
Abstract
Background
Early testing and treatment is among the successful strategies for the prevention and control of cervical precancerous and invasive cancer, and a paramount for women with HIV. In Ethiopia, visual inspection with acetic acid for screening and cryotherapy treatment is commonly practiced, though the recurrence of the precancerous lesion after treatment has not been well documented.
Objective
This study was aimed to estimate the association of HIV status and the recurrence of cervical precancerous lesion after cryotherapy among Ethiopian women.
Methods
We conducted a retrospective cohort study from January to April 2021. The time to the incidence of recurrence was compared between HIV positive and HIV negative women. Cox regression models were used to adjust the analyses for potential confounders, and only women treated with cryotherapy after a positive Visual Inspection with Acetic acid (VIA) screening test were included.
Results
A total of 140 eligible patient cards were included in the analysis with the median follow-up of 15.5 months. The overall recurrence rate was 15.7% (22/140), with a greater proportion among HIV negative women, 19.0% (4/21) than HIV positive 15.1% (18/119). Prolonged use of corticosteroid and higher age were the major significant predictors of a higher likelihood of recurrence. The recurrence of screening positive lesion was higher among women aged above 39 years (hazard ratio (HR) of 11.94 (95% CI, 1.07-133.04; P = .04), and women with prolonged use of corticosteroid (HR = 7.82, 95% CI = 1.04-58.75; P = .046) than their counterparts.
Conclusion
The recurrence of cervical precancerous lesion after cryotherapy was higher than the expert panel report by WHO with a higher proportion among women of old age and prolonged corticosteroid use. Cryotherapy showed a satisfying performance against the recurrence of cervical disease diagnosed through VIA. To substantiate, our findings, further prospective cohort study is also recommended.
Introduction
Despite comprehensive approach to cervical cancer prevention and control strategy implemented globally, 1 the high morbidity and mortality due to the disease is alarming, predominantly in African countries. 2 Furthermore, despite the theoretical framework from cervical cancer screening and control-these strategies are not often well implemented in low to middle income countries with coverage often being very low. According to the estimate of Global Cancer Observatory 2020 database (GLOBOCAN 2020), the incidence of cancer of the cervix uteri was 604 127, with 341 831 deaths worldwide. Compared with the 2018 estimate (ie, 311 365 women’s deaths) worldwide, the trend of death is increasing, although it is a rare disease in countries with strong screening programs. 3 In Ethiopia, new cases and deaths of cervix uteri were 7445 and 5,338, respectively (GLOBOCAN 2020). The disease (invasive cervical cancer) is caused by the sexually transmitted high-risk human papillomavirus types (HPVs),1,4 with other risk factors, including Human Immunodeficiency virus (HIV), driving infection. 5
The recurrence of cervical precancerous lesion was higher among HIV infected women as compared to women without HIV (18.3% vs 12.3%), 6 though the difference was not statistically significant. The magnitude of relapse among treated patients ranges between 11% to 64%. 7 According to the WHO 2011 report, expert panels strongly recommend cryotherapy over no treatment and the recurrence rate of all cervical intraepithelial neoplasia was reported as 6%. 8
The average age of women with cervical carcinoma recurrence was about 40-45 years and the majority of recurrence occurs within 18-24 months from the time of diagnosis. 9 Expert reviews also indicated that metastatic or recurrent cervical cancer has a survival duration of approximately 12 months. 10
Although the Federal Ministry of Health in Ethiopia has adopted the guideline for cervical cancer prevention and control in 2015, 11 and has been implementing VIA for screening and cryotherapy for treatment, though evidences regarding recurrence of cervical precancerous lesion after treatment and the performance of the methods is lacking. Therefore, this study was aimed to estimate the proportion of women that encountered recurrence of cervical neoplasia after the initiation of treatment and to investigate factors associated with recurrence in order to help in designing of the appropriate patient management strategies in the country.
