
Abstract
Objectives
Though menstrual and reproductive factors have been associated with the risk of breast cancer in many populations, very few studies have been conducted among Vietnamese women. This study aimed to assess the association between menstrual and reproductive factors and the risk of breast cancer in Vietnamese women.
Methods
A retrospective case-control study of 490 breast cancer cases and 468 controls was conducted in Northern Vietnam. Unconditional logistic regression models adjusting for confounders were used to estimate odds ratios (ORs) and their 95% confidence intervals (CIs) for the associations of menstrual and reproductive factors with the risk of breast cancer; overall and by cancer subtype.
Results
Among breast cancer patients, the luminal B subtype was the most frequent (48.6%), followed by HER2-overexpressing (24.5%), luminal A (16.7%), and triple-negative breast cancer (TNBC; 10.2%). Among menopausal women, menopausal age at 50 years or older (OR = 1.71, 95% CI: 1.15-2.57 vs. <50 y) was associated with an increased risk of breast cancer. Earlier age at menarche (<13 y) was associated with a significantly increased risk of breast cancer (OR = 2.66, 95% CI: 1.08-7.51) among premenopausal women only and the luminal A subtype of breast cancer (OR = 3.06, 95% CI: 1.04-8.16). Having more than two children was associated with a reduced risk of premenopausal (OR = .42, 95%CI: .21-.83), luminal B (OR = .43, 95% CI: .24-.79), and TNBC (OR = .34, 95% CI: .14-.89). Later menopause was positively associated with the risk of breast cancer with HER2 overexpression (OR = 2.19, 95% CI: 1.14-4.23).
Conclusion
Associations of menstrual and reproductive factors with breast cancer among Vietnamese women, particularly for among premenopausal women and for the luminal A subtype, are generally consistent with those reported from other countries. These findings suggest that changes in menstrual and reproductive patterns among young Vietnamese women may contribute to the recent rising incidence of breast cancer in Vietnam.
Introduction
Breast cancer is the most common cancer and the leading cause of death for women worldwide. The GLOBOCAN reported that there were 2.2 million new cases of breast cancer worldwide in 2020, accounting for a quarter of cancer cases among women. 1 In Vietnam, the incidence rate for breast cancer was 34.2 per 100 000 women, making it the most common cancer for women (25.8% of all cancers) and the fourth leading cause of cancer death overall, following lung cancer, liver cancer, and stomach cancer. 1
In the past few decades, breast cancer incidence rates have increased in developing countries, including Vietnam. Rising rates coincide with changes in lifestyle, population characteristics, and menstrual and reproductive patterns in these countries. 1 These changes include factors such as an increase of physical inactivity, obesity, dietary fat intake, alcohol consumption, early onset of menarche, late onset of menopause, nulliparity, late age at first birth, a decreased number of childbirths, and no or shortened duration of breastfeeding.2,3
Prior studies have consistently shown that prolonged endogenous and exogenous estrogen exposure increases the risk of breast cancer. 4 A meta-analysis of 117 studies in 2012 reported the associations between age at primiparity, parity, and at menopause with the risk of breast cancer. 5 Fewer parities and advanced age at first birth both increased the risk of ER+/PR+ cancer, but they were not associated with the risk of ER-/PR-cancer in most prospective studies. 6 A meta-analysis evaluated 15 studies, with 21 941 breast cancer patients and 864 177 controls, that investigated the impact of reproductive behaviors according to intrinsic subtype. 7 Parity and breastfeeding were associated with a reduced risk of developing luminal subtype, while later age at first birth was related to an increased risk of developing luminal subtype. 7 Breastfeeding was associated with a reduced risk of developing triple-negative breast cancer (TNBC) subtype. 7 Research on other reproductive factors, such as spontaneous abortion (SA) or induced abortion (IA), with breast cancer risk has yielded inconsistent findings. A 2015 meta-analysis of 15 prospective studies revealed non-significant associations of breast cancer with SA and IA. 8 These subtypes (luminal A, luminal B, HER2+, and TNBC) differ in age at diagnosis and prognosis. In addition, they may also differ etiologically and have different in risk factors. 9
Vietnamese women are experiencing significant changes in lifestyle and reproductive patterns. However, little is known about how these changes affect breast cancer risk. To our knowledge, only two small-scale studies on breast cancer have been conducted in Vietnam and the results were inconsistent.10,11 Herein, we report results from a large case-control study, the Vietnamese Breast Cancer Study (VBCS), focusing on the associations between menstrual and reproductive factors with breast cancer risk among Vietnamese women.
