
Abstract
Objectives
The aim of this study was to evaluate the performance of visual inspection with acetic acid compared with Human papillomavirus Deoxyribonucleic acid (HPV DNA) testing among women with HIV in Ethiopia.
Methods
A comparative cross-sectional study was conducted to address the aforementioned objective. Data were collected from January to October 2021, to compare the performance of these two screening modalities. Trained clinicians collected cervical specimens and immediately applied acetic acid for visual inspection. The HPV DNA testing was done using Abbott m2000rt/SP by trained laboratory professionals in accredited laboratories. A total of 578 women with HIV aged 25-49 years were included.
Results
Test positivity was 8.9% using visual inspection with acetic acid (VIA) and 23.3% using HPV DNA test. The sensitivity and specificity of the VIA test were 19.2% and 95.1%, respectively. The strength of agreement between the two screening methods was poor (k = .184). The burden of genetic distribution of high risk HPV16 was 6.1%, and HPV18 was 1.1%. Other high risk HPV types (ie non-HPV 16/18 high risk HPV genotypes) were predominant in this study (18.6%).
Conclusion
The higher positivity result using HPV DNA testing compared with VIA, and low sensitivity of VIA are indicating that the implementation of HPV DNA testing as the primary screening strategy is likely to reduce cervical cancer cases and deaths of women in the country.
Keywords
Introduction
Cervical cancer is a global health problem, 1 showing over a tenfold increase in developing countries than in developed countries. 2 According to GLOBOCAN, 2020, cervical cancer is the second leading cause of women’s cancer next to breast cancer in Ethiopia with 7445 new cases and 5338 deaths per annum. 3 An estimate of 33.7 million female population is at the risk of cervical cancer with age older than 14 years. 4
To avert the high morbidity and mortality of cervical cancer, screening of women using different diagnostic modalities including human papillomavirus (HPV) 5 DNA test is among the important prevention strategies of the disease. Visual inspection with acetic acid (VIA) and HPV detection tests have been recommended to screen women for cervical cancer in low and middle income countries (LMIC). 6 However, previous studies reported poor sensitivity, 7 low specificity, and low positive predictive values, 8 of the VIA test. In Tanzania however low sensitivity and high specificity of the VIA test for the detection of high grade squamous intraepithelial lesion is reported, 9 indicating some inconsistencies. A limited number of studies that have addressed cervical cancer screening using VIA in Ethiopia also reported low test positivity that ranged from 4.7% to 22.1%.10-12
The visual inspection is made, after applying 3-5% acetic acid to the uterine cervix. If an abnormal load of cellular proteins is present in the cervical epithelium, the acetic acid coagulates the proteins conferring an opaque and white aspect of the concerned area. 13
Recently, the Human papillomavirus Deoxyribonucleic acid (HPV DNA) test is reported as having better accuracy than other methods. 14 However, it has been reported to have low specificity compared with cytology. 15 Those women who were screened and positive for HPV were more likely to be positive for VIA. 16 The clinical performance for the detection of disease in a screening population of age greater than or equal to 30 years was reported with an encouraging sensitivity and specificity of HPV DNA testing. 17 Measurement of sensitivity and specificity is important to understand the ability of a test to correctly classify as positive and negative. In addition, positive and negative predictive values are used to estimate the likelihood of a client having a specific disease.
We applied sensitivity and specificity of the VIA as compared to HPV DNA testing in this study. The expert panel recommends screening cervical precancer using HPV test, where the resources are available, affordable, implementable, and sustainable over time. 18 According to the WHO (2013) expert panel, the reductions in cancer and related mortality were greater with the HPV DNA test. The evidence from the expert panel indicated that no study evaluating the diagnostic accuracy of HPV test followed by VIA has been conducted, 18 although, a recent evidence was reported from Kenya. 7
Ethiopia has been working on cervical screening using VIA for more than a decade and a new primary screening modality (HPV DNA) initiated in 2021 to screen women with HIV as a pilot. However, evaluation of the two screening methods and selection of the best performing technique has the potential to be used for mass screening, which is lacking in our setting. Therefore, the aim of this study was to compare the performance of the VIA with HPV DNA testing and indicate the appropriate cervical screening test in Ethiopia.
