
Abstract
Background
Because of multiple competing death outcomes and time-varying coefficients, using a Cox regression model to analyze the prognostic factors of low-grade gliomas (LGG) may lead to a possible bias. Therefore, we adopted time-dependent competing risk models to obtain accurate prognostic factors for LGG.
Methods
In this retrospective cohort study, data were extracted from patients enrolled in the Surveillance, Epidemiology, and End Results (SEER) database between 2000 and 2018. Univariate analysis was performed using the cumulative incidence function (CIF) and Kaplan-Meier (KM) function. Time-dependent competing risk and Cox regression models were used in the multivariable analysis.
Results
A total of 2581 patients were diagnosed with low-grade glioma, among whom 889 died from low-grade glioma, 114 died from other causes, and the rest were alive. The time-dependent competing risk models indicated that age, sex, marital status, primary tumor site, histological type, tumor diameter, surgery, and year of diagnosis were significantly associated with low-grade glioma-specific death, and the relative effect of age, tumor diameter, surgery, oligodendroglioma, and mixed glioma on low-grade glioma-specific death changed over time. Compared with the competing risk models, the Cox regression model misestimated the hazard ratio (HR) of covariates on the outcome and even produced false-negative results.
Conclusions
The time-dependent competing risk models were better than the Cox regression model for evaluating the impact of covariates on low-grade glioma-specific mortality in the presence of competing risks and time-varying coefficients. The models identified the prognostic factors of LGG more accurately than the Cox regression model.
Keywords
Introduction
Gliomas, which are malignant tumors originating from brain glial cells, account for approximately 80.8% of primary malignant tumors of the brain and other central nervous systems (CNS).1,2 According to the World Health Organization classification, gliomas can be classified as grades I–IV based on histological features. Grade I and II gliomas, which are defined as low-grade gliomas (LGGs), mainly include astrocytoma, oligodendroglioma, and oligoastrocytoma (mixed glioma) 3 and occur primarily in the supratentorial brain regions; the frontal lobe is the most common site. 4 The most common clinical symptom of patients with LGG is epileptic seizures, although some patients have headaches, personality changes, visual field defects, etc.5,6 Although LGGs are noted for their slow growth and low proliferation capacity, there is a risk of recurrence and progression to high-grade malignancy. Accordingly, surgical resection within the maximum safety range is the first and most important consideration in patients with LGG. Patients at high risk of recurrence or deterioration may require radiotherapy or chemotherapy. 7 However, the regimens and timing of radiotherapy and chemotherapy are still controversial. In such cases, appropriate personalized therapeutic plans require accurate survival and prognosis analyses.
Patients with LGGs can experience LGG-specific death (LSD) or other causes of death (OCD; eg, acute stroke, accidents). Generally, LSD is not observed when patients die of other causes because OCD can affect or hinder the occurrence of LSD. Other causes of death and LSD are mutually exclusive, and there are competing risks between them. Kaplan-Meier (KM) analysis and the Cox regression model are widely used to analyze the effect of variables on the outcome of interest, but they assume that the endpoint is constituted only by the outcome of interest and regard other competing outcomes as censored, resulting in a misestimation of cumulative mortality. Unlike traditional survival analysis methods, the cumulative incidence function (CIF) and competing risk models support the existence of multiple endpoints and consider the competing risks among them, resulting in greater accuracy when identifying prognostic factors.8,9
In addition, Cox proportional hazards (PH) and competing risk models are established under the condition of PH assumption; that is, the hazard ratio (HR) for covariates is fixed and does not change over time. Ignoring this condition leads to time-dependent bias. 10 However, time-varying effects of covariates are very common, and it is necessary to consider time-dependent models, such as time-varying coefficient or stratified models. 11
Therefore, in our study, time-dependent competing risk models were adopted to obtain accurate prognostic factors. The models were compared with a time-dependent Cox regression model to assess the bias in the Cox regression analysis.
Materials and Methods
Data Source
The Surveillance, Epidemiology, and End Results (SEER) database is a large, publicly available database supported by the National Cancer Institute (NCI). The SEER database covers representative geographic areas and races from 18 U.S. registries and approximately 27.8% of the U.S. population.12,13 Therefore, it provides a tremendous amount of reliable information for cancer research. Surveillance, Epidemiology, and End Result statistical software version 8.3.9 (cancer.gov/seerstat, National Cancer Institute) was used for data extraction and statistical analysis. We selected the SEER research data of patients diagnosed with cancer between 2000 and 2018 and submitted in November 2020.