Methods
Study Population
We recruited newly diagnosed breast cancer patients (clinical diagnosis) aged 21 to 79 from inpatient surgical and chemotherapy units and outpatient units of the Vietnam National Cancer Hospital and the Hanoi Oncology Hospital. These are the two largest oncology hospitals in Northern Vietnam. Breast cancer patients with a prior history of cancer were not eligible for the study. Controls were selected from healthy relatives, neighbors, or friends of breast cancer patients (n = 64), or healthy women who were taking care of other cancer patients at these two hospitals (n = 402), and frequency was matched to cases on age (±3 years) and residence (urban/rural). Controls were recruited at approximately the same time as case recruiment. Women who had a history of cancer diagnosis were excluded from this study. Details of design and methods for the VBCS have been described previously. 12
A total of 501 newly diagnosed breast cancer patients and 468 controls were included in this study from July 2017 to June 2018 in Hanoi, Vietnam (response rates of 93.1% and 97.7% for cases and controls, respectively).We excluded case participants who were subsequently confirmed to have a benign tumor based on a pathological review (n = 9) or who were diagnosed at stage 0 (n = 2). Finally, 490 cases and 468 controls remained in the current study. Our study initially applied an age frequency matched design. However, during data collection, it was adapted to the individual matching study, in which cases and controls were individually matched to cases on age (±3 years), city, and province of residency. Thus, out of 490 cases and 468 controls, there are 374 individually matched case-control pairs. All patient information was de-identified. The protocol of this study was approved by the Vietnam National Cancer Institute (No.160530 – IRB approval issued May 30, 2016) and Vanderbilt University Medical Center (No.161039 “Vietnam Center of Research Excellence (V-CORE) - IRB approval issued May 31, 2018”). All patients provided written informed consent prior to enrollment in the study.
Assessment of Menstrual and Reproductive Characteristics
Information on menstrual and reproductive characteristics, demographics, lifestyle factors, medical history, and familial cancer history was collected through in-person interviews using a structured questionnaire built within the Research Electronic Data Capture (REDCap) mobile application. 13 In addition, anthropometrics, weight, height, waist, and hip circumferences were taken by trained interviewers following a standard protocol, from which body mass index (BMI) was calculated as weight (kg)/[height (m)]. 2 Data collected for the current study included age, marital status, residency (urban, rural), age at first menarche, age at menopause, menstrual cycle regularity and duration, parity, age at first live birth, age at last live birth, number of pregnancies and abortions, and total months of breastfeeding in a lifetime. Additionally, p postmenopausal status was defined as cease of menstruation naturally (i.e., excluding those brought on by pregnancy, surgery, or other treatments) for at least 12 months.
Menstrual and reproductive factors and covariates were categorized as follows in the study: age at menarche (<13 vs. ≥13 years, similar to publications from other Asian countries14,15), menopausal status (premenopausal vs. postmenopausal), age at menopause (<50 vs. ≥50 years), regularity of menstrual cycle (i.e., regular, irregular, sometimes irregular), length of the menstrual cycle (<26 days, 26-30 days, >30 days), number of pregnancies (0, 1, 2, 3, ≥4), parity (ever vs. never), number of livebirth (1, 2, ≥3), age at first live birth (<25, 25-29, 30-34, ≥35 years), abortion (never, induced only, miscarriage only, both induced and miscarriage), breastfeeding (ever vs. never), breastfeeding duration (<12, 12-23, ≥24 months), and family history of breast cancer (no vs. yes). Body mass index (BMI) was categorized using the World Health Organization’s classification for Asian populations: underweight (BMI < 18.5 kg/m2), normal/healthy weight (BMI ranges from 18.5 to 22.9 kg/m2), overweight (BMI ranges from 23 to 27.5 kg/m2) and obese (BMI > 27.5 kg/m2). Economic status was defined by annual family income (i.e., ≤50 million, 50-100 million, 100-150 million, 150-200 million, >200 million). 16
Data on ER/PR status and HER-2 expression was collected by reviewing medical charts from the Vietnam National Cancer Hospital and the Hanoi Oncology Hospital. ER and PR status, HER-2 expression, and Ki67 status were assessed by immunohistochemistry (IHC). Intrinsic tumor subtypes were classified as luminal A (ER-positive and/or PR-positive, HER-2 negative, and low Ki-67), luminal B (ER-positive and/or PR-positive, and HER-2 positive or HER-2 negative with high Ki-67), HER-2 overexpressing (ER-negative and PR negative, and HER-2 positive; HER 2+), and triple-negative (ER, PR, and HER-2 negative; TNBC).
