
Abstract
Background
Cervical cancer and human immunodeficiency virus prevention are public health priorities in Ethiopia. Despite cervical cancer being preventable with the Human Papilloma Virus vaccine and cervical cancer screening, HIV-infected women still have a low rate of screening, and data are scarce in this country. Thus, this study aimed to assess the prevalence of cervical cancer screening service utilization and associated factors among HIV-positive women in Southern Tigray, Ethiopia, 2018.
Methods
A facility-based cross-sectional study was performed from March 1st to May 15th, 2018. We recruited 465 HIV-positive women using a systematic random sampling method. Data were collected using a pre-tested structured interviewer-administered questionnaire. Descriptive statistics, followed by multivariable logistic regression analysis were performed. Crude odds ratios, adjusted odds ratios, and 95% confidence intervals (CIs) were reported.
Results
In this study, only 8% of HIV-positive women were screened for cervical cancer. The most frequently cited barrier by participants to getting screened was feeling healthy 282 (65.9%). Multiparity {AOR = 4.12, 95% CI = (1.70, 9.95)}, provider recommendation to get screened {AOR = 3.20, 95%CI = (1.34, 7.65)}, having good knowledge {AOR = 4.33, 95%CI = (1.66-11.29)}, and high perceived susceptibility for cervical cancer {AOR = 3.10, 95% CI = (1.31-7.33)} were the factors significantly associated with cervical cancer screening service utilization.
Conclusions
The prevalence of cervical cancer screening service utilization was quite low. Provider’s recommendation to get screened, multiparity, knowledge, and perceived susceptibility were factors strongly associated with the service utilization. There is a need of routine counseling of health care providers for all HIV-positive women to get screened. Women’s lack of knowledge also needs to be addressed by informing every HIV-positive woman that they are more susceptible to cervical cancer, and that screening is critical to fighting against the disease.
Introduction
Globally, 570 000 women developed cervical cancer (CC) and 311 365 women have died from the disease, making it the fourth most common cancer for both incidence and mortality among women aged 15-44 years in 2018. However, about 80% of the cases and 87% of the deaths occurred in low-to-middle income countries.1,2 In these countries, CC was the second most prevalent and leading cause of cancer death.3,4 The highest incidence of CC was documented in Sub Saharan Africa (SSA) at 34.9 per 100 000 women, 5 and the disease is responsible for 21.7% of all cancer deaths among women in these continents. 6 Each year, 7095 Ethiopian women are diagnosed with CC, and 4732 die from the disease.6,7
Several studies found that human immunodeficiency virus (HIV) -positive women have a higher burden of CC incidence and mortality than the general population.8,9 Immunosuppression and low CD4 count induced by HIV infection predispose HIV-infected women to CC and the development of squamous intraepithelial lesions.10,11 Moreover, HIV is associated with several enabling factors for CC, such as multiple sexual partners, early sexual debut, financial status, and smoking.11,12 This association between HIV and CC could be more relevant in developing countries, where access to highly active antiretroviral therapy and other services are still existing challenges. 13 CC is eight times more common in women living with HIV in this country, and the death rate is 2-fold higher.14,15
Cervical cancer screening programs have an important role in the prevention of CC. The massive decline in CC mortality in developed nations is attributed to widespread screening, but CC in developing nations continues to be the leading female malignancy because cervical cancer screening (CCS) is rare. 16 Ethiopia has adopted cheaper but effective techniques for screening of CC called visual inspection with acetate (VIA) 17 and the federal ministry of health targeted to achieve at least 80% coverage of CCS and treatment among target populations (all women aged 30-49 years) by 2020. 18 However, a nationwide Community-based cross-sectional survey conducted in Ethiopia in 2015 shows an extremely low rate of cervical screening (2.9%). 19 Even though, over 534 000 women were living with HIV in Ethiopia, 9 only 15 263 of this risky population get screened for CC in the whole country between 2010 and 2013. 20 Some recent small-scale studies done in Ethiopia, Gondar, 21 Addis Ababa21,22 among HIV-positive women also reported low rate of screening service utilization (23.5%), (10.8%), and (11.0%), respectively.21-23
According to the study done in Gondar, Southwest Ethiopia in 2017, variables such as age, perceived susceptibility, and knowledge of CC had a strong association with CCS service utilization. 23 A study carried out in 2016 in Addis Ababa, unveiled that the most prevalent barriers to getting screened were a lack of knowledge about CC and CCS, perceived pain during the procedure, and financial constraints. 22 Another study done in Addis Ababa, Ethiopia on HIV-positive patients’ acceptance of CCS revealed that higher educational status, getting information about CC from health professionals, and having awareness of the test were significantly associated with higher acceptance of screening. 21
To date, only a few studies assessed CCS service utilization and associated factors in Ethiopia, where the prevalence of CC and HIV are high.7,24 To the best of our knowledge, despite having started CCS services, evidence on the utilization of the service and associated factors among HIV-positive women are unknown in the entire Tigray region, much alone the research area, since analogous studies have not been done on these vulnerable groups. Further information on HIV-positive women regarding the prevalence of CCS utilization and associated factors is needed for effective program implementation, which aims to reduce the incidence and mortality of the disease. Thus, this study aimed to assess CCS service utilization and associated factors among HIV-positive women in Southern Tigray, Ethiopia.
