
Abstract
Background
Multimorbidity is common in patients with breast cancer, thus increasing the complexity of cancer care and economic burden, worsening their prognosis and quality of life. The prevalence of multimorbidity and its influence on psychological distress among patients with breast cancer have not been well characterized.
Objectives
To examine the prevalence of multimorbidity and its associations with anxiety and depression among newly diagnosed patients with breast cancer.
Methods
We conducted a retrospective observational cohort study using a large administrative claims database. Patients with breast cancer (ICD-10-CM: C50.x) were identified during the study period (1/1/2017-12/31/2020). The index date was defined as the diagnosis date of breast cancer. Demographics and comorbid conditions were assessed using data within 12 months prior to the index date. Multimorbidity was defined as the presence of ≥2 comorbid conditions. Anxiety and depression were examined using data within 12 months after the index date. Multivariable logistic regressions were performed to examine the associations between multimorbidity and anxiety and depression, adjusting for sociodemographic factors.
Results
Of the 6392 patients with newly diagnosed breast cancer, 86.9% had multimorbidity at the time of breast cancer diagnosis. The median number of comorbid conditions was 5. Overall, 27.7% experienced anxiety, and 21.9% experienced depression in the first year following breast cancer diagnosis. An increased number of comorbid conditions was associated with elevated prevalence of both anxiety and depression. After adjusting for possible confounding factors, number of comorbid conditions was significantly associated with risk of anxiety (adjusted odds ratio [95% confidence interval (CI)]: 1.17 [1.15-1.19]), and depression (1.24 [1.21-1.26]); all P < .0001.
Conclusions
Multimorbidity was highly prevalent among patients with breast cancer and was strongly associated with increased risk of anxiety and depression in the first year following breast cancer diagnosis. The presence of multimorbidity, anxiety, and depression should be considered in the context of clinical decision making to optimize cancer care and improve mental health and quality of life.
Keywords
Introduction
Breast cancer is the most common cancer among women in the United States (US), except for skin cancers. 1 It represents nearly a third of all new female cancer diagnoses each year (about 255 000 cases) and is the second leading cause of cancer deaths (after lung cancer) among women overall (about 42 000 women die from breast cancer each year).1,2 Due to early detection, accurate diagnosis, and advances in treatment and supportive care, an increasing number of patients with breast cancer are given a good prognosis.3,4 Today, in the US and Canada, the 5-year net survival for breast cancer approaches 90% (2, 8).2,5 The average 10-year survival rate in the US for women with non-metastatic invasive breast cancer is 84%. 2 As the number of breast cancer survivors increases, understanding and addressing the physical and mental health needs of this growing population and emphasizing the improvement of mental health and overall quality of life (QOL) is becoming increasingly important.6,7
The incidence of breast cancer increases with age and so does the prevalence of comorbidities.8,9 Cardiovascular diseases, obesity, diabetes, osteoporosis, metabolic disorders, and psychiatric disorders are commonly comorbid with breast cancer.4,8,10,11 Multimorbidity, the co-occurrence of two or more chronic conditions, is common in patients with cancer.12,13 Between 69-91% of this population had at least one comorbid disease,14,15 and 23% of the population had five or more comorbid conditions. 14 Breast cancer survivors tend to report more comorbid conditions and greater multimorbidity compared with survivors of other cancers. 16 One study claims that 32.9% of women with breast cancer experiencing one and 30.1% experiencing two or more comorbid conditions, 17 whereas a study conducted by Wu et al in 2014 found ∼84% of the participants had 1 or more comorbid conditions. 18
In addition to multimorbidity, psychological distress (eg, anxiety, depression) is a significant problem that can affect over half of those who have been diagnosed with cancer. 6 Cancer patients are about twice as likely to take medication for anxiety (16.8% vs 8.6%) and depression (14.1% vs 7.8%) as patients without cancer. 19 Hawkins et al estimated that 2.5 million cancer survivors were taking medication for anxiety or depression in the US in 2010-2013. 19 Carreira et al found that women with breast cancer had 1.3 times higher risk of anxiety and depression compared with matched women without cancer, the relative risks decreased over time but remained elevated for several years after breast cancer diagnosis. 20 Gaining a better understanding of the relationship between multimorbidity and psychological distress in breast cancer may assist with the prognosis assessment and disease management to improve outcomes and QOL.
No gold standard exists to measure multimorbidity in cancer populations.21,22 Many studies have reported that comorbidity and multimorbidity at the time of cancer diagnosis, and measured by the Charlson Comorbidity Index (CCI),10,23,24 or simple count of some strictly selected comorbid conditions and their relationships with psychological distress among breast cancer patients.4,8,10,17,23,25-29 However, the influence of individual comorbid conditions on mental health may vary, the CCI includes only 19 chronic physical conditions (without psychiatric conditions) and it has been validated to predict mortality, but maybe not associated with poor mental health. 10 Few studies to date have investigated multimorbidity including broad chronic conditions and their associations with breast cancer outcomes.8,10,23,26-30 Some studies have been limited to older populations (ie, ages ≥60, ≥65, or ≥70 years),10,15,31 cancer registry-based studies,4,17,23 or survey studies without detail data on comprehensive comorbidities.11,25,26,29,31 Very limited data are available on the associations of the presence of multimorbidity with mental health.17,18 The objectives of the current study were to quantify the prevalence of specific comorbid conditions and multimorbidity among patients with newly diagnosed breast cancer and examine the associations between multimorbidity and anxiety and depression using a large US administrative healthcare claims database.