Materials and Methods
Study Design
We conducted a retrospective cohort study of women with known HIV status who have been screened for cervical precancerous lesion and treated at the same visit with cryotherapy. The reporting of this study conforms to STROBE guidelines. 12
Study Setting and Period
This study was conducted from the 2 centers of excellence, namely Zewditu Memorial Hospital and St Paul’s Hospital, which are public hospitals in Addis Ababa, Ethiopia, from January to April 2021. Addis Ababa is the capital of Ethiopia, and geographically located at the center of Ethiopia, at 9°1′48″N38°44′24″E, with an approximate land area of 526.46 square km. 13 The location of data collection sites was as follows: The Zewditu Memorial Hospital is located in the Kirkos sub-city and St Paul’s Hospital is located in the Gulele sub-city, which are among a total of 11 sub-cities in the Addis Ababa city. 13 The 2 hospitals were selected for the current study based on their client load and high HIV testing, treatment and follow-up services, in addition to their involvement in early initiation of cervical cancer screening with an average of 10 years cervical screening experience. All eligible patient cards that met the specified objective were included as our study subjects.
Sample Size Estimation
The required sample size was estimated using observational study formula initially,
14
considering the HIV positive women as the exposed group and HIV negative women as non-exposed group, though the actual eligible data in the record were less than calculated that allow us to include all the eligible records in the study. As shown in Figure 1, a total of 5860 women were screened using VIA for the average of the 10 year period from 2009 to February 7, 2021. Out of the total screened, about 1636 patient records were excluded initially due to unknown HIV status, appointment date of treatment follow-up, which was beyond our data collection period and lack of information on the register. Of the remaining 4224 patient records, 3052 were HIV positive and 1172 HIV negatives. After checking the VIA positivity result, only 628 cases were identified, which was less than the calculated sample size (n = 1275). Of these, only 321 records were eligible for chart review. Baseline HIV status, cervical screening status and treatment of patients positive for cervical precancerous lesion were the main inclusion criteria for the current study. On the other hand, those client cards with missed information to address the proposed objective, including absence of assessment sheet in the patient card, no clear information about VIA result, first visit VIA result negative in the patient card, patients refused for cryotherapy and not eligible for this treatment, missed patient cards during the time of chart review, were excluded. Flow diagram indicating total VIA screened, and based on their HIV status from selected 2 Government Hospitals of the excellence sites. Finally, the records included in the analysis based on VIA positive status and treatment taken.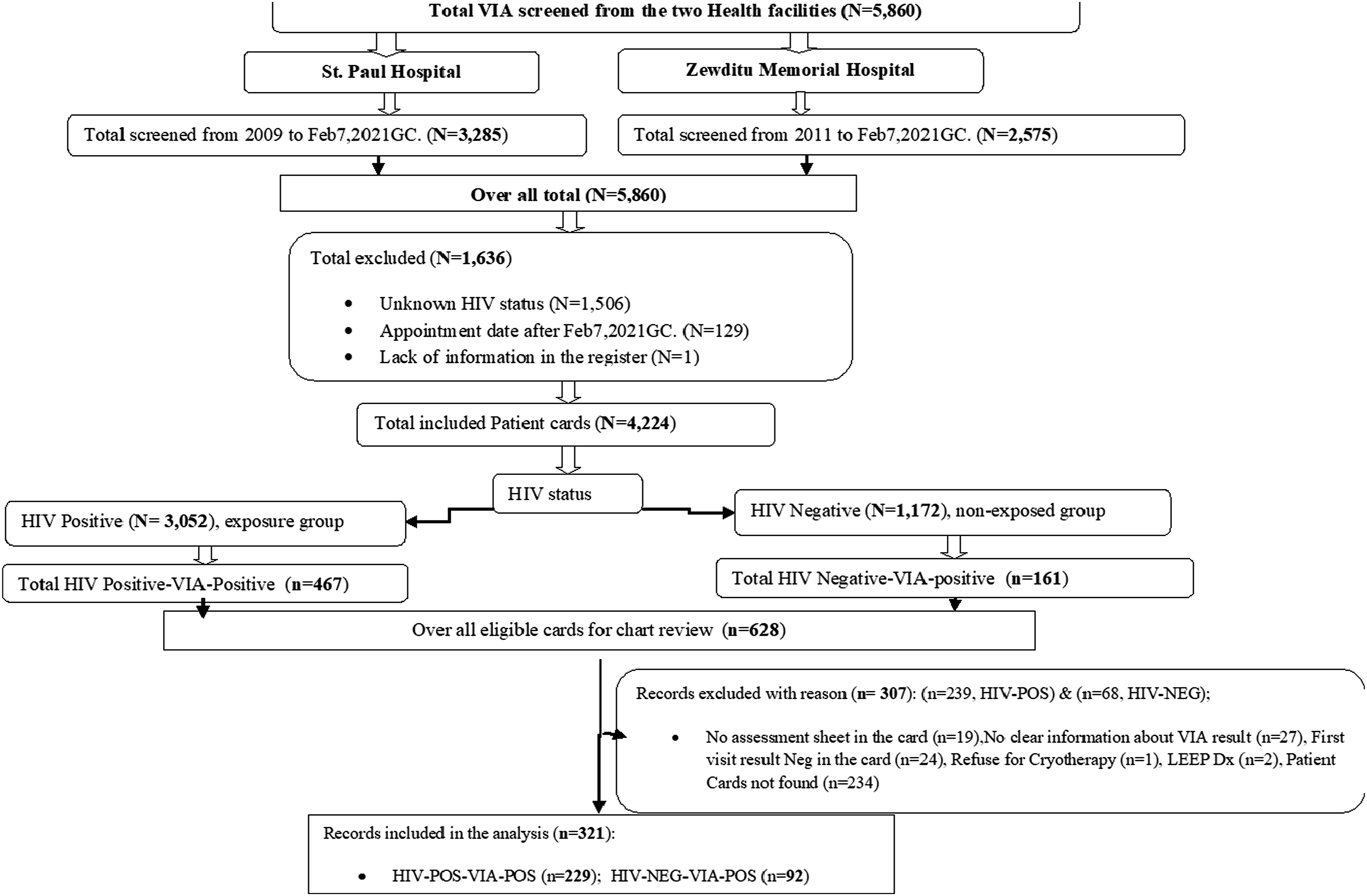
Data Extraction