The SEER database is publicly available and identifiable information is hidden. Therefore, additional ethical approval was not required.
Patient Selection
This was a retrospective cohort study. Following the International Classification of Diseases for Oncology, third Edition, we searched all glioma cases obtained from the SEER database with histology codes 9380/3-9384/3 or 9391/3-9480/3 and anatomical codes C71.0–C71.9. We extracted patient records, including demographic characteristics, tumor grade, primary tumor site, histological type, largest tumor diameter, treatment status, year of diagnosis, diagnostic information, first malignant primary indicator, outcome, and survival time. The exclusion criteria were as follows: (1) grade III or IV glioma; (2) age <20 years; (3) not confirmed by microscopic examination; (4) additional primary tumors; and (5) unknown variables. The final variables included age, sex, race, marital status, primary tumor site, histological type, tumor diameter, surgery, and year of diagnosis. Information on radiation and chemotherapy was not collected because of incomplete data. Outcomes were divided into censored outcomes, LSD (deaths attributed to LGG), and OCD. OCD (ie, competing events) was defined as death attributed to causes other than LGG. The patient selection process is shown in Figure 1. Flowchart of patient inclusion and exclusion.
Processing of Variables
X-tile software is a bioinformatics tool that can be used for outcome-based cutoff optimization.
14
Our study used X-tile to determine the optimal cutoff point for age and tumor diameter. According to the calculations of the X-tile program, we used 3 age groups (≤47 years, 48-62 years, and ≥63 years) and 3 tumor diameter groups (≤3.7 cm, 3.8-5.9 cm, and ≥6.0 cm) (Figure 2). The optimal cutoff points of age and tumor diameter are calculated using the X-tile procedure. The optimal cutoff value of age is represented by the histogram (A) and Kaplan–Meier plots (C) of the whole cohort. The optimal cutoff value of the tumor diameter is represented by histograms (B) and Kaplan–Meier plots (D) of the whole cohort.
Statistical Analysis
Univariate analysis
For data with only a single outcome, the KM survival analysis can be used to estimate the cumulative incidence of an outcome event. The function
Unlike the KM analysis, the CIF can accurately estimate the cumulative incidence of an event of interest in the presence of competing risks. The function
Multivariable analysis
In the absence of competing risks, the hazard function is written as
In the presence of competing risks, 2 competing risk models can be considered: a cause-specific (CS) hazard model and a subdistribution (SD) hazard model, which have different meanings. If there is data for the event of interest (event 1) and competing event (event 2), the CS model is defined as
The PH assumption test should be satisfied for the PH models described above. In this study, univariate analysis was performed using the CIF and KM functions. Then the variables with statistical significance in the univariate analysis were added to the competing risk and Cox regression models, and the year of diagnosis as a continuous variable was entered directly into the multivariable analysis. Interactions between time and covariates were introduced to test the PH assumption of the models. When the PH assumption of covariates was not satisfied, the interactions between time and corresponding covariates will be introduced to construct time-dependent models.
16
The formula of the time-dependent fitting model applicable to the these 3 models is
The data were analyzed using SAS (Version 9.4), and R (version 4.1.1) statistical software. Differences were considered statistically significant when the analysis found a probability value of P < .05.
Results
Patient Characteristics
Baseline Characteristics of Patients With LGG.

Abbreviations: SDW, separated/divorced/widowed; LGG, low-grade glioma.
Univariate Analysis
A total of 889 patients died from LGG and 114 died from other causes. The CIF showed that age, sex, marital status, primary tumor site, histological type, tumor diameter, and surgery were significantly associated with LSD, whereas race was not significantly associated with LSD. The cumulative incidence curves of LSD are shown in Figure 3. In addition, the KM analysis of the corresponding covariates had higher cumulative incidences at 60 months than the CIF. Older age was associated with a higher cumulative incidence of OCD. Additional details are provided in Table 2. Cumulative incidence curves of low-grade glioma-specific death by (A) age, (B) sex, (C) marital status, (D) primary tumor site, (E) histological type, (F) largest tumor diameter, (G) surgery. Univariate Analysis of Prognostic Factors in Patients With LGG. Abbreviations: LGG, low-grade glioma; LSD, low-grade glioma-specific death; OCD, other causes of death; KM, Kaplan-Meier; CIF, cumulative incidence function.