Methods
Study Design and Data Source
This is a retrospective observational cohort study of newly diagnosed patients with breast cancer using Aetna’s administrative claims data from January 01, 2017, to December 31, 2020 (study period). The claims database included over 20 million medical insurance beneficiaries, and contained patient demographics (gender, age, geographic region, and residential area), enrollment, as well as inpatient and outpatient medical and pharmacy claims for fully insured commercial health plan and Medicare Advantage members. 32 All data handling complied with federal and state requirements; the privacy and security of identifiable personal health information, required by Health Insurance Portability and Accountability Act (HIPAA) Standards, were preserved. As this retrospective observational study did not require direct patient identification, a Limited Data Set defined by HIPAA was used. The study received Waiver of Informed Consent and protocol approval from the Sterling institutional review board on April 1, 2021 (IRB ID#: 8823-HCoetzer). The reporting of this study conforms to the STROBE guidelines for observational cohort study. 33
Study Population
Patients with breast cancer were identified between January 1, 2018, and December 31, 2019 (index period). A patient was considered to have breast cancer if she met at least one of the following criteria: (1) One hospitalization with a diagnosis of breast cancer (International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis codes: C50.x) in the first diagnostic position (primary diagnosis); (2) One hospitalization with a Z-code indicating surgery (Z42.1, Z90.1, or the Current Procedural Terminology (CPT) codes: 19301-19307), radiotherapy (Z51.0), chemotherapy (Z51.11) or immunotherapy treatment (Z51.12) in the first diagnostic position; AND one claim with a diagnosis of breast cancer (C50.x) in the second diagnostic position; or (3) Three or more outpatient medical encounters, occurring within a 90-day period, with one claim with a diagnoses of breast cancer (C50.x) in the first or second diagnostic position. 34 The index date is defined as the first claim date of evidence of breast cancer within the index period. Patients with breast cancer were eligible for inclusion in the study if they had a fully insured commercial health plan or Medicare Advantage coverage with medical and pharmacy health insurance benefits for at least 12 months prior to the index date (baseline period) and 12 months after the index date (follow-up period). Patients with any evidence of breast cancer during the baseline period, age <18 years, male, or enrolled in the end-of-life care program or hospice care anytime in the study period were excluded.
Baseline Sociodemographic Characteristics
The patient sociodemographic characteristics evaluated included age at index date, US geographic region (Midwest, Northeast, South, and West), rural, suburban, or urban residence, and median household income. Household income was estimated by merging 2010 US census data to the claims data using zip-code.
Multimorbidity
Multimorbidity was defined as the presence of ≥2 comorbid conditions within a patient.12,13 The number of comorbid conditions was a count of all comorbid conditions in each patient. Forty-five most common chronic conditions including physical and mental health conditions in Aetna administrative claims data were assessed in this study. 32 These conditions and their corresponding ICD-10-CM codes were presented in Supplementary Table 1. Presence of comorbid conditions were assessed using all available data within 12 months prior to and including the index date. This long period time before breast cancer diagnosis allows for substantial time to identify diagnoses representing comorbid conditions at breast cancer diagnosis. We also defined and grouped individuals by multimorbidity level as defined by the presence of one, two, three, four, up to twelve, or thirteen or more conditions, as compared to breast cancer only. All these conditions were defined using previously described methods based on ICD-10-CM codes. 32 The Charlson comorbidity index (CCI), a validated algorithm that summarizes comorbidity burden and predicts risks of mortality and high healthcare resource utilization was also calculated (excluded breast cancer: C50.x).35,36
Outcomes
The outcomes of interest in this study included the prevalence of multimorbidity among newly diagnosed patients with breast cancer and its associations with anxiety and depression during the first year following breast cancer diagnosis. Anxiety (F40.x, F41.x) and depression (F32.x, F33.x) were identified using ICD-10-CM codes at any diagnostic positions in the claims data during the follow-up period.
Statistical Analysis
Continuous and categorical data were expressed as means (± standard deviation [SD]) or median (interquartile range [IQR]) and relative frequencies (%), respectively. Statistical significance was assessed with the Student’s t-test, or Wilcoxon rank-sum test for continuous variables, and chi-square tests for categorical variables. The means and 95% confidence intervals (CI) of the prevalence of anxiety and depression were used to compare the differences among breast cancer patients with different number of comorbid conditions. To evaluate the association of anxiety and depression with the number of comorbid conditions, multivariable logistic regression models were created to calculate adjusted odds ratios (AOR) with corresponding 95% CI. We checked model assumptions for all analyses. All P-values were two-sided, with P < .05 considered statistically significant. All data management and statistical analyses were conducted using SAS version 9.4 statistical software (SAS Institute Inc., Cary, NC).