Chart reviews were conducted by trained health professionals and the principal investigator. Data were extracted from the cervical cancer assessment sheets or history intake forms used in the healthcare facilities. Additional variables of interest (demographic, behavioral and clinical factors), were also extracted to identify the predictors or co-variates of the outcome variable (the recurrence of cervical precancerous lesion).
Data Computerization and Analysis
Data were entered into an excel spreadsheet, exported and analyzed using SPSS version 25. Proportional hazards assumption test (phtest) was checked using STATA version14. Descriptive statistical methods were used to summarize participants’ characteristics of the study. Quantitative variables like the Body Mass Index (BMI) were categorized based on clinical implication. We run Kaplan Meier to estimate a survival distribution and the results were reported using a Log Rank test. The proportional hazard model was used to estimate the effect of HIV status and the other predictor variables on the time to the recurrence of cervical precancerous lesions after treatment using cryotherapy. Hazard ratio with 95% confidence interval was reported as a measure of the strength of association between the target risk factor and the outcome of interest. The independent variables were included in a multivariate analysis provided that P-value was less than .25 in the univariate analysis, and sensitivity analysis was done.
Operational Definition
• Recurrence in this study refers to the relapse or re-infection of women who had treatment for cervical precancerous lesion. • Cryotherapy refers to a procedure, which involves freezing an area of abnormal tissue on the cervix and the tissue gradually disappears and the cervix heals. The procedure is based on the WHO expert panel suggestions to apply double freeze using a 3 minute freeze, 5 minute thaw, 3 minute freeze cycle over single-freeze cryotherapy using carbon dioxide gas. • Survival time refers to the time from a woman’s diagnosis of cervical precancerous lesion and cryotherapy treatment until the time of the recurrence of the lesion. • Corticosteroids are a type of anti-inflammatory drug used to treat rheumatologic diseases, lupus or vasculitis, etc.
Ethical Considerations
Ethical approval for the study was obtained from Addis Ababa University, Aklilu Lemma Institute of Pathobiology, IRB (ALIPB-IRB/35/2013/21) and a further facility-based ethical approval was obtained from the City Government of Addis Ababa Health Bureau (A/A/H/6092/227) and St Paul’s Hospital, Millennium Medical College (SPHHMC-IRB/PW/23/398). The objectives of the study were well explained to all concerned bodies and permission was obtained from selected health facilities to collect data. No consent was taken for this particular study, since we conducted a chart review with no direct patient contact. All information obtained from chart review was kept confidential. Names or personal identifiers were not included in the study, meaning, all the patient details were de-identified. To trace back participant information, medical record number and serial number found in the eligible patient card was used.