Materials and Methods
Study Setting and Participants
We used a comparative cross-sectional study design and the study participants were women with HIV in Ethiopia. Six government hospitals in Addis Ababa, Ethiopia, namely, Zewditu Memorial hospital, St. Paul hospital Millennium Medical College, Alert hospital, Yekatit-12 hospital, Menelik hospital, and St. Peter hospital were involved. These hospitals were selected based on the high ART coverage and those that initiated cervical cancer screening using VIA and HPVDNA tests. A total of 578 women with HIV were consecutively enrolled from January to October 2021 including eligible to collect a cervical specimen, and apply acetic acid, and look for the presence of acetowhite lesions. The main eligibility requirements were women with HIV who visit the facility for diagnosis and ART service, and interested to take cervical cancer pre-screening service. In addition, those women with HIV who were volunteering to participate in the study with age of 25 years and older.
Data Collection Procedure and Laboratory Testing
All data were collected by trained clinicians. After counseling, those who agreed and consented to participate in the study were included. The serial number, facility code, medical record number, VIA, and HPV DNA test result with a remark were all entered into a pre-created worksheet. The VIA test was performed right after skilled clinicians collected cervical specimens. Prior to data collection, women with HIV that enrolled in the study were informed the procedural aspects of specimen collection and VIA testing. After a client preparation in a separate room, all the equipments were ensured, including the light source. Examination table was arranged to enable the woman to position herself and clinicians insert a speculum and view the cervix. And then, cervical specimens were collected using the Abbott Cervi-Collect Specimen Collection Kit (4N73-06). After specimen collection for HPV testing, 5% acetic acid was applied in the cervix and waited for 1 minute for the acetic acid to be absorbed. The entire transformation zone for any raised and thickened white plaques or acetowhite lesions was checked. The VIA results were reported as negative, positive, or suspicious for cancer. The VIA results were submitted immediately into an open data kit (ODK Collect v1.29.2), and captured in the worksheet prepared. The woman was appointed for HPV test result for 2 weeks. For this particular evaluation, the combined HPV/VIA test result was used to determine the treatment and to compare the VIA alone. But, the system in the health facility was launched to use HPV testing as primary screening and VIA as a triage.
In each package of the Abbott Cervi-Collect Specimen Collection Kit for HPV testing, one Cervical Brush and one Transport Tube with 2.4 mL Specimen Transport Buffer (guanidine thiocyanate in a Tris buffer) to stabilize DNA till sample preparation were included. Collected samples were transferred to the testing lab. Qualified laboratory personnel used, the Abbott m2000rt/SP, polymerase chain reaction (PCR) technique to conduct laboratory testing. The principal investigator and a technical expert from Abbott provided the training. Aside from site-based supervision, phone calls were made to testing facilities to discuss any issues that arose during testing and to report results.
The molecular testing principles are as follows:
To amplify HPV targets, a primer mix of three forward primers and two reverse primers targeting a conserved late protein (L1 region) is utilized. Fluorescently labeled probes are used to create a signal for high risk (HR) HPV genotypes. Internal Control (IC) amplicons are produced using a primer set that targets an endogenous human beta globin sequence and identified using an IC specific probe. As a sample validity control for cell adequacy, sample extraction, and amplification efficiency, the Abbott RealTime HR HPV assay identifies the endogenous human beta globin sequence. Different fluorophores are used to mark probes for HPV 16, HPV 18, non-HPV 16/18 genotypes (Other HR HPV), and IC, allowing their signals to be distinguished in a single reaction. 17
Quality Assurance
Well-trained professionals were assigned for data collection and laboratory testing and close follow-up of data collection and testing was made by the principal investigator. Missing due to the invisibility of squamous columnar junction to apply VIA was minimized which was not observed during the pre-test. Additionally, improper labeling of specimen handling tubes and confusion in the reporting of the result, mainly in the reporting of ‘other high-risk HPV’ was timely resolved. The laboratory testing was conducted in laboratories that were accredited by the Ethiopian National Accreditation Office (ENAO) (M0030). The external quality control in each run was included to monitor the quality of the test parameter. The internal quality control (IC) which is an endogenous human beta globin sequence monitored the entire PCR process from the extraction to amplification and detection steps. Meaning, IC was used as a sample validity control for cell adequacy, sample extraction, and amplification efficiency.
Statistical Analysis
Collected data were entered into an Excel spreadsheet and exported to SPSS version 25, for analysis. The values for negative results were coded as ‘0’ and the positive test result was coded as ‘1’ for the categorical outcome measure, and summarized in percentage. Sensitivity, specificity, and the agreement between the two techniques were calculated. Strength of agreement as measured using Kappa value is interpreted as poor (<.2), fair (.2-.4), moderate (.4-.6), good (.6-.8), and very good (.8-1.0). 19 For all analyses, P < .05 was an indicator of statistical significance.