Results
Among the 6392 patients with newly diagnosed breast cancer in the study (Supplementary Figure 1), ages 18-101 years, median age was 69 years with 68.7% over the age of 65, 39.4% were in the southern U.S., and 40.2% lived in rural areas. Patients with Medicare Advantage health plan made up 68.9% of the study population; the remaining 31.1% were commercially insured patients (Supplementary Table 2).
Prevalence of Multimorbidity
Among the 45 comorbid chronic conditions, the number of comorbid conditions ranged from 0 to 21; median (IQR) values were 5 (3, 8) for overall, 3 (1, 5) for age <65 years patients and 6 (4, 8) for age ≥65 group. Of 6392 newly diagnosed patients with breast cancer, only 6% had none of the specified comorbid conditions, 7% had only one comorbid condition, 9.4% had two comorbid conditions, and 10.6% had three comorbid conditions; 10.8%, 11.1%, 9.7%, and 9.2% had 4, 5, 6, and 7 comorbid conditions, respectively. Over 26% of the breast cancer patients had ≥8 comorbid conditions.
Figure 1 lists the top 27 most common chronic conditions among newly diagnosed patients with breast cancer by age group. The top 5 most common comorbid conditions were pain disorders (63.7%), hypertension (62.2%), hyperlipidemia (60.9%), obesity (30.7), and osteoarthritis (29.1). Compared with breast cancer patients age <65 years, age ≥65 patients had significantly higher prevalence of 24 comorbid conditions of all the top 27 most common chronic conditions except anxiety, rheumatoid arthritis/collagen vascular disease, and liver disease (Supplementary Table 3). The prevalence of most of top 27 most common chronic conditions were higher among breast cancer patients with anxiety and depression than those without anxiety and depression after breast cancer diagnosis, but the prevalence of chronic thyroid disorders, diabetes mellitus, osteoporosis, glaucoma, peripheral vascular disease, atrial fibrillation, congestive heart failure, and Iron deficiency anemia were not significantly different between breast cancer patients with and without anxiety and depression (Supplementary Table 4). Most common comorbid conditions among newly diagnosed patients with breast cancer by age group.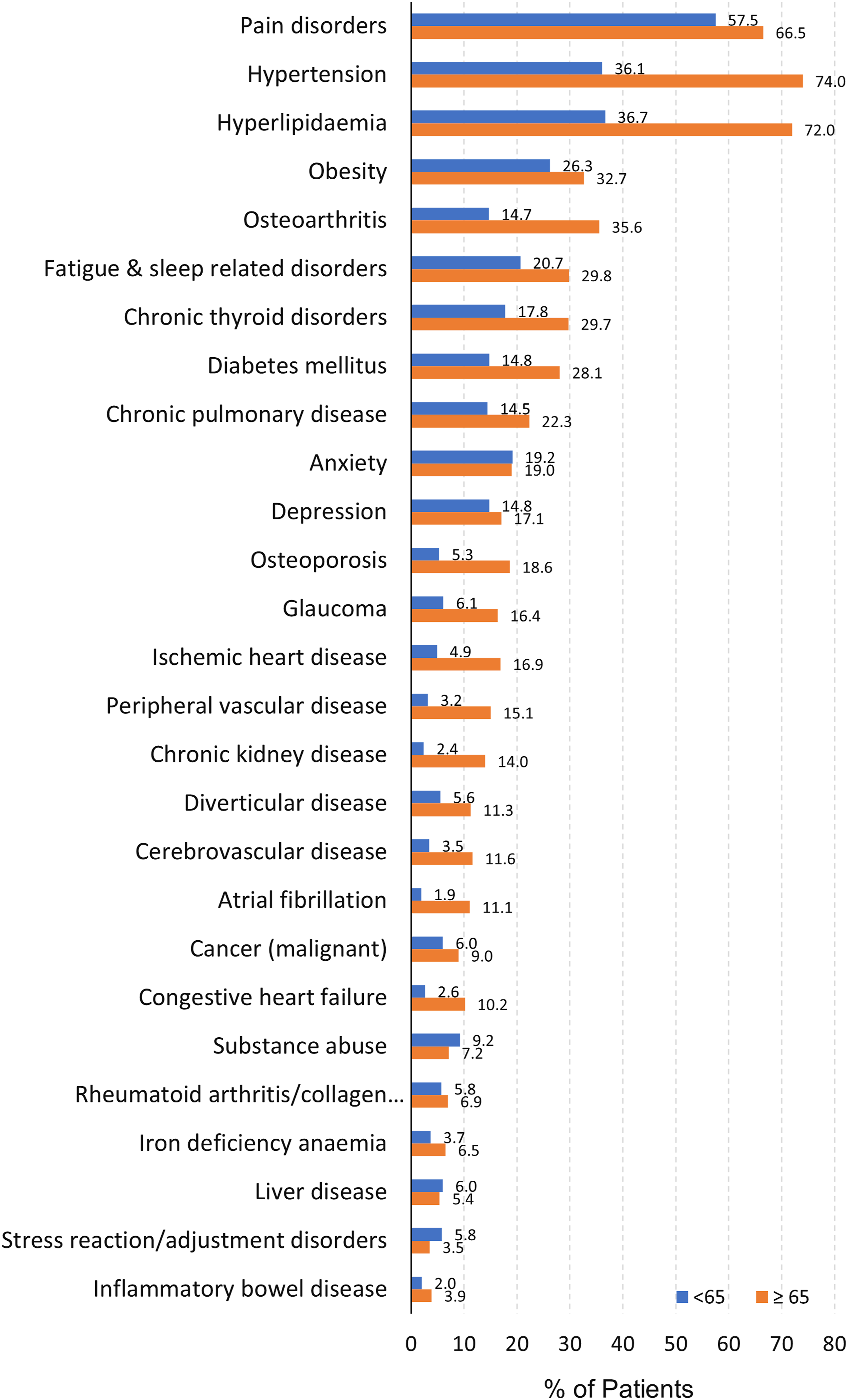