Results
In this study, only 61.8% of patient records were eligible for inclusion at baseline/enrolment (denoted as visit 0 in Figure 2). Less than a third of patients (27.9%) returned for their first annual follow-up visit after cryotherapy (denoted as visit 1 in Figure 2). Of those 145 patient records, five records were excluded due to the fact that 3 follow-up results indicated suspicious for cancer, which was beyond cryotherapy treatment, 1 record was with unknown status of the first follow-up and additional 1 due to lack of date of follow-up to calculate months of follow-up. Thus, only 140 records were included in the analysis. Percentage of women who visit Zewditu memorial hospital and St. Paul hospital for screening and treatment of cervical precancerous lesion. On the x-axis, zero indicates those women who were initial screening positive using VIA and treated using cryotherapy, and 5 is the maximum follow-up observed in the study. The y-axis indicated the percentage of each follow-up visit.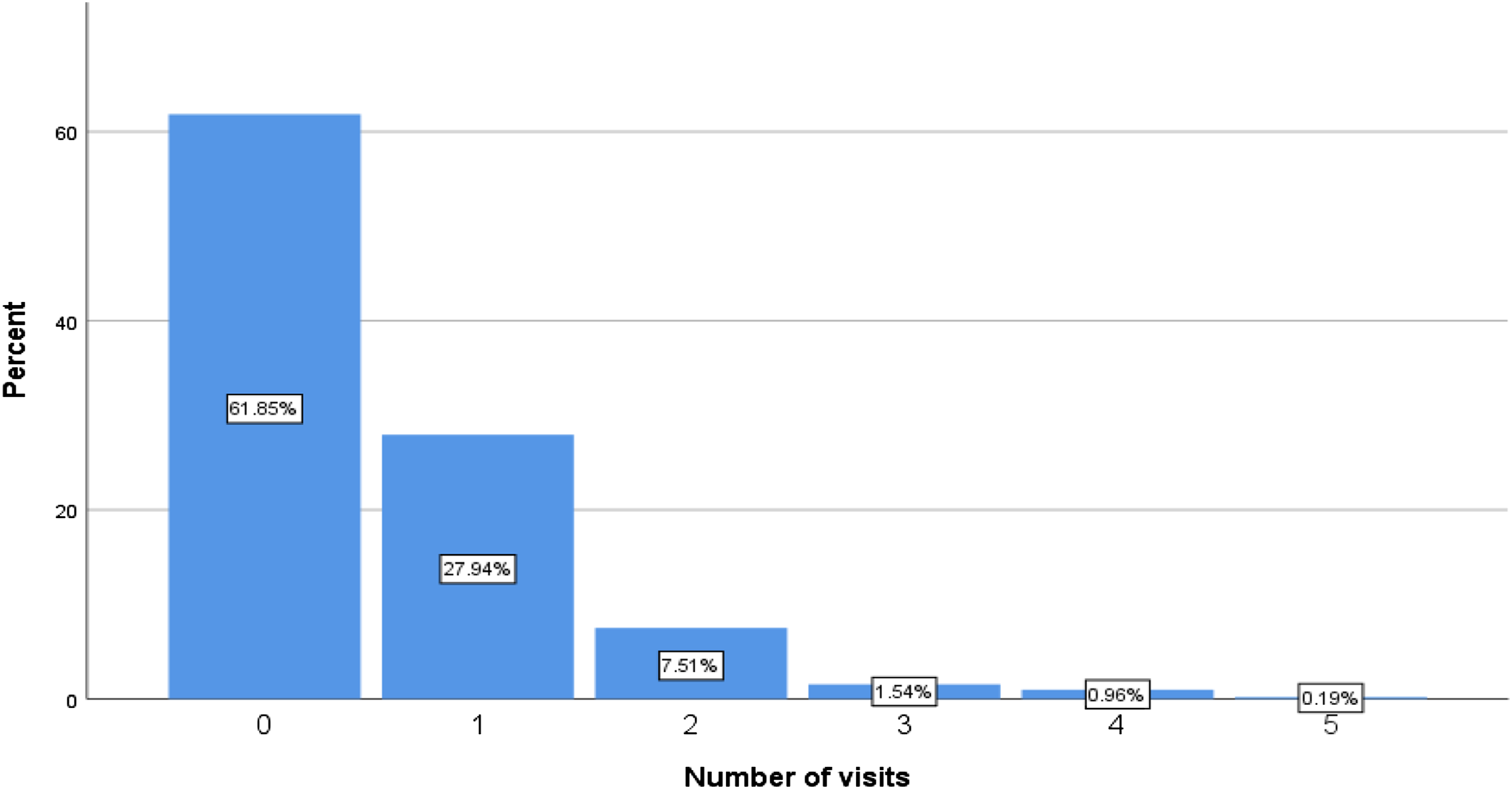
Demographic characteristics of eligible patient records of the earliest cervical cancer screening Hospitals in Addis Ababa, Ethiopia, January to April, 2021.