Multivariable Analysis
Time-Dependent Cox Regression, SD, and CS Models For LSD.
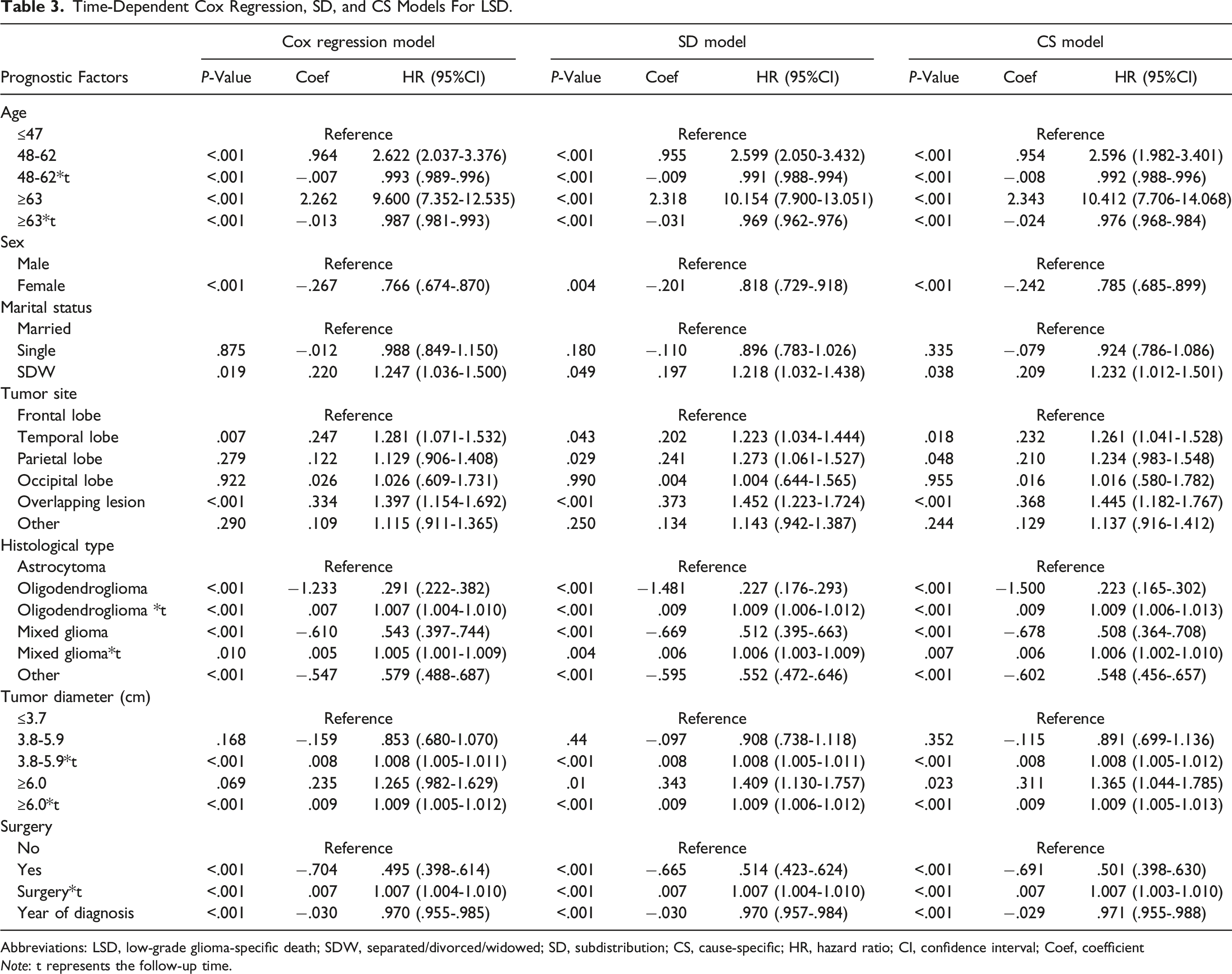
Abbreviations: LSD, low-grade glioma-specific death; SDW, separated/divorced/widowed; SD, subdistribution; CS, cause-specific; HR, hazard ratio; CI, confidence interval; Coef, coefficient
Note: t represents the follow-up time.
The SD and CS models showed that patients with older age, male sex, separated/divorced/widowed (SDW) status, tumors located in the temporal/parietal/overlapping lobes, astrocytoma, larger tumor diameter, no surgery, and earlier year of diagnosis had a higher relative incidence and cause-specific hazard of LSD. In addition, The HR of age in LSD decreased with time, whereas the HRs of surgery, tumor diameter, oligodendroglioma, and mixed glioma in LSD increased with time.