Materials and Methods
Study Area and Setting
A facility-based cross-sectional study was conducted from March 1st to May 15th, 2018, in public health facilities located in the southern zone of the Tigray region, Southern Ethiopia. Functional health facilities in this zone comprised three general and two primary hospitals, 35 medium- and lower-level private clinics, 27 health centers, and 67 health posts. Only Maichew Generalized Hospital, Korem Generalized Hospital, and Alamata Generalized Hospital provide both CCS and anti-retroviral therapy (ART) services in this zone. The overall prevalence of HIV-AIDS is 2.2%, and there are more than 18 000 women population living with HIV in Southern Tigray. However, only 10 574 (58.7%) HIV-positive women are medically treated in these facilities according to the information gained from respective facility heads.
Population
The study population was comprised of HIV-positive women aged 25 years and older 25 who were patients of adult HIV clinics at public health facilities that provide CCS in Southern Tigray for at least 6 months. Women who were critically ill and mentally disabled during the data collection period were excluded from the study. Women who had their uterus removed for a variety of reasons were also excluded from the study since they were not at risk of cervical cancer.
Measurement Variables
Outcome Variable
Predictor Variables
Wealth index: The wealth index of participants was produced from the existing variables (household assets ownership, household characteristics, and access to utilities) from the data set through factor analysis using Principal Component Analysis, and participants were assigned into three groups namely: low, medium, and high wealth index.
Knowledge of cervical cancer: Total knowledge of cervical cancer was assessed using a 5- point knowledge score. A total of 10 questions were used to assess the knowledge of participants; correct answers were scored 1 while incorrect answers were scored 0. Then, women with a summary score of greater than or equal to 5 were categorized as having “good knowledge” and those with a score less than 5 were categorized as having “poor knowledge”. 22
Perceived susceptibility: Participants who scored more than or equal to a median of 5 from a total of 5 questions regarding susceptibility to cervical cancer were considered as having “high perceived susceptibility” and those who scored less than 5 were considered as having” low perceived susceptibility”.
Perceived severity: Participants who scored more than or equal to a mean of 5 from a total of 5 questions regarding the severity of cervical cancer were considered as having “high perceived severity” and those who scored less than 5 were considered as having” low perceived severity”.
Perceived benefit: Participants who scored more than or equal to a mean of 4 from a total of 4 questions regarding the benefit of cervical cancer were considered as having “high perceived benefit” and those who scored less than 4 were considered as having” low perceived benefit”.
Perceived barriers: Participants who scored more than or equal to a mean of 10 from a total of 10 questions regarding barriers to cervical cancer were considered as having “high perceived barriers” and those who scored less than 10 were considered as having” low perceived barriers”.
Sample Size and Sampling Procedure
To determine the sample size, a single population proportion formula using Epi Info version 7.2.0.1 was used with the following assumptions: 23.5%,4,23 the prevalence of cervical cancer screening service utilization among HIV-positive women, a margin of error of 4%, and a 95% confidence interval. For possible nonresponse, 10% was added and the final sample size was 475. Of all public health facilities in the southern zone of Tigray, facilities that provide both CCS and ART services (Maichew Generalized Hospital, Alamata Generalized Hospital, and Korem Generalized Hospital) were included. 17 Samples were proportionally allocated to the estimated patient flow during the study period of each selected hospital.