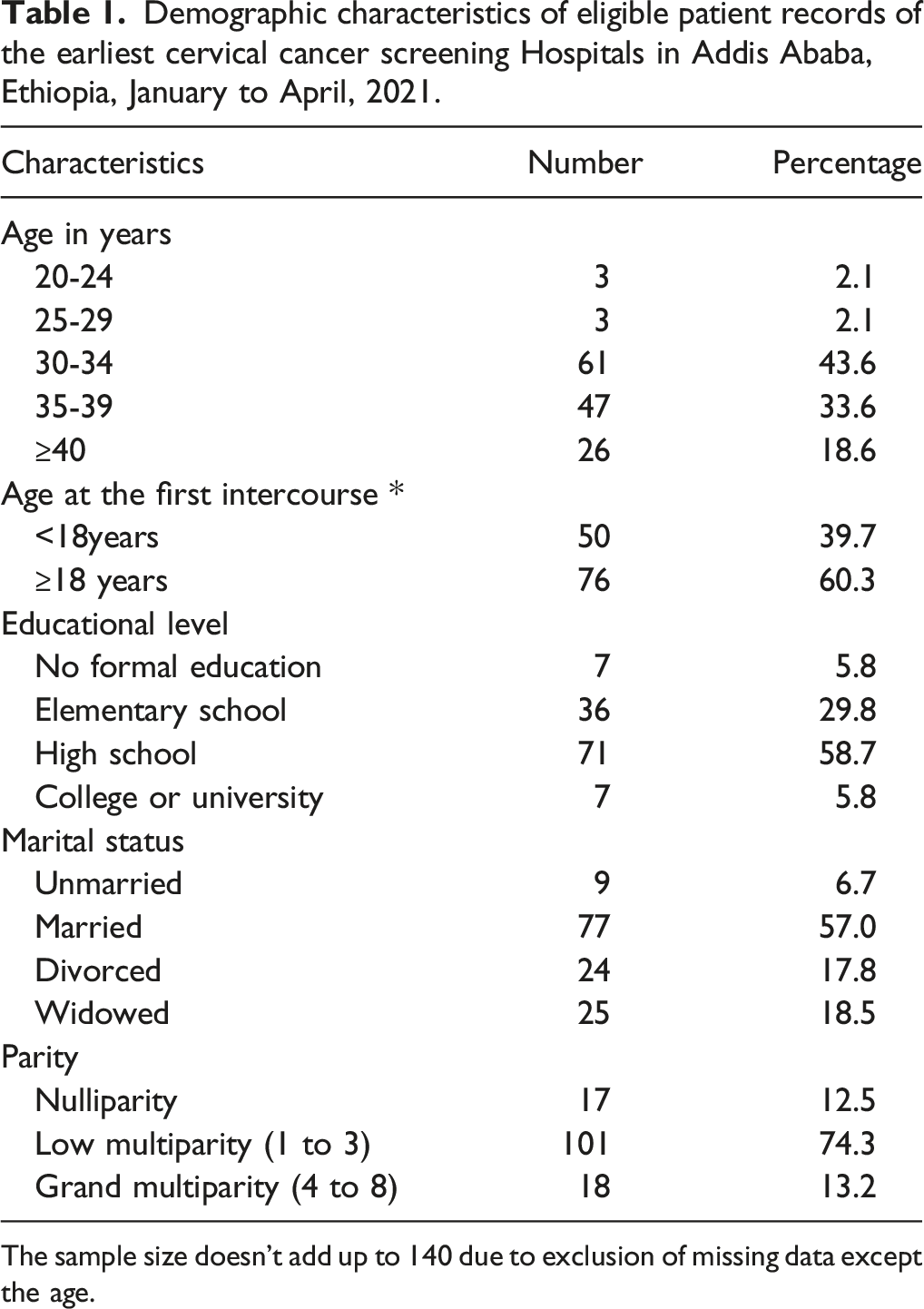
The sample size doesn’t add up to 140 due to exclusion of missing data except the age.
