validations of this effect were absent. Our research, employing a more comprehensive database, showed that patients with extrathoracic metastatic NSCLC who received preoperative systematic therapy and surgery had a significantly improved prognosis compared to those who did not. Hence, for patients with distant metastases scheduled for primary resection, the optimal approach may involve tumor control through systemic therapy before primary resection.
Furthermore, our prognostic analysis of the group undergoing surgery in conjunction with PRT revealed that lobectomy offers a more favorable prognosis compared to wedge resection. Additionally, the necessity of combined lymph node dissection in the surgical management of patients with extrathoracic metastases of NSCLC was underscored. This is consistent with the findings of previous studies. 21 However, the NCCN recommends the possibility of primary plus chemotherapy plus metastasectomy for appropriate patients with oligometastases, 22 but interestingly, our study did not find a survival benefit from additional metastatic control such as radiotherapy or metastasectomy in patients treated with chemotherapy in combination with PRT. This may be due to the SEER database’s lack of details on the type, dose, and target sites of radiation therapy, underscoring the need for further research and exploration into this aspect.
Only one previous study was found to develop a predictive model for primary resection in stage IV lung cancer; however, because this study did not include specific metastatic site and treatment information, the performance of the model was very limited, with AUCs of only 0.62 and 0.6 for the training and test sets, respectively. 23 We uniquely incorporated factors such as the locations of metastases at diagnosis, whether patients underwent systemic therapy prior to surgery, along with other critical clinical variables, to develop a nomogram. This model demonstrated superior predictive performance, achieving an AUC of 0.751 in the training set and 0.766 in the test set. This chart demonstrated good performance and offers a effective recommendation for clinical screening of extrathoracic metastatic NSCLC patients potentially suited for chemotherapy combined with PRT.
Our study has limitations inherent to its database-based, retrospective design, including the absence of specific treatment regimen details. Although SEER records whether radiation therapy was administered, it does not provide information on aspects such as type, dosage, or targeted locations. Similarly, details on chemotherapy protocols, including specific drugs, dosages, and cycles, are not fully available. More granular data in future studies would enable a deeper investigation into these treatment effects. Another limitation is the SEER database’s lack of specific data on certain metastatic sites, particularly adrenal metastasis, which plays a key role in understanding metastatic disease progression and prognosis. 24 These limitations highlight the need for more prospective studies to validate our findings.
Conclusion
This study demonstrates that in both pre- and post-immunotherapy eras, patients with extrathoracic metastatic NSCLC benefit significantly from adding primary tumor resection to chemotherapy, especially after preoperative systemic therapy. We developed a nomogram to accurately identify the best candidates for PRT among these patients, enhancing personalized treatment strategies and improving survival outcomes.
Supplemental Material
Supplemental Material - Exploring the Role of Preoperative Systemic Therapy and Primary Resection in NSCLC With Extrathoracic Metastases: Identifying the Optimal Candidates
Supplemental Material for Exploring the Role of Preoperative Systemic Therapy and Primary Resection in NSCLC With Extrathoracic Metastases: Identifying the Optimal Candidates by Xuanhong Jin, Xinyu Zhu, Hangchen Shen, Chongya Zhai, Hongming Pan and Liangkun You in Cancer Control
Footnotes
Acknowledgments
We extend our gratitude to the entire SEER database team for their dedication in data gathering, upkeep, dissemination, and related efforts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.