
Abstract
Introduction
Women with breast cancer eligible for neoadjuvant therapy (NAT) present a disorder of biopsychosocial variables and alteration of their quality of life. They cope with this changing by adopting psychological adjustment strategies, either passive or active. This systematic review aims to investigate the psychological distress, coping strategies, and quality of life in breast cancer patients under neoadjuvant therapy.
Methods
Cochrane Library, PubMed, ScienceDirect, Scopus, Web of Science, and Wiley Online library represent the databases that were searched to identify relevant published articles until September 27, 2021. Full-text published articles, written in English and assessing the main outcomes (namely: psychological distress, coping strategies, and quality of life) in women with breast cancer under NAT will be included. Also, we will integrate papers dealing with the related bio psychosocial variables to the main variables. The paper selection, data extraction, and quality assessment of selected studies will be performed independently by two researchers, and disagreements will be resolved through discussions. We will bring together the results of all of the included studies to draw conclusions based on the body of evidence. The narrative approach will be adopted to analyze the results and conclusions extracted and we would perform quantitative groupings if we have similar data.
Ethics and dissemination
Ethical approval is not required as the proposed systematic review will not use primary data. The results of this review will be disseminated through publication in a peer-reviewed journal and conference presentation(s). PROSPERO registration number: CRD42021230300.
Keywords
Introduction
Breast cancer (BC) is the second most common cancer all over the world with 2,088,849 new cases in 2018 and is the most common cancer in the female population with a global incidence of 46.3/100,000 women and 626,679 death cases. 1 BC is a heterogeneous disease with different molecular subtypes. It is routinely performed by immunohistochemical analyses in order to mark different subgroups and serve as biomarkers for therapeutic decisions.2,3
Locally advanced breast cancer (LABC) represents a variety of tumors ranging from slow-growing cancer to rapidly proliferating and aggressive cancers. 4 LABC is defined by the size of the tumor that exceeds 50 mm, which implies the skin of the breast/chest wall, supra/infraclavicular lymph nodes, or multiple axillary lymph nodes. 5 This includes T3 or T4 and N2 or N3 tumors (stage IIB-T3N0 to stage III). 6 Studies show that 4% of patients with BC have LABC in Europe, 8.5% in America, 7 while the situation is alarming in developing countries with an incidence rate between 33% and 77%. 4 For patients with LABC, neoadjuvant therapy (NAT) is recommended to reduce the extent of surgery and to facilitate breast-conserving surgery8,9 or to reduce the size of LABC previously considered unresectable.5,10,11
NAT provides potential opportunities for predicting response 12 and allows rapid assessment for the development of suitable therapy for BC 13 by seeking its benefits from the early stages of cancer. That is why the National Comprehensive Cancer Network (NCCN) BC guidelines 14 recommend consideration of NAT for women with LABC as an integral part of the multi-modality approach including also surgery, radiotherapy, hormonal therapy, and/or targeted therapy.
Thereby, preoperative or NAT, initially used for LABC has become more common in patients with the BC operable, especially those with larger primary tumors.15,16 It is based either on cycles of neoadjuvant chemotherapy (NACT) or neoadjuvant endocrine therapy (NET).3,17
NACT was introduced in BC treatment in the 1970s18,19 to reduce the stage of the LABC disease (inoperable) and make it operable. Anthracycline and taxane-based regimens are the standard primary NACT for LABC. 14 In general, the most commonly used combination is the bi-weekly (dose-dense) or tri-weekly (doxorubicin-cyclophosphamide) combination, followed by 12 weekly paclitaxel or four tri-weekly cycles of docetaxel and its efficacy has been previously demonstrated. 20 For HER2-positive BC, NACT includes administration of chemotherapy with anti-HER2 monoclonal antibodies, such as trastuzumab and pertuzumab.3,21 While Neoadjuvant endocrine therapy (NET) may be beneficial for LABC patients with estrogen receptors (ER) positive or progesterone receptors (PR) positive since it can decrease the tumor size and improve breast-conserving surgery rates. 22 Two applications of NET are possible, the first inhibits the production of estrogen used by aromatase inhibitors (AI) including letrozole, anastrozole, and exemestane, or by luteinizing hormone-releasing hormone agonists in premenopausal women. The second approach targets the ER itself and is used by drugs such as tamoxifen or fulvestrant.23,24 In most cases, the administration of NET lasts 3 to 6 months. 25 Researchers have studied26,27 the efficacy of NET and found promising results in ER-positive BC patients, leading them to suggest it may be less toxic than NACT.