The HRs and time-varying effects of covariates in the Cox regression model were higher or lower than those of covariates in the competing risk models, and the Cox regression model showed negative results for tumors in the parietal lobe.
Time-Dependent SD and CS Models for OCD.

Abbreviations: OCD, other causes of death; SD, subdistribution; CS, cause-specific; HR, hazard ratio; CI, confidence interval; Coef, coefficient.
Discussion
The Cox PHs model has been widely used in clinical research. However, if the covariates violate the PH assumption or there are multiple endpoints in the data, using the Cox PHs model may result in incorrect results. In our study, by analyzing the prognostic factors of LSD using a large sample with multiple endpoints and time-varying coefficients, we found that traditional Cox regression analysis showed a certain bias in the coefficients and HR values of covariables and even had false-negative results compared with time-dependent competing risks models.
Two competing risk models should be established in the presence of competing events. These models explain the process from etiology to the absolute incidence of the event, respectively. The impact of variables on the relative incidence of events of interest can be interpreted by considering cause-specific hazards of events of interest and competing events.8,18 For example, the impact of variables on the increase in the cumulative incidence of LSD was led by an increase in the cause-specific hazard of LSD or the indirect effect of a significant decrease in the cause-specific hazard of OCD. Therefore, treatment strategies should be carefully determined taking into account the indirect effects of competing events that can lead to a lower or higher incidence of events of interest. In our study, the effect of prognostic factors on the cumulative incidence and cause-specific risk of LSD were statistically significant and in the same direction. Therefore, the effect of prognostic factors on LSD can be interpreted as actual effects rather than indirect effects of competing events.
Older patients with LGG were more likely to have neurological deficits, larger tumors, and more aggressive expansion than younger patients, leading to a poor prognosis.19,20 However, our study found that the effect of older patients on the relative incidence and cause-specific hazard of LSD decreased over time. We believe that this may be due to the risk of young age on LSD increasing over time. In addition, age also was a strong risk factor of OCD, which may indirectly lead to a lower relative incidence of LSD in older patients than the actual risk. The Cox regression model that ignores competing events underestimates the relative change of age over time and gradually overestimates the impact of older patients on LSD.
Previous studies have shown that methylation of the O-6-methylguanine-DNA methyltransferase promoter is more likely to occur in women and often leads to better survival outcomes.21,22 Our study confirmed that women had a lower risk of LSD than men. Specifically, the relative incidence and cause-specific hazard of LSD for women was decreased by 18.2% in the SD models, 21.5% in the CS model, and 23.4% in the Cox regression model. Therefore, the Cox regression model overestimates the effect of this covariate.
Compared with married patients, the relative incidence and cause-specific hazard of LSD among SDW patients increased by 21.8% in the SD model and 23.2% in the CS model; the Cox regression model overestimated this risk. Separated/divorced/widowed patients experience greater stress and are more likely than married patients to suffer from depression or other psychological disease.23,24 Psychological disease can lead to neuroendocrine and immune system disorders, which cause the release of glucocorticoids, inhibit the expression of major histocompatibility complex class-I and class-II molecules, and reduce natural-killer cells activity, and ultimately accelerating tumor progression and increasing LGG-specific mortality.25,26
In our study, the SD and CS models showed that patients with LGG in the temporal/parietal/overlapping lobes had worse prognosis than those with LGG in the frontal lobe. Surprisingly, tumors in the parietal lobe gave a false-negative result in the Cox regression model. We speculate that competing risks caused this bias. Authoritative statistical reports indicate that patients with tumors in the parietal lobe have lower 5-year survival than patients with tumors elsewhere in the brain and CNS, 2 which, to some extent, supports the results of the competing risk models. Previous studies have also indicated that patients with mutated isocitrate dehydrogenase (IDH) have longer survival times than those with wild-type IDH. Frontal lobe tumors are more likely to have mutated IDH, whereas temporal and parietal lobe tumors are more likely to have wild-type IDH,27,28 which could explain why temporal and parietal lobe tumors are associated with a worse prognosis than frontal lobe tumors. In addition, patients with LGG in overlapping regions had shorter survival times than those with LGG originating in a single lobe, which may be because they are more likely to have complex functional deficits and surgical resection is more difficult.
