
Abstract
Objective
This study aimed to investigate the risk factors of venous thromboembolism (VTE) in admitted patients with lung carcinoma before surgery.
Methods
We conducted a retrospective case-control study of 94 preoperative lung cancer patients with VTE between January 2017 to December 2020. Each VTE patients was randomly matched with 2 control patients according to residence and gender. The clinical characteristics and related laboratory test results between the groups were compared by univariate analysis, while the risk factors of VTE in preoperative patients with lung cancer were analyzed using multivariate logistic regression analysis.
Results
Patients aged ≥60 years, a history of arrhythmia, homocysteine>15ummol/L, Fibrinogen (FIB) >4 g/L and D-dimer>500 ng/mL were found to be associated with an increased risk of VTE by univariate analysis. The multivariate logistic regression analysis revealed that age ≥60 years (OR=10.985), FIB >4 g/L (OR=8.861) and D-Dimer >500 ng/mL (OR=6.613) were independent risk factors for VTE in patients with lung carcinoma before surgery (P<.05).
Conclusion
For preoperative patients with lung cancer, the independent risk factors of VTE included age ≥60 years, FIB >4 g/L and D-Dimer >500 ng/mL. As for these patients, prophylactic anticoagulant therapy should be considered before surgery.
Introduction
The occurrence of deep venous thrombosis (DVT) or pulmonary embolism (PE), together described as venous thromboembolism (VTE), is a common complication of cancer, with an incidence of 1-20%.1,2 Cancer is recognized as an independent risk factor of VTE, patients with cancer are associated with a four-to seven-fold higher risk of VTE than patients without a malignancy.3,4 Patients with cancer have a prothrombotic state resulting from stasis of the blood caused by bed rest or by tumor compression, vascular injury caused by intravasation of cancer cells or drugs, and blood hypercoagulability caused by the release of cancer cell procoagulant factors. 5 Besides, the development of VTE in cancer patients is related to increases in mortality, and medical costs. Occurrence of VTE in cancer patients has been proved to increase the likelihood of death by two-to six-fold, VTE has become the second leading cause of death in cancer patients.6,7 Besides, costs of patients with VTE associated with hospitalization is 2.5-fold higher, which contributes a substantial economic burden to the family.8,9
Many studies have showed that the prevalence of VTE is increased significantly among lung cancer patients, and It has been reported that patients with lung cancer are more likely to develop thrombotic events than other cancer patients, with an incidence of 13.9%.10,11 VTE can appear before cancer diagnosis, and before the begin of lung cancer treatment, the related mechanism may be that patients are in a hypercoagulable state. 12 One study reported that among 231 cases of lung cancer patients before surgery, the incidence of VTE on admission was 5.2% (12/231). 13 Except cancer-related factors, patient-related factors such as advanced age, race and a priority history of a thrombotic event, and treatment-related factors also contribute to developing VTE in admitted patients with lung cancer. 10 Therefore, recognizing the risk factors of VTE in patients with lung cancer before surgery has become an important task to prevent and intervene in the occurrence of VTE. However, risk factors identification of VTE in lung carcinoma patients before surgery remains poorly studied. Thus, we conducted a retrospective case-control study to analyze the possible risk factors of VTE events in preoperative patients with lung cancer. The aim was to provide a basis for clinical prevention and treatment of VTE, and further improve the quality of life of patients.
Methods
The reporting of this retrospective case-control study conforms to STROBE guidelines. 14
Studied Population
We conducted a retrospective case-control study of all admitted lung cancer patients with a VTE diagnosed between January 2017 and December 2020 at one cancer institution in China. Patients diagnosed with lung cancer and prescribed to have an operation for curative treatment were included. Besides, all cases included were preoperative patients with the diagnosis of a DVT or a PE at admission. Patients with stage IV disease or history of other malignancy were excluded. The diagnosis of DVT was ascertained based on color Doppler ultrasonography or a computerized tomography (CT) venous angiogram and a PE event was confirmed by contrast-enhanced CT.
Data Collection
As cases of VTE were identified retrospectively, we searched the hospital VTE adverse events reporting system, which would record the occurrence of a VTE, in order to avoid the potential loss of some cases. Each VTE patient was randomly matched to two patients without VTE based on residence and gender. The matched patients lived in the same city and had the same gender. Potential risk factors including demographic information along with patient characteristics, laboratory tests of 2 groups patients were collected at admission based on electronic health records system. As part of the routine preoperative workup at our center, homocysteine, fibrinogen and D-dimer were included in the laboratory tests.