During the period of diagnosis and administration of CTNA, patients are often exposed to unpleasant changes and physical symptoms. They also experience discomfort28-32 and deleterious effects on their quality of life and especially on their psychological state. 33 Among these symptoms, peripheral neuropathy can be caused by antineoplastic agents such as taxanes. It is characterized by numbness, paresthesia, and pain.34-37 Also, NACT can cause persistent pain38-40 which is associated with poor quality of life after treatment.41-43 In the study of Saibil et al, 44 87% of BC patients reported they suffered pain during anthracycline or taxane chemotherapy and 79% confirmed experiencing their worst pain during treatment with taxane. Fatigue remains a well-known side effect of chemotherapy 45 and can negatively impact multiple facets of a patient’s life. 46 Several studies have shown fatigue occurs even before the start of treatment.47,48 Therefore, fatigue especially in association with pain or other symptoms can increase anxiety and depression. 49 Emesis is another side effect of NACT 50 and it occurs highly with the combination of doxorubicin (anthracyclines) and cyclophosphamide. 51 In addition, patients who undergo NACT usually develop alopecia, which causes psychological distress and may affect the body image and quality of life. 52 In phase II neoadjuvant trial, 53 the therapy with epirubicin (anthracyclines) and docetaxel (taxanes) was evaluated in patients with large, operable breast carcinoma or LABC, and with inflammatory breast carcinoma. A clinically significant proportion of patients (25%) suffered from diarrhea, 43.3% from oral mucositis, and 26.6% from emesis. Also, 80% of them developed grade 4 neutropenia, while one third suffered febrile neutropenia.
On the other side, it is well documented that cancer and its treatment are linked to alarming psychological disorders54,55 which may vary depending on types and combinations of therapy, dosages, and number of treatment cycles, as well as other individual correlates such as age, comorbidity, level of social support, and coping strategies.56,57 Psychological distress is the most prevalent in BC 58 and it negatively affects the quality of life 59 and increases the risk of mortality.60,61 If the psychological distress of BC patients was ignored and left untreated 62 and was not recognized by the care team, and if no support has been provided to improve their psychological state, certain problems arise, namely, the non-compliance with treatment,63,64 the non-participation in therapeutic decisions, and the increase in the number of patients visits which will be stressful for the oncology team. 65 In general, psychological distress refers to anxiety and/or depression symptoms58,66,67 which are the most documented disorders affecting two-thirds of women with BC.68-70 Meta-analyses have found that depression and anxiety are very common among BC patients, with a percentage of 32.2% and 41.9% 71, 72, respectively.71,72 There is evidence that depression and anxiety may contribute to the suffering of patients, impair their physical capacity and quality of life, affect their ability to adhere to therapy, and also lead to mortality of those patients.60,73
All of these aroused physical and psychological symptoms increasingly interfere with the daily life of BC patients by limiting their social roles within the family and the community. 74 They develop negative feelings, causing poor perceptions of their self-image, disrupting their sexuality, and lowering their self-esteem. Moreover, the stigma associated with surgery can also create a great deal of stress and troubles, causing women to adopt different coping strategies.75,76 However, the coping strategies mobilized by the patients differ and take several forms, such as emotional expression, positive cognitive restriction, the practice of certain exercises such as yoga, acceptance of the disease, wishful thinking, religious practice, and social and family support. 77 Coping strategies used by women with cancer are important elements of psychosocial adjustment that protect patients from psychosocial distress. 78 Adjustment to neoplastic disease is an issue of coping not only with the illness itself but also with its side effects, such as pain, uncomfortable feelings, and other changes affecting the quality of life in the long term.79,80 In one study, it was found that BC patients on chemotherapy with a low level of anxiety tend to use a problem-solving strategy to deal with their anxiety, 81 while depression symptoms increased with lowered positive reframing, higher acceptance, self-blame, and negative body image. 