Operational Definitions
Precancer or precancerous lesions of the cervix- refers changes to the cervical cells in an area called the transformation zone.
HPV infection- refers a viral infection that causes cervical precancer and if persist it causes cervical cancer.
Test positivity- refers the proportion of a positive test result of the overall tested or screened women with HIV.
ART coverage- refers a number of women with HIV who take service in the health facility.
Sensitivity- refers the ability of a test to correctly generate a positive result (true positive).
Specificity- refers the ability of a test to correctly generate a negative result (true negative).
Visual inspection with acetic acid- refers a naked-eye examination of the uterine cervix after application of 5% acetic acid and interpreting the result at 1 minute, and used to detect precursors of cervical cancer by a professional.
Results
Participant Characteristics
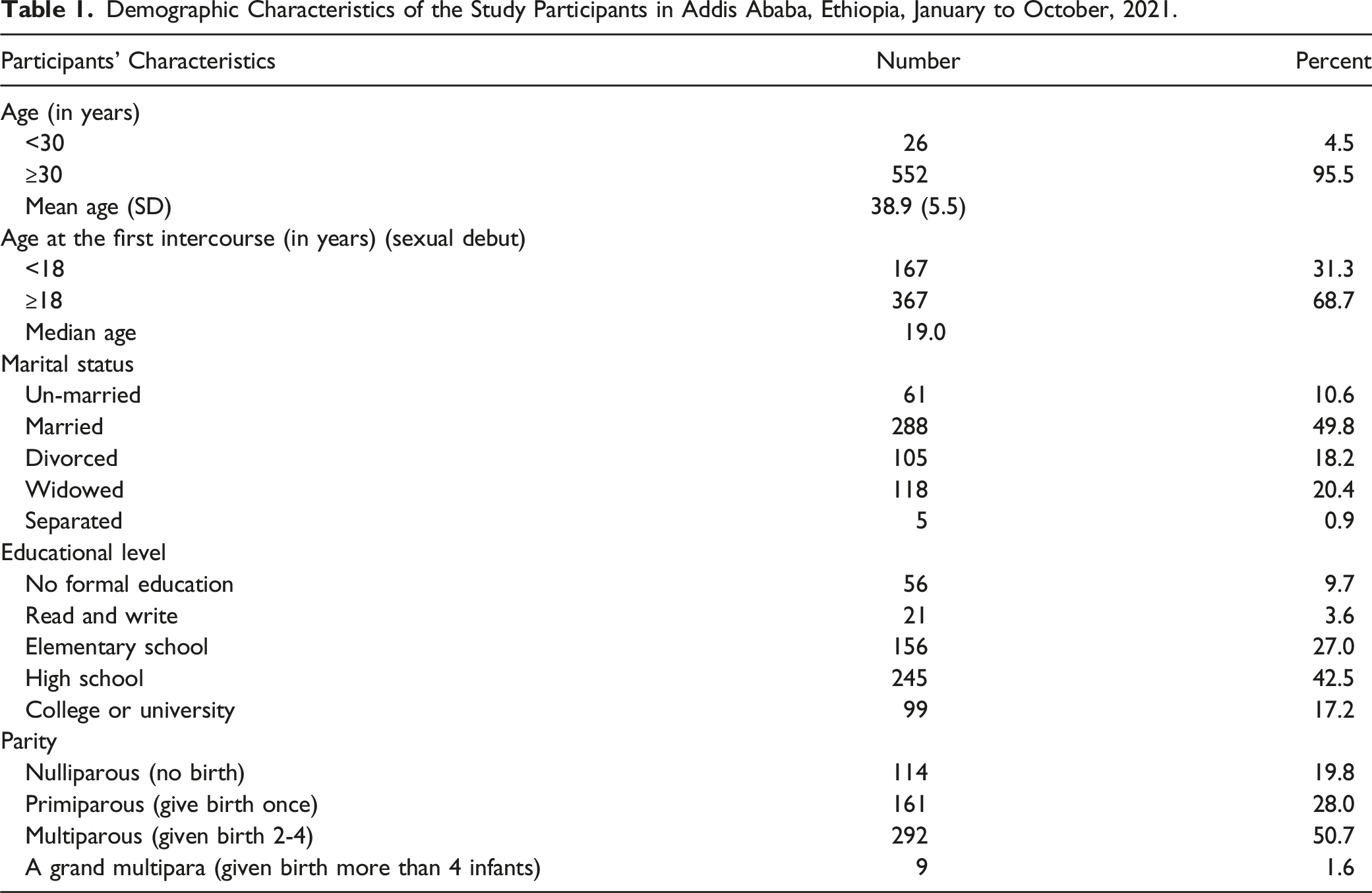
Demographic Characteristics of the Study Participants in Addis Ababa, Ethiopia, January to October, 2021.