For every woman attending the HIV clinic for a routine follow-up visit, eligibility criteria were checked at the entrance desk and a sequential number was given to each eligible participant according to the arrival order. Using a systematic random sampling technique, every third eligible woman on the list of their order of arrival was selected to participate in this study. This procedure was repeated every day in each HIV clinic and a tag was attached to the cards of participants to prevent repeated enrollments of the same participant.
Source of Data and Data Collection Methods
A structured questionnaire
Data Quality Control
The tool was reviewed by two senior experts and pre-tested on 5% of the sample size, before administration. All required revisions were made to the study tool based on the experts' comments and the pretest. Experienced enumerators ie, six BSc nurses and two MSc nurses were recruited for data collection and supervision. Three-day intensive training on the aim of the study and sampling procedures was provided to the enumerators. An overview of the study and random selection were explained to eligible women and data was collected in a private setting after addressing all doubts and concerns. Supervisors conducted routine checkups on completed questionnaires for completeness and scientific soundness. Additionally, the principal investigator checked the filled questionnaire and provided feedback to the supervisors daily. Before commencing the data analysis, appropriate transformations were made to the variables.
Data Processing and Analysis
The data were entered into Epi-data version 3.1.1 and then transferred to SPSS version 25 for analysis. Frequency and percentage distribution were used to describe the characteristics of the overall sample respondents across a set of background characteristics. Bivariable and multivariable logistic regression analyses were also performed. Simple summary statistics (percentage of the outcome variables) were obtained for each category of the explanatory variables to examine the unadjusted but statistically significant relationship between the dependent variable and explanatory variables. The statistical significance was tested by a Pearson’s χ2 (chi-square) test. Age was controlled for in the bivariable analysis. After adjusted for age, variables that remained significant with a P-value of less than .05 were retained for further analysis with multivariable logistic regression to control for confounders. Odds ratios and 95% confidence intervals were computed and a P-value of less than .05 was used to determine the cut-off points for statistical significance. The necessary assumption of model fitness during logistic regression was checked using Hosmer -Lemeshow goodness-of-fit test statistics. Multicollinearity was checked by a variable inflation factor and all showed no multicollinearity with a variable inflation factor of less than five.
Results
Socio-Demographic Characteristics of Participants