82 Patients with BC who used approach-focused coping strategies, (for example, fatalism, social support, future perspective, and fighting spirit) reported fewer feelings of depression and anxiety and reported better quality of life. 82 Positive psychological attributes (like optimism) and adaptive coping strategies such as seeking solutions to problems, seeing the positive aspects of cancer, and sharing feelings related to cancer, all help improve psychological adjustment and quality of life. 83 Religious coping and spirituality can also reduce depression, improve quality of life and increase feelings of control, especially if women with BC have a positive perception of God and adopt acceptance as a coping strategy.84-86
Due to the particular characteristics of the pathway of patients who are candidates for NAT that differ from other current treatment options like primary surgery and because of critical times such as the moment of diagnosis, NAT sessions and their side effects, the moments of the clinical, radiological, and histological response of NAT and to other expected steps management, namely, surgery, radiotherapy, and if necessary hormone therapy or targeted chemotherapy, it becomes relevant to explore the psychological distress, the quality of life and to study patients’ attempts to adapt during this treatment.
In this regard, we believe that the establishment of a systematic review on this topic would be enriching of literature and will provide answers to the needs of these patients. Our research has shown that since the 1990s, several systematic reviews and meta-analyses have evaluated this variable in breast cancer. These reviews either looked at one of these variables71,72,87-93 or related to a particular type of breast cancer70,94-96 or a particular time of their therapy or are examined during a specific treatment modality64,97-101 or in breast cancer survivors.68,102,103 However, these studies did not examine any of these variables specifically in patients who were receiving NAT. Thus, our primary objective of the systematic review which we will carry out is to identify the best available evidence related to psychological distress, strategies adjustment, and quality of life in BC patients receiving NAT. The secondary objectives of our systematic review are (a) to explore other psychological, social aspects, and the symptoms reported by patients during neoadjuvant therapy, (b) to understand the experiences of patients and the problems they live during neoadjuvant therapy, and (c) to assess different interventions implemented to improve aforementioned variables. Thus, the results of this systematic review will assist clinicians in improving their management skills and knowledge, as well as highlight potential areas for additional strategy plans to promote the mental health of patients and their quality of life and to support them in adopting effective adjustment strategies during NAT.
Methods
This article presents a protocol of a systematic review, written according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols guidelines (PRISMA-P), as shown in the PRISMA-P checklist in supplemental file 1. 104 This protocol presents an objective and clear procedure for maximizing information extraction from articles that study psychological distress, coping strategies, and quality of life, and which have been reported separately or jointly in patients receiving neoadjuvant chemotherapy. The protocol has been registered at the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number: CRD42021230300, which is available at: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=230300.
This protocol’s registration in the PROSPERO database and the publication of this article will ensure transparency in the writing process for the full text of the systematic review and improve the writing of the content based on reviewers’ comments.
Inclusion and Exclusion Criteria
We focus on the PICOS (population, intervention, comparison, Outcome of the included studies) as the basis for determining which studies can be grouped for synthesizing study characteristics.
Population
This review will consider studies that include women aged over 18 with breast cancer under one of two neoadjuvant treatments, either chemotherapy or endocrine therapy. Neoadjuvant chemotherapy is given to a patient with LABC, including generally T3 or T4, and N2 or N3 tumors (according to the TNM classification). For Neoadjuvant endocrine therapy, it offered for patients with strongly hormone-positive tumors.