Magnitude of Positive Test Results for visual inspection with acetic acid and HPVDNA Testing
Proportion of Positive Test Results for visual inspection with acetic acid and HPVDNA Testing with Age Category Among Women with HIV in Addis Ababa, Ethiopia, January to October, 2021.

The burden of HPV16 was 6.1% (34/558), and HPV18 was 1.1% (6/558). The category of high risk HPV that include 12 HPV types (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68) of the Abbott Multiplex real-time PCR technology was shown in 18.6% (104/558) of women with HIV. About twenty (3.5%) of the samples were not done due to reagent stockout.
The Performance of visual inspection with acetic acid Versus Human papillomavirus Deoxyribonucleic acid Testing for Cervical Screening
Performance Indices of visual inspection with acetic acid as Compared to Human papillomavirus Deoxyribonucleic acid Testing for Cervical Screening Among Women with HIV in Addis Ababa, Ethiopia, January to October, 2021.

Discussion
Simultaneous evaluation of HPV test and VIA is important for adequate generation of evidence. 18 We evaluated the performance of visual inspection with acetic acid as compared to the HPV DNA molecular technique among women with HIV in Ethiopia.
In this study, the test positivity of HR HPV using Abbott real-time PCR technique was 23.3%. A study in Zambia among women with HIV indicated that the test positivity of HR HPV using the Xpert HPV technique was 47.0%, 20 and a study conducted in Burkina Faso and South Africa among women with HIV indicated that 45.1% have a positive careHPV test. 21 Similarly, a study in Tanzania reported 36.4% using CareHPV and 33.8% using hybrid capture-II (HC II) technique. 9 Our finding is lower than previously reported findings in the African continent among similar study populations. The observed difference might be attributed to the difference in the number of the study participants involved in the study, and age of the participants, the molecular technique used, and the study setting. This means, various factors could contribute to HPV infection, like HIV pandemic settings, economic and sociocultural factors, parity, smoking and dietary factors in different settings.22-24 In addition, HPV infection was higher among youth aged under 25 years, probably,22-24 due to transient infection. The analytical sensitivity, target gene amplified, primers and probes for a particular molecular technique might also cause the observed difference in the reported proportions of the HPV test positivity. 25
A study conducted among the general female population in Kenya revealed HR HPV test positivity of 33.0% using HC II. 7 A similar study in Latin America reported the prevalence of HPV (15.4%-18.8%) using HC II. 26 A multi-country study in India, Nicaragua, and Uganda reported positivity rate of cervical careHPV ranging from 2.9% to 20.2%. 27 In China the HPV positive rates using careHPV and HC II were 14.0% and 16.4%, respectively. 28
All HPV infected women do not develop cervical neoplasia and cervical cancer, since persistence of the infection mainly occurred in the immunosuppressed individuals among other contributing factors.22-24
In the current study, the VIA test positivity among women with HIV was 8.9%, which was lower than the previous study in Southern Ethiopia, 22.1%. 12 Similar studies in Zambia and Tanzania depicted that the VIA test positivity was 15.0%, 20 and 10.6%, 9 respectively.
Other studies conducted in Latin America, Asian and African countries, among the general female population reported that the VIA test positivity was 7.1%, 6 9.7%, 8 7.6%, 16 6.6%-16.1%, 26 5.5%-34.4%, 27 6.0%, 28 and 7.0%. 7 Similar studies conducted in Ethiopia among eligible women in the general population also showed varied results. For instance, in Butajira, test positivity of VIA was low (4.7%), 10 and in Jimma, VIA positive result was 12.9%. 11
The VIA positivity was higher among HIV positive women (12.9%) compared with HIV negatives (3.4%). 29
The attributed difference observed in general was due to the difference in the number of the study participants, the study setting, age of the study participants included in the study, and also, the subjectivity of the VIA test results interpretation. Meaning, VIA results were highly variable, 30 through variations of acetowhite areas, 13 and interobserver variability. 31
A study revealed that the sensitivity of VIA ranged from 21.9% to 73.6%, while the specificity is 84.2%. 27 The low sensitivity (31.1%) and high specificity (94.6%) of the VIA test reported by a Tanzanian study, 9 was in agreement with our finding. The low sensitivity of VIA indicated that the test is not suitable for mass-screening program, 28 which is in agreement with our finding of low sensitive VIA result compared with the HPV DNA test. A population based study from Nigeria reported that the VIA test is insensitive compared with cytology and HPV test. 32 The highest test sensitivity and a lower number of visits observed using HPV testing show cost-effectiveness and reduce the lifetime cancer risk by 29.5% than other testing modalities including Pap cytology, 33 although, it requires the high upfront cost of equipment and supplies. 34 The reported strategy,33,34 is in agreement with our finding indicating the higher test positivity of HPV DNA compared to VIA.