Socio-demographic Characteristics of HIV-positive Women Aged 25 Years and Above Attending Adult HIV Clinics in Southern Tigray, Ethiopia 2018 (N = 465).

SD = Standard Deviation.
Reproductive and Medical Characteristics of Participants
The mean age ± SD at first sexual intercourse was 17.70 ± 2.98. Of all the study participants 303 (65.2%) claimed that they did not have multiple sexual partners, 319 (68.6%) claimed that their partner or husband did not support them in checking their gynecological health, and 330 (71.0%) claimed to have ever used modern contraceptives. Only 178 (38.3%) participants admitted to having a history of sexually transmitted diseases (STIs).
Reproductive and Medical Characteristics of HIV-positive Women Aged 25 Years and Above Attending Adult HIV Clinics in Southern Tigray, Ethiopia 2018 (N = 465).
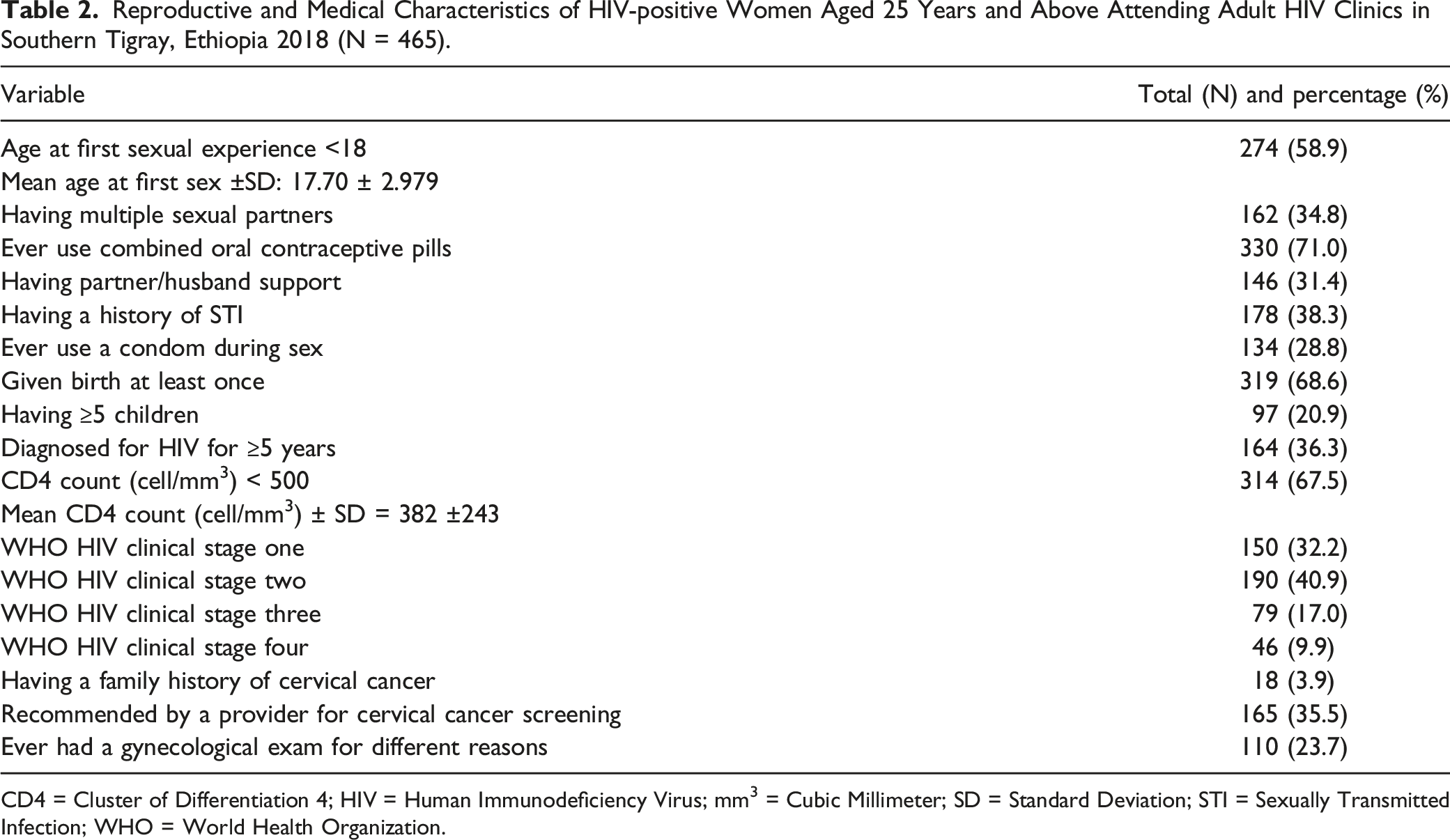
CD4 = Cluster of Differentiation 4; HIV = Human Immunodeficiency Virus; mm3 = Cubic Millimeter; SD = Standard Deviation; STI = Sexually Transmitted Infection; WHO = World Health Organization.
Information and Knowledge Related to CC and CCS Service
Information and Knowledge Related to CC and CCS service among HIV-positive Women Aged 25 Years and Above Attending Adult HIV Clinics in Southern Tigray, Ethiopia 2018 (N = 465).

CC = Cervical Cancer; CCS = Cervical Cancer Screening; HIV = Human Immunodeficiency Virus.
Perceptions and Utilization of CCS
Participants Perception (Constructs of Health Belief Model) and CCS Service Utilization among HIV-positive Women Aged 25 Years and Above Attending Adult HIV Clinics in Southern Tigray, Ethiopia 2018 (N = 465).

CC = Cervical Cancer; CCS = Cervical Cancer Screening.
More than half 265 (57.0%) of women had a high perceived severity of the disease. In this study, merely 37 (8.0%) HIV-positive women were screened within the last 5 years preceding the survey. Concerning reasons cited by participants for not being screened, the perception of being healthy was mentioned by a significant number of women (282) followed by embarrassment (200) (Figure 1 jpg). Reasons cited by participants for not being screened among HIV-positive women aged 25 years and above attending adult HIV Clinics in Southern Tigray, Ethiopia 2018 (N = 428).
Percentage Variation in the Prevalence of CCS Service Utilization
Regarding the CCS service utilization percentage variation across a set of some selected variables in Table 4, participants who fell within the age range of (25-34) and (35-44) were more likely to utilize CCS service (11.0%) and (6.9%), respectively than those who found in their age of ≥45 years (4.3%). Participants who belonged to the high wealth index group were more likely to utilize CCS service (16.6%) than those who belonged to the low wealth index group (3.8%). However, participants who belonged to the medium wealth index group were less likely to utilize the service (3.3%) compared to those who belonged to the low wealth index group (3.8%).