Intervention
Studies will be included if they have assessed any intervention applied to diagnose and assess psychological distress, mobilized coping strategies, and aspects of quality of life. We are also interested to Studies which assess the other psychological and physical correlates and any intervention used to manage and prevent these different variables.
Comparison
We focus on studies that compare the changes in the outcomes studied concerning the time (T) of diagnosis of breast cancer and the different steps of administration of neoadjuvant therapy. For example: T0 corresponds to stage of diagnosis and before administration of NAT and T1 corresponds to moment after NAT and before surgery, or Tn with n corresponds to the NAT cycle number.
We also include all studies dealing with comparisons between groups of patients with breast cancer under NAT compared to patients undergoing the first surgery or compared to other cancerous pathologies treated by a NAT.
Outcomes
Following the definition of psychological distress in the NCCN 105 Guidelines for Managing Distress that it considers as “a multifactorial and unpleasant experience of a psychological (i.e., cognitive, behavioral, emotional), social, spiritual nature. and/or physical which may interfere with the ability to effectively cope with cancer, its physical symptoms and treatment”, We draw from this definition the main and secondary outcomes related to the psychological situation in patients with breast cancer candidates for NAT. We consider psychosocial distress, depression, anxiety, coping strategies, and quality of life in breast cancer patients ongoing NAT as the main outcomes. As regards the quality of life, we prefer to introduce above all its component dimensions, in particular the psychological, social, and physical dimensions. Moreover, we consider secondary main outcomes the following concepts: patient information and decision support, social support, physical symptoms, patient perception, and experiences.
Thus, studies will be included if they have objectively measured or explored this main or secondary outcomes, separately or jointly, in patients receiving neoadjuvant chemotherapy.
Type of Studies
Studies eligible for inclusion in this review were those using an observational study design (e.g., cross-sectional, prospective, case-control, and retrospective designs, with a quantitative and/or qualitative method) and examining the outcomes, primary and/or secondary, or the associations between them. This systematic review also will include psychological interventions, randomized controlled trials, experimental pharmacological studies that assessed and/or improved main and secondary outcomes.
Literature reviews, books, abstracts, letters, editorials, case reports, conference abstracts, abstracts of unpublished studies, grey literature will be excluded from the analysis.
Language
The systematic review will be limited to studies published in English.
A Summary of the PICOS Elements that Comprise the Systematic Review.

Information sources and search strategy
The following databases were searched to identify relevant articles published: Cochrane library, PubMed, ScienceDirect, Scopus, Web of Science, and Wiley Online library.
Bibliographic research was also extended to other sources and specific journals. Besides, the authors reviewed the reference lists of documents identified in certain journals (i.e., The Breast, Journal of Breast Cancer, The Lancet Oncology, J, The Breast Journal). The published articles were supplemented by a manual search of reference lists and a forward citation search using Google.
The search used Boolean operators to combine free text terms and/or Medical Subject Headings (MeSH) terms including: - ‘‘Breast cancer”; Breast Neoplasms”; - “neoadjuvant therapy,” “neoadjuvant,” “neo-adjuvant,” “Preoperative,” “chemotherapy,” “Primary systemic chemotherapy,” “neoadjuvant endocrine”; - “psychological distress,” “depression,” “anxiety,” “anxiety disorders”; depressive disorder,” “Mental Disorders”; - “Coping,” “adjustment,” “adaptation,” “mental,” “psychological,” “adaptation,” “psychological,” “behavior, coping,” “Social support,” “family support,” “Patient information,” “informational support”; - “Quality of life,” “QOL,” “health-related quality of life,” “health-related quality of life,” “Health-related of QOL,” “HRQOL.”
Search Strategy Until September 27, 2021.

Data extraction
All articles and documents (n = 2.253) will be grouped and organized into collections using Zotero® reference management software. Each collection will have the name corresponding to each database. After all, research has been carried out, the references of each collection will be merged into a single Zotero® group which will subsequently be shared among the reviewers. We will then look for duplicates to identify them and merge them by relying on functions of the Zotero® software. We will export all the references of this group in a spreadsheet in CSV format and redefine the predetermined fields for the bibliographic characteristics of each data. The redefinition of the fields will be limited to: Year of publication, authors, title, abstract, DOI, URL, document type. We will also add in the same spreadsheet two columns, one to show if each study will be included or not, and the other to show the reasons for the exclusions.