Statistical Analysis
Differences in frequency distribution of categorical variables were evaluated by Pearson chi-square, while the Student t-test was performed to compare mean values of continuous variables between cases and controls. Unconditional logistic regression models were used to estimate odds ratios (ORs) and their respective 95% confidence intervals (CIs) for associations of breast cancer risk with menstrual and reproductive characteristics. The differences in ORs between the two groups, pre- and post-menopausal, was tested using Likelihood ratio tests. The multivariable logistic regression model was adjusted for potential confounders based on the literature. Tests for trends across categories were performed by assigning the median value for each category. Multivariable multinomial logistic regression was also performed to evaluate whether the observed risk estimates varied across molecular subtypes of breast cancer. We used likelihood ratio tests to evaluate heterogeneity across molecular subtypes. All analyses were performed using R version 4.1.0. A two-sided P-value of less than .05 was considered statistically significant.
The reporting of this study conforms to STROBE guidelines. 17
Results
Sociodemographic characteristics and familial cancer history of study participants.

Association between menstrual and reproductive factors and breast cancer risk.

Adjusted for age, first-degree family cancer history, income.
additionally adjusted for number of live births among parous women.
Association between menstrual and reproductive factors and breast cancer stratified by menopausal status.

*Pheterogeneity = .04, Test for heterogeneity.
Adjusted for age, first-degree family cancer history, income.
additionally adjusted for number of live births among parous women.
Association between menstrual and reproductive factors and breast cancer by intrinsic subtypes.
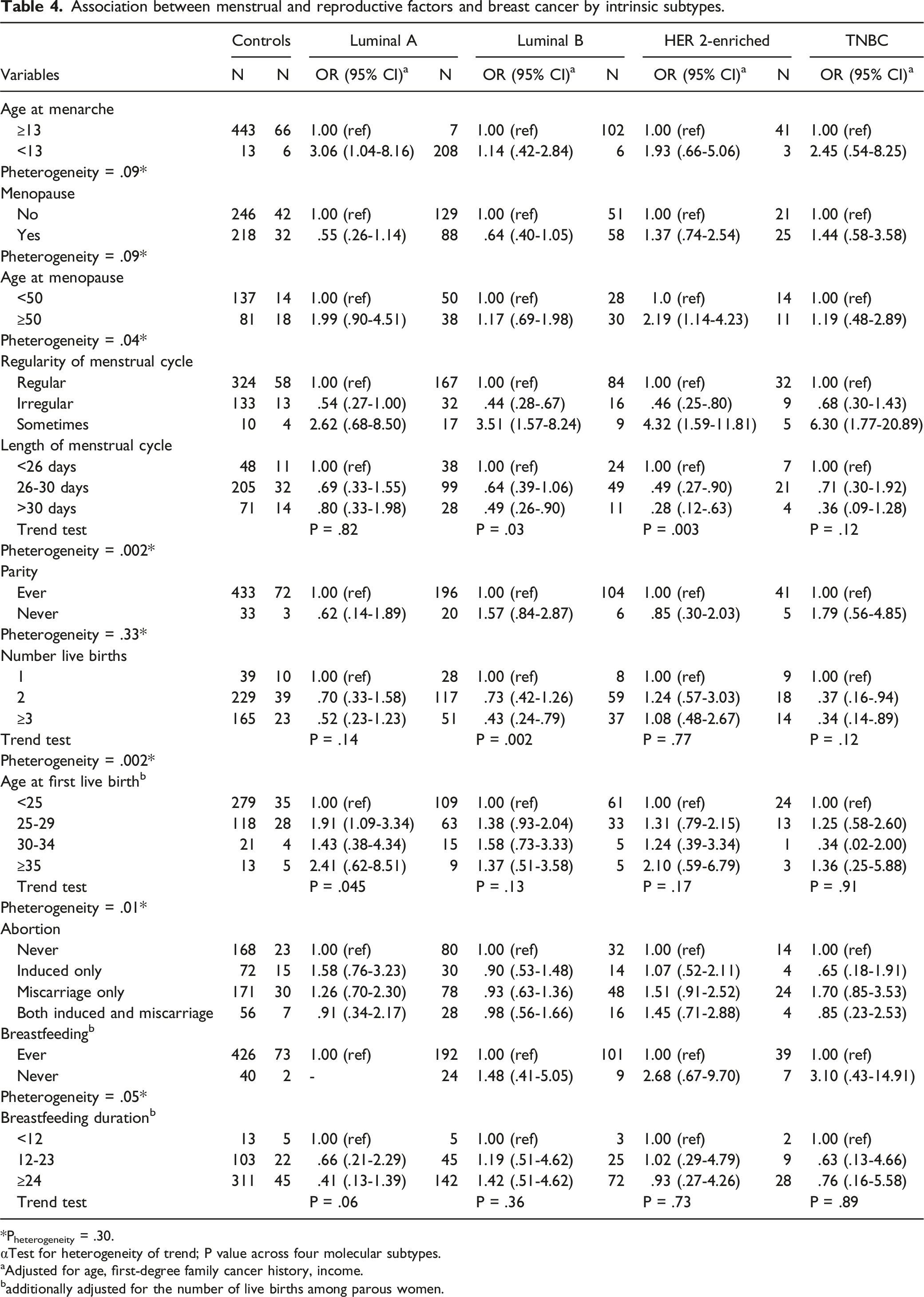
*Pheterogeneity = .30.