Overall, the proportion of multimorbidity among patients with breast cancer was 86.9%. The proportions of multimorbidity were higher in patients age ≥65 years than in the age <65 years group (93.9% vs 71.6%, P < .0001). Number of comorbid conditions and summed proportions of multimorbidity distribution among newly diagnosed patients with breast cancer by age group are shown in Figure 2. Most common was five comorbid conditions in patients age ≥65 years (14.9%), followed by three comorbid conditions in patients age <65 years (13.9%), shown in Figure 2(A). Age ≥65 years group had significantly higher summed proportions of multimorbidity with more than one comorbid condition (all P < .0001), Figure 2(B). Proportion of breast cancer patients with the indicated number of comorbid conditions (A). Summed proportions of multimorbidity with the indicated number of comorbid conditions (B). Proportion of breast cancer patients with the indicated number of comorbid conditions by age group (C). Summed proportions of multimorbidity with the indicated number of comorbid conditions by age group (D).
Prevalence of Anxiety and Depression
Of these newly diagnosed patients with breast cancer, 27.7% suffered anxiety, 21.9% suffered depression during the 1st-year post-diagnosis of breast cancer. The prevalence of anxiety (29.1%) and depression (23.9%) were significantly greater among the breast cancer patients with multimorbidity compared with the prevalence of anxiety (18.4%) and depression (8.9%) among those without multimorbidity (both P < .0001). The prevalence of anxiety and depression by sociodemographic characteristics and specific comorbid conditions were presented in Table 2.
Associations of Multimorbidity With Anxiety and Depression
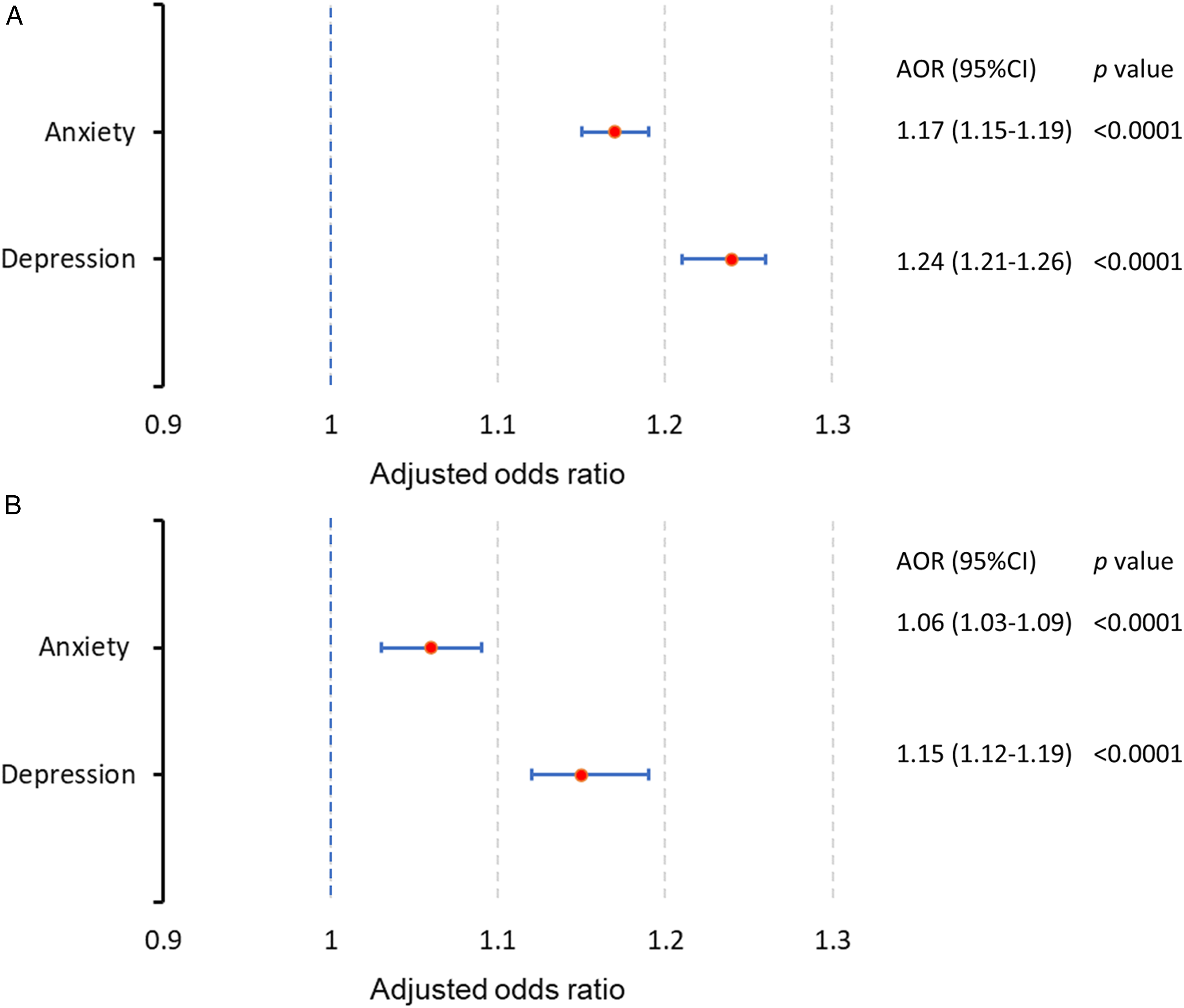
The prevalence and 95% CIs of anxiety and depression were used to compare the differences among breast cancer patients with different numbers of comorbid conditions. Although there were some fluctuations, the trend of the prevalence of both anxiety and depression were increased with increased numbers of comorbid conditions for patients with breast cancer (Figure 3A). The same patterns were found in both breast cancer patients ages <65 and ≥65 years (Figure 3B and C). To remove possible influence between the prevalence of anxiety and depression and the numbers of comorbid conditions, we also performed multivariable