Prevalence of Cervical Cancer Screening Service Utilization, Stratified by Selected Participant’s Characteristics and Unadjusted but Significant Association of Dependent and Explanatory Variables.

*P-value: Indicated the unadjusted but statistically significant relationship between the dependent variable and explanatory variables (not adjusted for age) obtained after being tested by the χ2 (chi-square) test.
Factors Associated With CCS Service Utilization
Results of Age-Adjusted Logistic Regression Analysis on Factors Associated with CCS Service Utilization (N = 465).
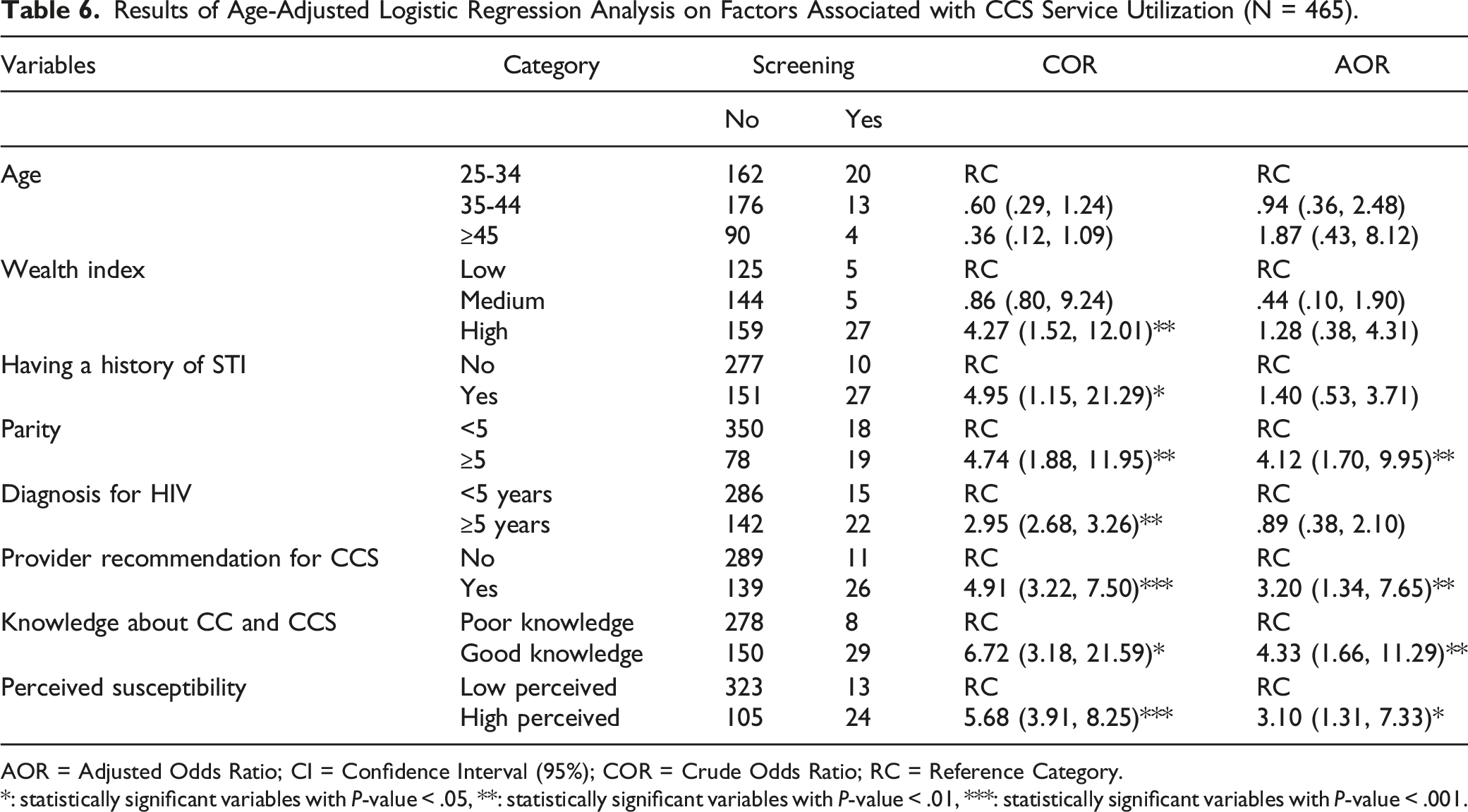
AOR = Adjusted Odds Ratio; CI = Confidence Interval (95%); COR = Crude Odds Ratio; RC = Reference Category.