αTest for heterogeneity of trend; P value across four molecular subtypes.
Adjusted for age, first-degree family cancer history, income.
additionally adjusted for the number of live births among parous women.
Discussion
To our knowledge, this study is the largest case-control study of breast cancer and the first one to investigate breast cancer risk factors by tumor subtype in Vietnam. Most of our findings on menstrual/reproductive characteristic-breast cancer risk associations are consistent with those reported for Western and other Asian populations, while few previously established associations were not observed in our study.
Early age at menarche has been consistently associated with an increased risk of breast cancer in several Asian and Western populations.19-24 In our study, early age at menarche was associated with a non-significantly elevated risk of breast cancer overall. This association became significant among premenopausal women and for luminal A breast cancer. These findings are consistent with previous studies that showed the association between menarche and breast cancer was stronger for the luminal A subtype.15,25,26 Early-onset of menarche was related to early and greater cumulative exposure to estrogen, in which the presence of progesterone can increase the risk of breast cancer, particularly in the luminal A subtype in which estrogen exposure is most relevant. We found that the menarche-breast cancer association was mainly confined to premenopausal women is likely caused by a cohort effect as Vietnamese women traditionally have a late onset of menstruation (more than 97% of control participants began menstruation at ≥13 years of age). In addition, the age at menarche has decreased in younger generations. In our study, the average menarche age among controls was 15.7 years.
We found that women with irregular cycles had 48% and 56% reduced risks of breast cancer overall and for luminal B breast cancer, respectively. This finding is in line with reports from previous studies.27,28 Irregular menstrual cycles may be related to anovulation, leading to reduced exposure to estrogen and progesterone, and thus, lower risk of breast cancer. 29 The more than 3-fold elevated odds ratio for overall breast cancer, and most subtypes of breast cancer, associated with sometimes irregular menstruation has not been previously reported and may be caused by recall bias. Of note, the confidence intervals for the OR associated with irregular menstruation are extremely wide due to how few women reported having the condition. Therefore, this result should be interpreted with caution.
Similarly, late age at menopause is a well-established risk factor for breast cancer. Our results show that women aged 50 or over at menopause had an increased risk for breast cancer overall and HER-2+ and a suggested elevated risk of luminal A breast cancer. Late menopause is associated with increased lifetime exposure to estrogen, which may account for the increased risk of breast cancer. 30 The lack of significance for luminal A breast cancer is likely due to the small sample size.
Our findings on reduced numbers of live births and late age at first live birth being associated with an increased risk of breast cancer were consistent with results of previous studies,31-35 including those conducted in Vietnamese women.36,37 Our study, for the first time, showed that these associations varied by tumor subtype among Vietnamese women. Specifically, women with more than two children had a decreased risk of both luminal B and TNBC subtypes, and a suggested decreased risk of luminal A breast cancer, compared to women with one child. However, the number of live births was unrelated to HER 2+ breast cancer. These results support a different etiology for breast cancer subtypes, which warrants further investigation.
Our finding of a null association for miscarriage and abortion with breast cancer risk was consistent with a 2015 meta-analysis that showed no evidence from prospective studies on an association between breast cancer risk and abortion, including both induced and spontaneous abortion. 8
We did not find that the length of time breastfeeding was significantly associated with breast cancer overall and by subtypes in our study, which is inconsistent with some of the earlier findings.38,39 It should be noted that 96.6% of cases and 96.9% of controls in our study have had breastfeeding experience, most for longer than 12 months. Thus, our study has low statistical power to investigate the influence of no or short-term breastfeeding on breast cancer risk.