Behavioral and clinical characteristics of eligible patient records of the earliest cervical cancer screening Hospitals in Addis Ababa, Ethiopia, January to April, 2021.
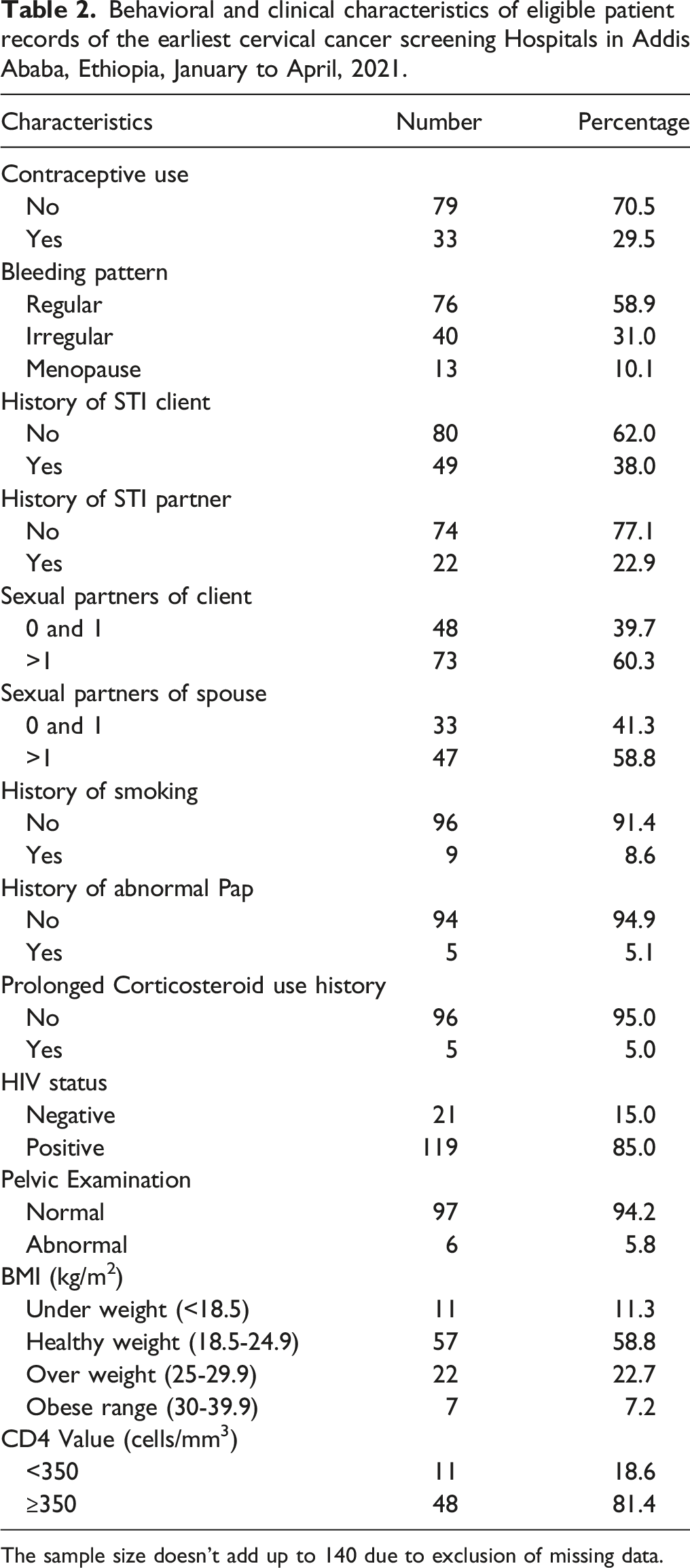
The sample size doesn’t add up to 140 due to exclusion of missing data.