logistic regression analyses after adjusting for other potential contributors to anxiety and depression, such as age, geographic region, rural or urban residency, household income and type of health insurance. After adjusting for these covariables, there was 17% odds for anxiety (adjusted odds ratio (AOR) [95% CI]: 1.17 [1.15-1.19], P < .0001) and 24% odds for depression (AOR: 1.24 [1.21-1.26], P < .0001) increased for breast cancer patients with each additional comorbid condition (Figure 4A). We also found Charlson comorbidities index was significantly associated higher odds of anxiety (AOR: 1.06 [1.03-1.09], P < .0001) and depression (AOR: 1.15 [1.12-1.19], P < .0001) among newly diagnosed patients with breast cancer (Figure 4B). Proportion of breast cancer patients with anxiety (light blue line), depression (blue line) by indicated number of comorbid conditions during the first year after the first diagnosis date of breast cancer (A). Proportion of breast cancer patients with anxiety (B) or depression (C) by age group (age <65 blue line, ≥65 orange line) and indicated number of comorbid conditions during the 1st year after the first diagnosis date of breast cancer. The solid dots indicate the average, and the high and low bars indicate 95% confidence intervals. Forest plot of odds ratios of number of comorbid conditions (A) and Charlson comorbidities index (B) for anxiety and depression during the first year after breast cancer diagnosis. The vertical blue dashed line represents a odds ratio of 1, which is associated with equal odds for both groups. For each odds ratio displayed, the symbol red solid dot depicts the mean, and the blue horizontal line represents the 95% confidence intervals. Lines which do not cross the blue dashed vertical line are statistically significant. Multivariable logistic regressions were performed to calculate adjusted odds ratios (AOR) with corresponding 95% confidence intervals (CI). Adjusted co-variables included: age, geographic region, rural urban residence, household income, type of health insurance plan.
Prevalence of Anxiety and Depression among Patients with Breast Cancer Stratified by potential Psychological Distress-related Factors at baseline.

*Excluded breast cancer.
Multivariable Regression Analysis of Risk Factors Associated with Anxiety and Depression.