The large sample size, high participation rate, standardized data collection, and availability of breast cancer subtype information are significant strengths of our study. However, our study also has several limitations. First, our study was hospital-based; therefore, selection bias cannot be excluded. Nevertheless, the Vietnam National Cancer Hospital and the Hanoi Oncology Hospital are the leading hospitals treating most breast cancer patients in Northern Vietnam. Because most Vietnamese have government-provided health insurance, systematic selection bias is minimized. In addition, we have adjusted for education and family income in our analysis to reduce selection bias further. Second, like almost all previous studies, information regarding menstrual and reproductive factors is self-reported. Misclassification is unavoidable and may introduce a biased estimation for the associations between menstrual/reproductive factors and breast cancer. Because our study is a retrospective by design, contrary to prospective studies, the bias may be differential. Third, most controls (95.9%) were recruited from female relatives or friends of cancer patients other than those treated for breast cancer at the Vietnam National Cancer Hospital. Therefore, they may not be a representative sample of Vietnam’s general population. This may be why the family history of cancer among controls was similar to that of cases in our study. This raises a potential concern that the association estimation derived from our research may be somewhat underestimated or overestimated.
Conclusion
In summary, in this first large case-control study investigating breast cancer risk factors by tumor subtype in Vietnam, we found that menstrual and reproductive factors played an important role in breast cancer etiology, particularly among premenopausal women and for hormonal positive breast cancer subtypes. Therefore, our findings are imperative for developing breast cancer prevention strategies in Vietnam, particularly given the recent changing trends in menstrual and reproductive patterns in the younger generation of Vietnamese women.
Supplemental Material
Supplemental Material - Menstrual and Reproductive Factors in Association With Breast Cancer Risk in Vietnamese Women: A Case-Control Study
Supplemental Material for Menstrual and Reproductive Factors in Association With Breast Cancer Risk in Vietnamese Women: A Case-Control Study by Oanh Thi Bui, Huong Thanh Tran
Abbreviations
body mass index
confidence interval
estrogen receptor
induced abortion
human epidermal growth factor receptor 2
odds ratio
progesterone receptorSAspontaneous abortion
standard deviation
triple-negative breast cancer
Footnotes
Acknowledgments
The authors would like to give special thanks to the participants and the research staff members of this project, without whom this study would not have been possible. We also thank Dr. Mary Shannon Byers and Ms Rachel Mullen for their assistance in editing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NIH/NCI Grant # P20 CA210300 and OISE-19-66185-1 (PIs: Xiao-Ou Shu and Thuan V. Tran). Sang Nguyen was supported by a VECD Global Health Fellowship, funded by the National Cancer Institute (NCI) and the Fogarty International Center (FIC) of the NIH (D43 TW009337) and Ingram Cancer Professorship Fund (to Dr. Shu).
Authors’ Contributions
Conception and design: O. T. Bui, H.TT. Tran, X. O. Shu, Development of methodology: O. T. Bui, X. O. Shu, Acquisition of data (provided animals, acquired and managed patients, provided facilities, etc.): O. T. Bui, H. TT. Tran, S. M. Nguyen, T.V. Dao, Q. V. Bui, A. T. Pham, M. J. Shrubsole, Q. Cai, F. Ye, W. Zheng, H. N. Luu, T. V. Tran, X. O. Shu, Analysis and interpretation of data (e.g., statistical analysis, biostatistics, computational analysis): O. T. Bui, S. M. Nguyen, X. O. Shu, Writing, review, and or revision of the manuscript: O. T. Bui, S. M. Nguyen, H.TT. Tran, X. O. Shu, Administrative, technical, or material support (i.e., reporting or organizing data, constructing databases): O. T. Bui, H. T. T. Tran, S. M. Nguyen, T. V. Dao, Q. V. Bui, A. T. Pham, M. J. Shrubsole, Q. Cai, F. Ye, W. Zheng, H. N. Luu, T. V. Tran, X. O. Shu, Study supervision: H. T. T. Tran, T. V. Tran, X. O. Shu
Ethical Approval
The protocol of this study was approved by the Vietnam National Cancer Institute and Vanderbilt University Medical Center.
Informed Consent
All patients provided written informed consent prior to enrollment in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.