Two reviewers will carefully read the titles and abstracts of each document to exclude those that do not meet the criteria for inclusion (as per PICOS) and to establish a pre-final list of articles to be included.
The reviewers will proceed to read the full text of the papers selected for the pre-final list to eliminate those that do not meet the criteria and design the final list of articles included in the systematic review. Disagreements between the two reviewers will be resolved through discussions with the other reviewers. Data extraction will be done in the same sheet.
The design of the PRISMA organization chart will be carried out based on the data extracted, specifying the number of duplicates, then analyzing the titles and summaries, as well as the full texts.
Analysis of Subgroups
Summary data for each article will be extracted into a data extraction form specifically designed for that journal. Summary tables will be created in Microsoft Office Excel for general information on the articles and information on the outcomes studied.
Among the General Information taken from each article, we will mention date and country of publication; sample size; type of study; age, ethnic origin, clinical data; NAT type and number of cycles.
Among the information related to outcomes, we will present the objectives of the study, the variables studied, the data collection instruments (questionnaire, interview, etc.), and the main results and conclusions.
By presenting the quantitative results of the included studies, we will see whether we will have the opportunity to establish a meta-analysis or not.
Discussion
The administration of NAT to women with breast cancer is an uncomfortable experience and influences the quality of life and social activities in women. However, to our knowledge, this is the first systematic review that will comprehensively assess biopsychosocial variables, coping strategies, and levels of quality of life in patients under this type of treatment. Several bibliographic databases will be systematically searched on the date of the search.
Conducting an inclusive search of major databases will maximize the coverage of original research studies on this topic. We will undertake a narrative approach to synthesizing data. A complete analysis of the subgroups should lead to a better investigation of the variables to be studied.
Therefore, this systematic review will examine the psychological distress in patients during treatment administration and describe the degrees of depression and anxiety as well as the coping strategies they adopt. We will seek to assess their evolution from the first oncology consultations until the days following the administration of the last doses of neoadjuvant therapy.
Besides, we will analyze the adaptive role of the coping strategies mobilized by these patients and determine the biopsychosocial factors associated with the level of psychological distress and the types of coping strategies adopted.
Since the quality of life study would generally examine biological, psychological, and social aspects, we will also seek to show those aspects of quality of life examined in the studies included in this systematic review and analyze their results.
Complete subgroup analysis should lead to a better investigation of the factors influencing the association of NAT in breast cancer with psychological distress, coping strategies, and quality of life. The results of the present study should provide a better understanding of the relationship between common mental health problems and biopsychosocial factors in these patients. This will provide a better understanding of the keys to the success of neoadjuvant therapy in breast cancer.