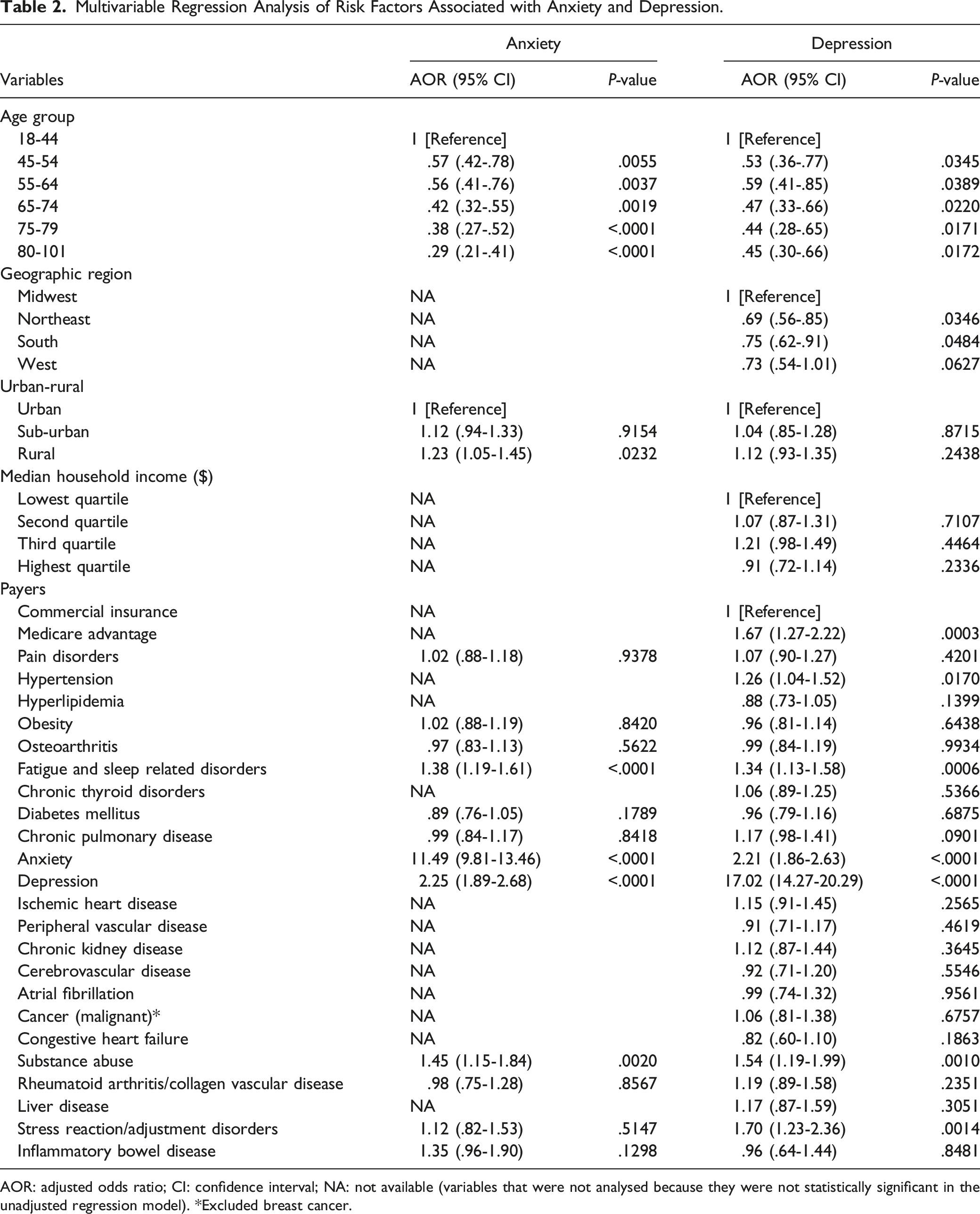
AOR: adjusted odds ratio; CI: confidence interval; NA: not available (variables that were not analysed because they were not statistically significant in the unadjusted regression model). *Excluded breast cancer.
The associations of specific comorbid chronic condition with anxiety and depression were assessed via logistic regression analyses, either univariate unadjusted (Supplementary Table 5) or adjusted for covariates (Table 2). Only fatigue and sleep related disorders (AOR: 1.38 [1.19-1.61], P < .0001) and three baseline psychiatric disorders: anxiety (AOR: 11.49 [9.81-13.46], P < .0001), depression (AOR: 2.25 [1.89-2.68], P < .0001), and substance abuse (AOR: 1.45 [1.15-1.84], P = .002) were significantly associated with higher odds of anxiety. Hypertension (AOR: 1.26 [1.04-1.52], P = .017), fatigue and sleep related disorders (AOR: 1.34 [1.13-1.58], P = .0006) and four baseline psychiatric disorders: anxiety (AOR: 2.21 [1.86-2.63], P < .0001), depression (AOR: 17.02 [14.27-20.29], P < .0001), substance abuse (AOR: 1.54 [1.19-1.99], P = .001), stress reaction and adjustment disorders (AOR: 1.70 [1.23-2.36], P = .0014) were significantly associated with higher odds of depression.