Statistical Analysis
The univariate association between VTE and baseline clinical variables was initially characterized using chi-square tests. Variables found to be significant (P < .05) by univariate analysis were subsequently entered into a multivariate stepwise logistic regression analysis with VTE as the response variable. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. Statistical analysis was performed using SPSS software, version 20.0 (IBM, USA), and two-sided P values <.05 were considered statistically significant.
Results
Patient Characteristics
Totally ninety-four patients with lung cancer before surgery developed VTE in the 4-year study period. The median age was 64 years old, and all of the VTE patients were diagnosed with DVT. A total of one hundred and eighty eight preoperative lung carcinoma patients without VTE were selected as matching controls, with a mean age of 65.4±8.7 years.
Univariate analysis of the risk factors for VTE in preoperative patients with lung cancer
Baseline and clinical characteristics of the total study population (N = 282).
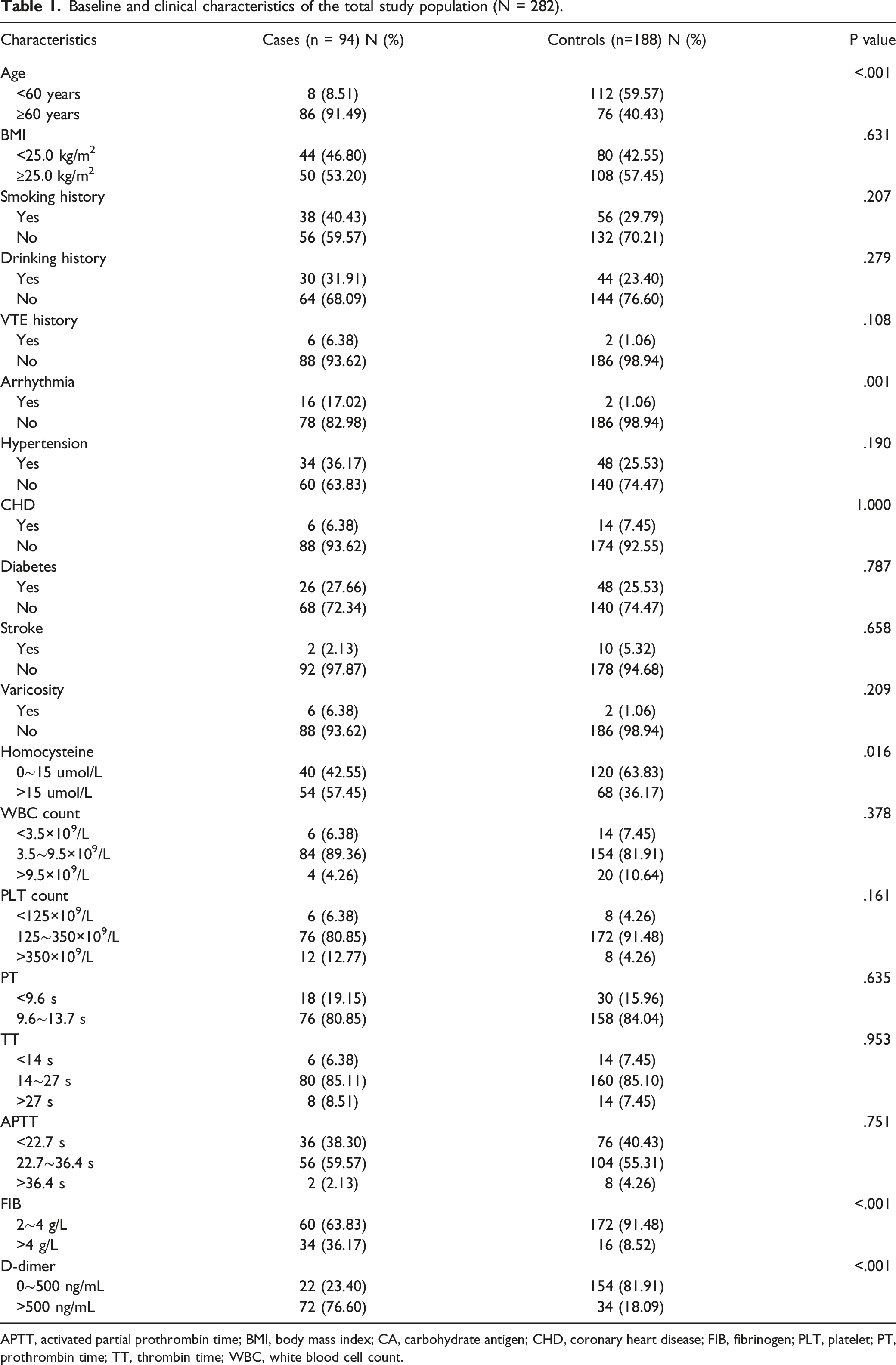
APTT, activated partial prothrombin time; BMI, body mass index; CA, carbohydrate antigen; CHD, coronary heart disease; FIB, fibrinogen; PLT, platelet; PT, prothrombin time; TT, thrombin time; WBC, white blood cell count.