We found that patients with larger tumor diameters had a worse prognosis over time, especially those with tumor diameters ≥6 cm at diagnosis. We believe that a large tumor diameter increases the difficulty of complete surgical resection, thereby increasing the risk of recurrence and deterioration. 29
In the SD model, patients with astrocytoma had the worst prognosis, which can be explained by genetic alteration of the chromosome arms 1p and 19q in gliomas. As LGGs with 1p/19q codeletion are sensitive to radiotherapy and chemotherapy, they are less likely to transform into higher-grade tumors, thus conveying a better prognosis and a greater chance of survival. 1p/19q codeletion is a typical genetic feature of oligodendrogliomas and is also found in most oligoastrocytomas but it is rarely seen in astrocytomas, 30 which could be why astrocytomas have a poorer prognosis. However, the protective effects of oligodendrogliomas and mixed gliomas against LSD are not constant. The relative incidence and cause-specific hazard of LSD among patients with oligodendrogliomas and mixed gliomas increases over time.
The models in our study confirmed the protective effects of surgery. However, the protective effect of the surgery gradually decreased over time, which may be due to tumor growth and recurrence. There is increasing evidence that total surgical resection and early surgery are beneficial to the prognosis of patients with LGG, whereas subtotal surgical resection and late surgery result in a high risk of recurrence and deterioration. Therefore, LGGs should be surgically resected within the maximum safety range as early as possible, as early surgery improves overall survival and progression-free survival and reduces the incidence of recurrence and malignant transformation.31,32
Our study showed that the relative incidence and cause-specific hazard of LSD decreased as the year of diagnosis neared the present, and related studies have suggested that this is largely due to improved treatment. 33 According to the European EORTC22844 and American RTOG9802 standards, LGGs can be divided into low-risk and high-risk groups based on prognostic predictors.34,35 Patients in the high-risk group are recommended early radiotherapy and/or chemotherapy. 36 The RTOG0424 clinical trial, which included 129 patients with high-risk LGG, confirmed that chemotherapy combined with radiation therapy was more beneficial for survival than radiation therapy alone. In addition, patients with 1p/19q intact or IDH1-R132H wild-type often have a poor prognosis and are recommended are recommended postoperative adjuvant therapy. 37 Therefore, further exploration of prognostic factors is conducive to the continuous improvement of treatment options.
The advantages of our study are as follows. First, we analyzed the prognosis of LGGs using time-dependent competing risk models, thus correcting for the bias caused by the traditional Cox regression model and explaining the time-varying effects of the variables. Second, X-tile was used to scientifically intercept the optimal grouping nodes of age and tumor diameter. Finally, our data were obtained from the SEER database, which includes a large amount of cancer data and is supported by the NCI, a factor that adds to the high reliability of our study.
However, our study had some limitations. First, because more detailed information, such as complete radiation and chemotherapy information, presurgical neurologic deficit, and genotyping, was unavailable, we could not perform a more detailed analysis of risk grouping and treatment effect. In addition, cause of death classification may be misattributed, leading to overestimation or underestimation of the outcome of interest. Second, our study was retrospectively designed, resulting in inevitable selection bias. However, to the best of our knowledge, our study is the first to adopt time-dependent competing risk models to identify prognostic factors of LGG; therefore, it possesses an important reference value. In addition, competing risks and the violation of the PH assumption test are common problems in the survival data, and our study provides a very useful research method to address those problems.
Conclusion
This study took advantage of time-dependent competing risk models to accurately identify prognostic factors for adult patients with LGG in the SEER database. We found that older age, male sex, SDW status, tumors in the temporal/parietal/overlapping lobes, astrocytoma, larger tumor diameter, no surgery, and earlier year of diagnosis were associated with poor prognosis for LGG patients. The protective effect of young age, surgery, oligodendrogliomas, and mixed glioma on LSD will gradually decline over time, and the deleterious effect of tumor diameter will gradually increase.
Footnotes
Author Contributions
KC, DH, JL, AX designed this study. DD, MK, MP participate in data selection and collation. KC, DH, DD, MK, MP are involved in statistical analysis and drawing tables and figures. KC, DH performed data analysis and manuscript drafting. JL, AX critically revised the manuscript. All authors reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data in this study are from SEER database. These data can be freely available through the website of SEER database (https://seer.cancer.gov/).
Ethical Approval Statement
This study does not require ethical approval because SEER is a public database, and personally identifiable information has been hidden.