Discussion
Using a large administrative healthcare claims database, we found that 86.9% of newly diagnosed patients with breast cancer had at least two comorbid conditions, 77% had 3 or more, and 56.1% had 5 or more comorbid conditions. The median number of comorbid conditions was 5. Our study revealed that the summed proportion of multimorbidity of two and more comorbid conditions in patients age ≥65 years was significantly higher than those age <65 years. The most common individual comorbid conditions are pain disorders (63.7%), hypertension (62.2%), hyperlipidemia (60.9%), and obesity (30.7%). These patterns were in line with the findings of previous research.4,8,10,11 There are no standard operational definitions for comorbid conditions that should be included in such studies and no gold standard to measure comorbidity in the context of cancer,21,22 some just measured CCI,10,23,24 many measured different set of comorbid conditions.4,10,25-29 Therefore, we included the top 45 most common chronic conditions, which represented the wide spectrum of comorbidities among breast cancer patients and are the most in the same kind studies. Due to the limited space for survey questionaries or instruments, both health surveys and patient registries can only collect carefully selected data. 37 Unlike surveys or registry-based studies, we were able to include a wide spectrum of comorbid conditions, which are available in the healthcare claims databases. 37
To the best of our knowledge, this study is the first large-scale, population-based study evaluating the overall burden of comorbidity and multimorbidity and their association with anxiety and depression among newly diagnosed patients with breast cancer in the US. This work highlights the complexity of the growing population of breast cancer survivors; it shows that 27.7% of breast cancer patients experienced anxiety and 21.9% experienced depression during the first year after the breast cancer diagnosis. The prevalence of anxiety and depression were 29.1% and 23.9% among the breast cancer patients with multimorbidity respectively, which were significantly higher than those without multimorbidity (anxiety: 18.4%, depression: 8.9%). The prevalence of anxiety and depression among breast cancer patients increased as the number of comorbid conditions increased, which were consistent with the findings of previous studies.17,38 The same trends were found in breast cancer patients both age <65 and ≥65 years. We found that the prevalence of anxiety and depression varied by age. Younger patients more likely experienced both anxiety and depression, which was in line with other studies.17,38-41 This calls attention to the importance of preventing and early screening of anxiety and depression among middle aged patients with breast cancer and not only their older counterparts. Living in rural area was more likely to experience anxiety, which reinforces calls for improving mental health care in resource-poor rural communities. However, geographic region, household income, and type of health insurance are not significantly associated anxiety. Compared with patients lived in US Midwest, patients in Northeast and South are less likely to experience depression. Compared to commercially insured patients, patients with Medicare Advantage health plan are more likely to experience depression. Urban rural residency and household income are not significantly associated depression in this population.
Few studies have assessed the associations between individual comorbid conditions and the risk of anxiety and depression in breast cancer. In one observational cohort study, Burgess et al observed that previous psychological treatment predicted anxiety, depression, or both in the first 2 years after breast cancer diagnosis. 40 One recent study found that comorbid psychotic disorders were significantly associated higher risk of anxiety and depression among patients with breast cancer. 41 In this study, we found that fatigue, sleep disorders, three most common psychiatric disorders including anxiety, depression, and substance abuse were strongly associated higher odds of both anxiety and depression after breast cancer diagnosis. Hypertension, stress reaction and adjustment disorders were also significantly associated with higher odds of depression. Further research on the associations between specific comorbid conditions and anxiety and depression after cancer diagnosis would be beneficial to find the risk factors and build predictive models to screen and identify patients with high risk of anxiety and depression for early intervention.
Foster and Niedziedz found that 30.1% women with breast cancer had two or more chronic conditions, 5.3% of patients had current depression. A strong, dose-response relationship was found between multimorbidity and the likelihood of depression (OR: 2.09, 95% CI: 1.56-2.79 for two conditions and OR: 6.06, 95% CI: 3.63-10.14 for five or more conditions) among women UK Biobank participants with breast cancer. 17 The prevalence of multimorbidity and depression were lower than our findings. There are three main reasons may explain the differences: first, the average UK Biobank participant was healthier than the average member of the UK population second, different age range, the age range was 40-70 years at the time of recruitment in their study cohort. 17 Third, their comorbid conditions were self-reported, and depression was measured by PHQ-2 (Patient Health Questionnaire 2 item version). They used the cutoff threshold of ≥3 to identify more severe depression and there are some potential limitations with the approach, including lower sensitivity, but higher specificity compared with PHQ-9 cutoff scores ≥10 alone.17,42 Nevertheless, both studies clearly demonstrated a strong association between the number of comorbid conditions and the risk of depression. Another large-scale populations-based studies in UK reported that compared to women with no prior cancer, breast cancer survivors had higher risk of anxiety and depression. The relative risks estimate tended to decrease overtime, but anxiety and depression were significantly increased for 2 and 4 years after breast cancer diagnosis, respectively. 20
Like our study, 31.7% of breast cancer patients experienced anxiety, 22.0% had depression in a cross-sectional study conducted in Malaysia. 39 Younger age and low income were associated with higher risk of anxiety. Having less financial support and living alone were associated with higher risk of depression. 39 However, they did not examine the associations of multimorbidity with anxiety and depression. Yan et al conducted a cross-sectional study among 1546 survivors of all cancer types in China and found that the prevalence of anxiety and depression were 28.2% and 48.2%, respectively. When compared with those without any comorbidity, cancer patients with 1-2 comorbid conditions and ≥3 comorbid conditions had higher risks of anxiety and depression. 38 All these findings underscore the importance of preventing and managing multimorbidity in breast cancer patients, especially younger women, as an important strategy to improve mental health and QOL.