The rate of the recurrence of cervical precancerous lesion after cryotherapy
The rate of the recurrence of cervical precancerous lesion was 15.7% (22/140) with the median follow-up of 15.5 months. Among the total of 22 events observed, 4 events were HIV negative women, which was 19.0% (4/21), and 15.1% (18/119) of the events were HIV positive women. The longest time to the recurrence for HIV negative women was 24 months while for HIV positive women was 72 months [Figure 3(a)]. Overall comparison among HIV positive and negative women was identified using Log Rank (Mantel-Cox) and depicted that there was a significant difference between the 2 observations (Chi-Square = 6.943, DF = 1, and P-value = .008). The survival estimate using the age category, the highest survival was seen in the age category 30-34 years, indicating 72 months, followed by greater than 39 years of age that the last event happened in 59 months and 35-39 years of age in which last event observed at 46 months of follow-up [Figure 3(b)]. The test of equality of survival distribution for the different levels of age category or overall comparison couldn’t indicate a significant difference (Chi-Square = 4.092, DF = 4; P-value = .39). (a) Kaplan-Meier survival estimate of the recurrences of HIV positive and negative women after cryotherapy treatment for cervical precancerous lesion. (b) Kaplan-Meier survival estimate of the recurrences based on age category. In both scenarios, the horizontal axis represents the time of follow-up in months starting from enrolment while the vertical lines correspond to censoring.
Predictors of the recurrence of cervical precancerous lesion after cryotherapy
Univariate and multivariate hazard ratio of women screened for cervical cancer in excellence sites of Addis Ababa, Ethiopia, January to April, 2021.

One indicates the reference category, HR = hazard ratio.
Discussion
It was evident that post-treatment follow-up of cervical precancerous lesion recommended at 12 months to ensure treatment efficacy.15,16 We estimated the recurrence rate of cervical precancerous lesion among HIV positive and negative women in Ethiopia who were screened using VIA and treated by using cryotherapy. The key findings include: the survival analysis or time-to-event of the recurrence of cervical precancerous lesion after cryotherapy indicated 15.7% with median follow-up of 15.5 months. The highest time to recurrence was seen among HIV positive women and age category of 30-34 years (72 months each). The age greater than 39 years, Corticosteroid use and abnormal pelvic examination were found to be consistent significant predictors for the recurrence of cervical precancerous lesion.
Our study finding was higher than the 5-year recurrence rate reported for the Danish women, 17 and 4.5 years, median follow-up of women in Thailand, 18 which were 6.4%, and 10.3%, respectively. Compared with the previous expert review report on the recurrence rates of cervical intraepithelial neoplasia (CIN) based on evidence generated from observational studies that have used cryotherapy (6%), 8 our finding varied markedly. The difference might be due to the recurrence of the previous studies reported based on the International Federation of Gynaecology and Obstetrics (FIGO) stage, and the treatment modality was not purely cryotherapy,17,18 and CIN category. 8 In addition, we used women with HIV as an exposed group and pure cryotherapy treatment, which was different from the previous aforementioned studies. Meaning, the characteristics of the study population, including the widespread availability of health care, and cancer screening, in these countries might induce the observed difference. On the other hand, a study conducted among Nigerian women reported recurrence of 16.4%, 6 which was somewhat closer to our finding (15.7%) though the treatment modalities employed in Nigeria was thermo-coagulation as opposed to our study which used cryotherapy. A higher proportion of the recurrence was reported among HIV positive women than HIV negatives in the previous study, 6 though not statistically significant. Surprisingly, the proportion of the recurrence was higher among HIV-negative women compared with HIV-positives in our current study, although the loss-to-follow-up was high and the number of the study subjects was less among HIV-negative women to further interpret our finding. This might be due to the fact that HIV positive women are coming into the clinic frequently, and used health care services.