The higher positivity of our HPV DNA test compared to VIA suggests that the Ministry of Health and other stakeholders in Ethiopia could consider applying the HPV DNA testing as the primary screening strategy. The test was conducted in a batch of 96 tests in one run, which is important to address screening to a larger population. However, the time to receive the result takes a few days/weeks as observed in the facilities.
The narrative report indicated that few clients who had cervicitis during the time of data collection were treated with antibiotics, and re-appointed for re-screening. Three clients had VIA negative plus polypectomy, and one client had VIA positive plus polypectomy. Three other participants who practiced multiple sexual partnerships were negative for both VIA and HPV DNA testing, suggesting adequate awareness about the prevention methods of sexually transmitted infections.
The limitation of this study was that no further colposcopy triage was applied, which is better than VIA triage as indicated by WHO experts’ recommendation, 18 and cytological findings used as the reference standard for the evaluation of the performance of available diagnostic modalities. In addition, confirmation of the HPV result with actual cervical lesion or graded CIN was not done.
Conclusion
Our finding had shown low sensitivity of VIA as a cervical screening method. The test positivity of VIA is low compared with HPV DNA, and there was poor agreement between the VIA and HPV DNA tests. Thus, the implementation of HPV DNA testing as the primary screening strategy is likely to reduce cervical cancer cases and deaths of women in Ethiopia and to meet the 2030 elimination program launched by WHO.
Footnotes
Acknowledgments
All my advisors are duly acknowledged for their suggestions and advice during the research work. The authors extend gratitude to the Ministry of Science and Higher Education (MoSHE), National Research Ethics (NRERC), Aklilu Lemma Institute of Pathobiology, City Government of Addis Ababa Health Bureau, Yekatit 12 Hospital Medical College, and St. Paul’s Hospital Millennium Medical College, and EPHI-IRB for clearing the study. We extend our thanks to the Federal Ministry of Health (FMOH) in Ethiopia and the Ethiopian Public Health Institute for writing a support letter to the responsible bodies including Health Bureaus to conduct the study. Kidist Alemayehu, Million Hailu, and Girma Zemedu acknowledged for their support in open data kit template design and data collection training facilitation. Finally, we also thank all study participants and data collectors for their invaluable contribution during the study period.
Authors’ contributions
Agajie Likie Bogale: Made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content. Tilahun Teklehaymanot, Getnet Mitike Kassie, Girmay Medhin, Jemal Haidar Ali, Nega Berhe Belay: Made substantial contributions to the conception and design, acquisition of data; took part in reviewing and editing of the final manuscript. All authors have read, critically revised, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Seed money was obtained from Addis Ababa University and the Ethiopian Public Health Institute for data collection.
Abbreviations
ART, Antiretroviral therapy; CIN, Cervical intraneoplasia; DNA, Deoxyribonucleic acid; ENAO Ethiopian national accreditation Office; HIV, Human Immunodeficiency virus; HPV, Human papillomavirus; HR, High risk; IC, Internal control; k, kappa value; PCR, Polymerase chain reaction; rt, real-time; SP, Sample preparation; VIA, visual inspection with acetic acid.
Ethics statement
Ethical clearance was obtained from the National Research Ethics (NRERC) (MoSHE/04/246/832/21), Aklilu Lemma Institute of Pathobiology (ALIPB-IRB/35/2013/21), and Ethiopian Public Health Institute (EPHI-IRB-118-2018). Furthermore, a facility-based approval letter was obtained from the City Government of Addis Ababa Health Bureau (A/A/H/6092/227), St. Paul Hospital, Millennium Medical College (SPHHMC-IRB/PW/23/398), and Yekatit 12 Hospital Medical College (07/21). The objectives of the study were explained and permissions were obtained from the selected health facilities to collect data. Those volunteer women to participate had signed consent and were involved in the study. All information obtained from the study participants was kept confidential, names or personal identifiers were not included in the study. A medical record number was captured to trace back a patient card when needed.
Availability of Data and Materials
All data generated or analyzed are included in this article, and data are available on reasonable request.