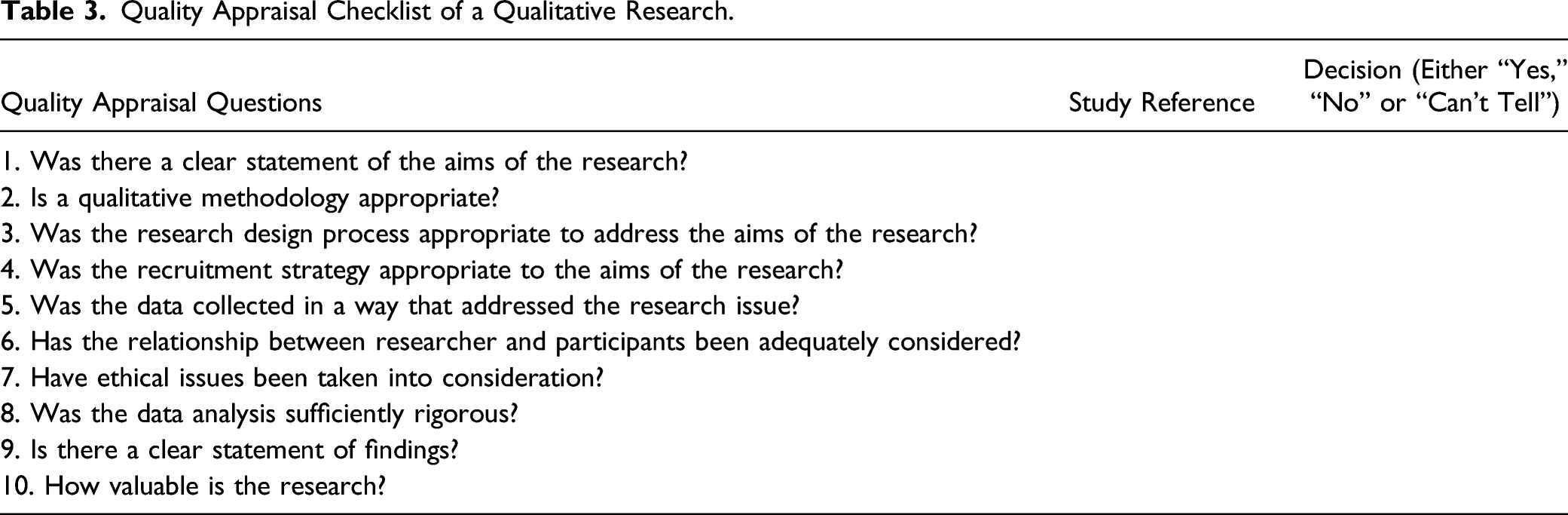
Quality Appraisal
Quality Appraisal Checklist of a Qualitative Research.
Qualsyst Quantitative Scoring Tool.

Strength and Limitations of This Study
- The systematic review will produce a comprehensive assessment of the variables of psychological distress, coping strategies, and quality of life of patients with breast cancer receiving neoadjuvant chemotherapy; - To our knowledge, no systematic review has been conducted to assess psychological aspects and the coping strategies adopted by women with breast cancer ongoing neoadjuvant therapy; - The systematic review protocol is registered with the International Prospective Register of Systematic Reviews (PROSPERO) and is reported following Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) statement; - Non-English electronic databases will not be searched. This limitation may cause language bias.
Conclusion
This systematic review seeks to summarize the results of articles around psychological stress, quality of life, and coping strategies in breast cancer patients under NET. The outcomes of this systematic review will address this gap in the literature and provide insight into biopsychosocial factors of patients with advanced locally breast cancer during undergoing NET.
Moreover, these results provide an opportunity to implement specific interventions targeted at these patients such as educational and psychosocial support. Also, they would allow establishments to optimize and improve patient care during these treatments and train caregivers in best practices that function within the domain. From the synthesis of this systematic review, avenues for research on psycho-oncology in these patients could be also carried out.
Supplemental Material
sj-pdf-1-ccx-10.1177_10732748221074735 – Supplemental Material for Psychological Distress, Coping Strategies, and Quality of Life in Breast Cancer Patients Under Neoadjuvant Therapy: Protocol of a Systematic Review
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748221074735 for Psychological Distress, Coping Strategies, and Quality of Life in Breast Cancer Patients Under Neoadjuvant Therapy: Protocol of a Systematic Review by Majid Omari, Zarrouq Btissame, Lamiae Amadour, Zineb Benbrahim, Achraf El Asri, Nawfel Mellas, Karima El Rhazi, Mohamed El Amine Ragala, and Karima Halim in Cancer Control
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This protocol research is supported by Moffitt Cancer Center under the NIH International Fogarty Center for the award number 5D43TW009804, PI Anna Giuliano.
Systematic Review Registration Number
International Prospective Register of Systematic Reviews (PROSPERO), registration number: CRD42021230300. Additions and possible modifications will also be recorded in PROSPERO to guarantee the criterion of transparency
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.