According to the 2016 State-of-the-Art Treatment and Novel Agents in Local and Distant Recurrences of Cervical Cancer report, recurrence was described as being diagnosed within 2 years of initial treatment, 19 and the percentage of pelvic recurrences fluctuates from 10 to 74%, 9 which was inclusive of the current finding. The recurrence of Cervical Intraepithelial Neoplasia following treatment occurs in at least 15% of cases even with the most effective excision and ablative treatment modalities. 6 In addition, prospective cohort study in Western Kenya indicated that the recurrence of at least 1 follow-up visit after the loop electrosurgical excision procedure (LEEP) was 13.0%, 20 somewhat closer to our study finding. A single institutional experience also indicated that the relapse of locally advanced cervical cancer after radio-chemotherapy was 23.0%. 21 A review paper depicted that, the pooled prevalence of treatment failure to treat cervical lesions was 21.4% among women with HIV, and the prevalence of treatment failure using cryotherapy was 13.9%, which was closer to our current finding (15.7%). 22
In this study, age greater or equal to 40 years was a significant predictor of the recurrence of the cervical precancer and our finding was similar to the study report of Peiretti et al, 9 who reported the average age of the recurrence of cervical carcinoma is about 40-45 years. Low CD4 value mainly below 200 cells/mm3 was another significant predictor in the previous studies,6,20 though this was not the case in the current study. Although smoking caused invasive cervical cancer and precancer, 23 the recurrence of cervical precancerous lesion due to smoking was not observed in our study. Our study indicated the lack of a significant difference between the recurrence of cervical precancerous lesion and contraceptive use, which was in concordance with a study that reported no association between cervical neoplasia and hormonal contraceptive use for birth control. 24
Even though various anticipated predictor variables for the recurrence were assessed in the present study only age greater 39 years, prolonged Corticosteroid use and abnormal pelvic examination were the major significant predictors of clinical importance. The implication of this finding might be due to the persistence of the infection and lesion residual at the old age of women, 25 which means, older age was an independent predictor of the persistence and/or the recurrence. 26 Patients with prolonged corticosteroid use developed cervical abnormalities, mainly due to decreased immune surveillance for tumor cells. 27 The recurrence events occurred in the pelvic cavity. 28
Strength and Limitation of the Study
To the best of our knowledge, such kind of the study was not reported in Ethiopia yet. This study assessed average of 10 years screening and follow-up data and looked for the recurrence of cervical precancerous lesion after treatment, making it relevant to inform clinicians and care providers to manage their clients through understanding of the efficacy of cryotherapy which was among the strengths of the study. The limitations were, however, unknown HIV status of patients who were positive for cervical precancer screening and treated for cryotherapy in the register. The high loss to follow-up mainly on HIV negative women who were first time screening positive and treated for cryotherapy, and appointed for 1 year to revisit. This high loss to follow-up was a way to include less sample size in the analysis, and might have an impact on external validity of the study result. Missing data and improper documentation of the records were also some of the limitations in the study, which was always a challenge to conduct retrospective studies in such settings where documentation was not optimal.
Conclusion
Our findings indicated that cervical precancerous lesion recurrence after cryotherapy was higher than the expert review report of WHO guideline for use of cryotherapy (WHO 2011) with a higher proportion among HIV-negative women. The recurrence was greater among women of older age, and those who used corticosteroid. The time to recurrence was higher among HIV positive women than HIV negatives, probably due to lack of follow-up among HIV negative women. Further prospective cohort follow-up of women treated using cryotherapy and other treatment modality is recommended. In addition, local health authorities, including hospitals and other stakeholders need to establish a system to trace or manage loss to follow-up otherwise providing first visit treatment had no any guarantee whether the women were cured or not.
Footnotes
Acknowledgments
All the supervisors are duly acknowledged for their suggestion and advice during the research work. The authors extend gratitude to Addis Ababa University, Aklilu Lemma Institute of Pathobiology, City Government of Addis Ababa Health Bureau, and St Paul’s Hospital Millennium Medical College for clearing the study. We extend our thanks to the Federal Ministry of Health (FMOH) in Ethiopia and Ethiopian Public Health Institute for writing a support letter to the responsible bodies including Regional Health Bureaus to conduct the study. The authors also acknowledge Ajanaw Yizengaw at Ethiopian Public Health Institute and Dr Achameleh (MD, GYN/OBS resident at Blacklion Medical School) for data collection and scientific input. Finally, all study participants and data collectors for their invaluable contribution during the study period.
Author contributions
AL designed the study, manage the overall activities from the inception of topic selection to data collection, data cleaning, analysis and writing draft manuscript. TT, JH, GMK, GM critically reviewed the manuscript, intellectual content, and add-up their valuable scientific input for the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was obtained from Addis Ababa University, Aklilu Lemma Institute of Pathobiology, IRB (ALIPB-IRB/35/2013/21) and a further facility based ethical approval was obtained from the City Government of Addis Ababa Health Bureau (A/A/H/6092/227) and St. Paul’s Hospital, Millennium Medical College (SPHHMC-IRB/PW/23/398). The objectives of the study were well explained and permission was obtained from selected health facilities to collect data. No consent was taken for this particular study, since we conducted a chart review with no direct patient contact. All information obtained from chart review was kept confidential. Names or personal identifiers were not included in the study, meaning, all the patient details are de-identified. To trace back participant information, medical record number and serial number found in the eligible patient card was used.
Availability of data and materials
All data collected for this study were analyzed and included in this article, and data are available on reasonable request.