Multivariate analysis of the risk factors for VTE in preoperative patients with lung cancer
Study variables were selected based on the results of univariate analysis and the clinical significance of the influencing factors. With the occurrence of VTE as the dependent variable, and age, a history of arrhythmia, homocysteine, FIB and D-dimer as the independent variables, multivariate logistic regression analysis was performed.
Predictors of developing VTE in preoperative patients with lung malignancy.

S.E., standard error.
Discussion
The primary aim of this study was to identify the risk factors of VTE in preoperative patients with lung carcinoma. Our findings showed that older age was one of the independent risk factors of VTE in this population, patients with age more than 60 years were more likely to have thrombotic events than those below 60 years. In the normal population, the risk of VTE increases with age, but the association between age and VTE in lung cancer patients is controversial. 15 Lee YG et al conducted a retrospective analysis of 1998 consecutive patients with non-small cell lung cancer, and found that advanced age was an independent predictor of VTE development, which is consistent with the conclusion of this study. 16 While one research among 91933 patients with newly diagnosed with lung malignancy revealed that younger age (<45 years old) was a significant predictor of developing VTE within one year of non-small cell lung cancer diagnosis. 17 The reason for this inconsistency may be related to the differences of study subjects, tumor biological characteristics.
D-dimer is the minimal degradation product of fibrin, produced by fibrinolytic hydrolysis, and is a specific marker indicating activation of fibrinolytic system and hypercoagulable state in patients.18-20 During thrombotic event, thrombus fibrinolysis leads to an elevated plasma level of D-dimer.21,22 In this study, we obtained similar results, suggesting that increased D-dimer concentration was correlated with the development of VTE in preoperative lung malignancy patients. Wells clinical prediction model combines with D-dimer testing, which has proved to be useful in the diagnosis of VTE. However, the level of D-dimer would also be elevated in condition of infections, heart failure, tumors, myocardial infarction, stroke, and chronic kidney disease. 23 Thus, National Comprehensive Cancer Network (NCCN) guideline of cancer-associated venous thromboembolic disease recommends that further validation of D-dimer testing and clinical prediction models is warranted before these strategies are incorporated into the diagnosis of VTE in cancer patients. 24
FIB is an acute reactive protein synthesized and secreted by liver cells, which is involved in the endogenous hemostatic process of the body. 25 FIB is also known as coagulation factor Ⅰ, and the increase of its level indicates that the body is in a state of hypercoagulation, which is easy to induce the formation of thrombus.26,27 What mentioning above is consistent with the results of this study, which showed that FIB >4 g/L is associated with higher risk of VTE development in admitted patients with lung cancer.
For preoperative patients with lung carcinoma, at admission, chest CT, and color Doppler ultrasonography are routinely performed to diagnosis the occurrence of VTE events of patients before surgery in many medical centers. Furthermore, although the Caprini risk assessment model has been widely implemented for VTE risk stratification in thoracic surgery patients, it showed to be with low specificity in patients with resectable lung cancer. 28 Our findings may help to recognize the patients with high risk of VTE, and chest CT and ultrasound examination will make sure of the diagnosis next, in order to better use the limited medical resources. Besides, for high-risk patients before surgery, anticoagulant therapy could be given after evaluation of general conditions, such as low molecular weight heparin. However, the current research was a single-center retrospective study with limitations of certain selection bias and small sample size. What is more, although the association between obesity and VTE has been well recognized in the general population and in cancer patients, we failed to find BMI was significant difference between the 2 groups in this study.29,30 Thus, prospective multicenter studies with large sample size are needed to verify the results further, which also can help to establish an effective prediction model of VTE in preoperative patients with lung malignancy.
Conclusions
This case-control retrospective study finds that patients aged more than 60 years old, D-dimer>500 ng/mL, FIB>4 g/L are independent risk factors of VTE in preoperative patients with lung cancer. However, considering of the sample size in this study was small, and this study was conducted in a single medical center, the results may need to be further validated.
Footnotes
Acknowledgments
We thank Hongtao Wang from Medical Department of Tianjin Cancer Hospital, who offers great support for the data collection. We also thank Qingqing Kong from Lung Neoplasms Department of Tianjin Cancer Hospital, who contributes to the study design and data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.