*: statistically significant variables with P-value < .05, **: statistically significant variables with P-value < .01, ***: statistically significant variables with P-value < .001.
Discussion
This study aimed to assess the prevalence of cervical cancer screening service utilization and associated factors among HIV-positive women aged 25 years and above attending adult HIV clinics in Southern Tigray, Ethiopia. The prevalence of CCS service utilization was quite low (8.0%). Multiparity, provider recommendation for cervical cancer screening, having good knowledge about CC and CCS, and having high perceived susceptibility for CC were factors associated with CCS service utilization,
In this study, only 37 (8%) of HIV-positive women reported a history of CCS in the last 5 years. This finding was lower than that of previous studies carried out among HIV-positive women in Ethiopia: Gondar (23.5%), 23 Addis Ababa (11.5%), 22 and Addis Ababa (10.8). 21 This variation can be explained by the differences in the level of knowledge of study participants about CC and CCS. It may also be due to the weak integration of ART follow-up care with CCS services. This figure was also much lower than the findings from the study conducted in Spain among 479 HIV-positive women (50.6%), 29 the study carried out in England among 209 low-income women living with HIV (85.7%), 30 a mixed study conducted in Kenya among 378 HIV-positive women (46%). 31 The possible reason for this variation could be due to the variations in the universal access to the health service as well as the countries’ promotional policy variations. Kenya, for example, has a more robust CCS program with other prevention services as well as ongoing provision of health education about cervical cancer and screening services. 32
Furthermore, the prevalence of CCS service utilization in the current study is also lower than in prior studies among the general women population conducted in different locations in Ethiopia, such as Dessie (11.0%), 26 Mekelle (19.8%), 27 and Jimma (15.5%). 33 This could be explained by the fact that as the previous studies were done in large cities, with individuals more likely to be urban and have more access to media and other information that can enable them to utilize the service. On the other hand, the finding from the current study is higher than the previous studies conducted among married women in Arbaminch among married women (5.9%) 29 and Dire Dawa among all women aged 30-49 (4.0%). 34 This might be because of the integration of ART to CCS service, which has a potential to enhance the utilization among HIV-positive women.
The perception of being healthy due to the absence of symptoms was the most frequently cited barrier to getting screened by the study participants 282 (65.9%). The same result was also reported in the studies conducted in Gondar 23 and Addis Ababa, 21 which revealed that the absence of symptoms/discomfort” was among the main reasons mentioned by participants for not utilizing the service. This could be explained by the fact that most people seek health care services while they feel unhealthy, especially in developing countries.
In this study, the odds of cervical cancer screening among women with good knowledge were 4.3 times higher than those who had poor knowledge. Consistent findings were also reported in a study conducted in Gondar 23 and Addis Ababa.21,22 There is, therefore, a need to increase awareness about cervical cancer and the need of being screened as a measure to prevent cervical cancer.
Recommendation/consultation from health professionals was a strong predictor of CCS uptake. Women who have been recommended by health care providers were more likely to be screened when compared with those who had not been recommended. This finding is in line with studies conducted in Kenya 31 and Uganda. 35 This might be attributed to the consultation/recommendation from health care providers increasing awareness about CC and the importance of screening services.
Participants who have high perceived susceptibility to develop CC were 3.10 times more likely to utilize CCS service as compared to their counterparts. The results of the current study are in line with previous studies conducted in Gondar, 23 Mekelle, 27 and Uganda. 36 This might be attributed to the assumption of the behavioral model theory, which assumes that individuals who admit a high risk that they will be personally affected by a particular health problem are more likely to engage in behaviors to decrease their risk of developing the condition. 37
Furthermore, women with five or more children were nearly four times more likely to be screened than women with less than five children. This finding was similar to that of a previous study conducted in Arbaminch. 28 This could be because women who had many children might visit health care facilities more frequently in addition to their routine HIV care follow-up than those with few children. As a result, they might have the opportunity to get information and advice to use the screening service from health professionals.