The presence of multimorbidity greatly increases the complexity of cancer care.43,44 For instance, multimorbidity could complicate or delay cancer, anxiety, depression, and other diagnoses, limit the possibility to receive optimal treatments, delay their initiation, decrease adherence and persistence, increase the risk of polypharmacy and adverse drug interactions.16,43-48 Most importantly, a high burden of comorbid conditions leads to decreased survival in cancer.23,30,44,48-50
As a retrospective observational study, although we were unable to determine the causal relationships between multimorbidity and anxiety and depression, our findings regarding these associations are valuable. Anxiety and depression do negatively impact health status and QOL but also complicate breast cancer care and increase the risk of mortality.6,7,40,50 A recent large prospective study demonstrated that depressive symptoms are strongly associated with new-onset risk of chronic diseases and multimorbidity, and the risks were almost lower with newly developed and relieved depressive symptoms than with persistent depressive symptoms, suggesting the potential benefits of active management of depressive symptoms to reduce the risk of emergent diseases in middle-aged and elderly population. 51
This work highlights the need for effective strategies to reduce the burden of anxiety and depression in patients with breast cancer, and especially in patients with breast cancer who have multimorbidity. In randomized clinical trials, cognitive behavioral therapy (CBT) and Cognitive-Behavioral Stress Management (CBSM), a combination of cancer-specific CBT and relaxation training, have been shown to effectively reduce anxiety and depression as well as pain and fatigue in patients with breast cancer.52-54 CBSM maybe especially suitable for those with multimorbidity since it is non-pharmacotherapy and without elevated risk of polypharmacy and adverse drug events. Our study emphasizes the importance of prevention, recognition, and managing of chronic conditions among patients with breast cancer. Most biomedical and health related research is currently focused on the prevention and management of disorders in isolation. 13 Prevention and active management of anxiety, depression, and multimorbidity in breast cancer warrants further research in prospective observational studies, especially in randomized pragmatic trials, which are more inclusive of comorbidities and in real-world setting.
Limitations
This study had several limitations. First, this was a retrospective observational study. Therefore, we may have underestimated the prevalence of multimorbidity, anxiety, and depression in the study.32,55 Since identification of all comorbid conditions was based on ICD-10-CM codes only, coding errors and misclassification were likely. However, this approach is conventionally used in many observational studies.8,11,32,37,46,55 Second, we have not compared multimorbidity, anxiety and depression before and after breast cancer diagnosis and between breast cancer population and general population in the current study. Multimorbidity, anxiety and depression may pose a risk for new-onset chronic diseases and multimorbidity, 51 which need further studies. Third, there is no gold standard and operational definitions for comorbid conditions that should be included in such studies,13,21,22 so we included the top 45 most common comorbid conditions. Though the number of conditions is adequate to assess overall multimorbidity, 14 some rare chronic conditions which may be associated with mental health after cancer diagnosis could be missed in the study. Fourth, we did not examine the cancer related therapy or other undergoing treatments which may lead to new-onset comorbid conditions. These treatments and new-onset comorbid conditions could be a source of psychological distress or precipitate mental health disorders. Fifth, some clinical information that would have been very helpful is not available in the claims data, such as the stage of breast cancer, exact diagnoses and their timing, and the severity of comorbid conditions. Sixth, we do not know patient’s race and ethnicity, marital status, education level, employment, smoking, alcohol consumption, and social support; all these factors may be associated with mental health after breast cancer diagnosis.17,25 In addition, the study results and implications may not be generalizable to the overall population in the US, as well as to other countries, for a variety of reasons.37,55
Conclusions
Multimorbidity was highly prevalent among patients with breast cancer and was strongly associated with increased risk of anxiety and depression. Each additional comorbid condition was associated 17% and 24% higher odds of diagnosed anxiety and depression, respectively. Comorbidity and multimorbidity patterns vary considerably across breast cancer patients and by age. As breast cancer patients survive longer, they accumulate more comorbidities. The presence of multimorbidity, anxiety, and depression should be considered in the context of clinical and policy decision making to improve mental health, QOL, and breast cancer care.
Supplemental Material
Supplemental Material - Multimorbidity and Its Associations With Anxiety and Depression Among Newly Diagnosed Patients With Breast Cancer: A Retrospective Observational Cohort Study in a US Commercially Insured and Medicare Advantage Population
Supplemental Material for Multimorbidity and Its Associations With Anxiety and Depression Among Newly Diagnosed Patients With Breast Cancer: A Retrospective Observational Cohort Study in a US Commercially Insured and Medicare Advantage Population by Dingwei Dai, Henriette Coetzer, Sean R. Zion, and Michael J. Malecki in Cancer Control
Footnotes
Author Contributions
DD was responsible for study design, statistical analysis, visualization, and drafting of the manuscript. HC was responsible for clinical concept, study design, and validation. SZ was responsible for review, editing, and validation. MM was responsible for obtained funding, study design, statistical analysis, and drafting of the manuscript. All authors fully contributed to the content of this manuscript and met the four criteria of the Internal Committee of Medical Journal Editors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DD and HC were employees of CVS Health Clinical Trial Services LLC, which received funding from Blue Note Therapeutics, Inc. to complete this research. SZ and MM were employees of Blue Note Therapeutics, Inc. at the time the study was conducted.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Blue Note Therapeutics, Inc.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.