Strength and Limitation of the Study
The health belief model was utilized in this study to examine the behaviors of participants. Another aspect of the study is that it is controlled for potential confounders. The limitation of this study is the difficulty in interpreting the findings from a cause-and-effect relationship, as the study was cross-sectional. The recall period of screening service utilization of up to 5 years may increase recall bias in this study, and participants may have inflated or underestimated their screening prevalence Since the study is facility-based, it may not represent all women not visited health institutions during the study period. Despite training being given for data collectors and the purpose of the study being discussed with participants, the study may still be liable to social desirability bias, especially while we assessed the behavioral characteristics of participants. Health belief model questions were also better if supported by a qualitative approach.
Clinical and Public Health Implications
The evidence from this study suggested that public health policies aimed at increasing cervical cancer screening service utilization better target risky groups discovered in our study such as; non-multipara women, women having low perceived susceptibility& poor knowledge. All HIV-positive women, especially those in high-risk categories identified by our study, require a well-established community sensitization and awareness-building activities. Initiatives for health education should focus on spreading awareness about cervical cancer’s asymptomatic nature and HIV-positive women’s highest risk of the disease.
The current study documented the issue of failure to utilize CCS service also attributed to provider’s recommendation for ART patients to get screened. Higher intentions to the screen have been documented among women who reported discussions on CC with health care providers.38,39 The opportunity presented is that health care providers can be used as an effective intervention to increase the utilization of screening services among HIV-positive women. CCS should therefore form part of the discussion between health workers and HIV-positive women when they go to seek health care. This could take the form of asking patients whether they have ever been screened during routine visits, providing them with more information and support, and recommending them to access cervical cancer screening services. Consequently, effective screening intervention and implementation approaches are warranted if the full benefits of screening and the risk of acquiring the disease are to be recognized.
Conclusion
The prevalence of screening uptake among HIV-positive women was too low. The common reason provided by participants after being asked why they did not get screened was feeling healthy, preceded by embarrassment. Having good knowledge, high perceived susceptibility, being recommended by health care providers to be screened, and multiparity were factors positively associated with CCS utilization in this study.
Supplemental Material
Supplemental Material - Determinants of Cervical Cancer Screening Service Utilization Among HIV-Positive Women Aged 25 Years and Above Attending Adult ART Clinics in Southern Tigray, Ethiopia
Supplemental Material for Determinants of Cervical Cancer Screening Service Utilization Among HIV-Positive Women Aged 25 Years and Above Attending Adult ART Clinics in Southern Tigray, Ethiopia by Lielt Gebreselassie Gebrekirstos, MSc, Meron Hadis Gebremedhin, MSc, Tiwabwork Tekalign Tafesse, MSc, Tilahun Saol Tura, MSc, Mulugeta Geremew Geleso, MSc, and Tsiyon Birhanu Wube, MSc in Cancer Control
Footnotes
Abbreviations
AOR Adjusted Odds Ratio
ART Anti-Retro Viral Therapy
CC Cervical Cancer
CCS Cervical Cancer Screening
CD4 Cluster of Differentiation 4
CI Confidence Interval
COR Crude Odds Ratio
HBM Health Belief Model
HIV Human Immunodeficiency Virus
HPV Human Papilloma Virus
SPSS Statistical Package for Social Science
STI Sexually Transmitted Infection
WHO World Health Organization
VIA Visual Inspection with Acetate
Acknowledgments
We would like to express our deepest heartfelt thanks to Addis Ababa University for covering per diem for data collectors. Our special thanks go to the study participants for their commitment to providing valuable information.
Author Contributions
All the data of this study are available from the corresponding author upon request. All authors contributed equally to this work. LG, MH, TT, TS, MG, and TB contributed to the study concept, design, acquisition of data, contributed to analysis, and interpretation of data. LG and TB contributed to the draft of the manuscript. All authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Addis Ababa University was involved in financial support for data collection.
Ethical Approval and Consent to Participate
Ethical approval was obtained from Addis Ababa University College of the Health Science Department of Nursing and Midwifery Institutional Review Board of the research committee (approval no. ERC/052/2017) and the official letter of cooperation was written to the respective health facility heads. Permission letters were obtained from the respective health facility heads. Written informed consent was obtained from all study subjects before interviewing. No personal details were recorded or produced on any documentation related to the study participants and punctuality was assured.
Availability of Data
The data sets used and/or analyzed during this study are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.