
Abstract
A hospital-based, case–control study was conducted to investigate the association between lifestyle patterns and risk of colorectal cancer (CRC) in the north of Vietnam. Demographic factors employed for the models were age, sex, marital status, occupation, education, income, smoking status, alcohol consumption, vegetable consumption, tea, coffee consumption, and physical activity (PA). Individuals of both groups (n = 154 for the control group and n = 136 for the CRC group) were interviewed using a questionnaire by trained interviewers. The findings showed that moderate PA was inversely associated with CRC risk: odds ratio (OR) = 0.19, 95% confidence interval (CI) = 0.10 to 0.36 with P < .01. The total PA showed that the highest tertile (>2.7 MET-h/d) was associated with the reduced risk of CRC compared with the lowest tertile one after controlling for confounding factors: adjusted OR = 0.25, 95% CI = 0.09 to 0.74, P < .01. Sedentary time was associated with an increased level of CRC risk by 57% as compared between the highest tertile and the lowest one after controlling for confounding factors. Daily consumption of vegetables and 1 to 3 cups of tea per day or more were also associated with decreased risk of CRC. Despite promising findings, a limitation of this research is that it did not establish a temporal relationship between risk factors and CRC due to its retrospective design. However, this is the first analytic study highlighting the role of the active lifestyle pattern associated with reduced CRC risk in Vietnamese adults.
Keywords
Introduction
Cancer is the second leading cause of death globally, and it was responsible for an estimated 9.6 million deaths in 2018. Globally, about 1 in 6 deaths is caused by cancer, with approximately 70% of these deaths occurring in low- and middle-income countries. Around one-third of deaths from cancer are due to the 5 leading behavioral and dietary risks: high body mass index, low fruit and vegetable intake, lack of physical activity (PA), tobacco use, and alcohol use. 1
Colorectal cancer (CRC) is a leading cause of cancer death worldwide. Colorectal cancer was responsible for approximately 1.8 million deaths worldwide in 2018, according to the World Health Organization (WHO). 2 Globally, CRC is the second most common cancer and the third most common cause of death in both men and women. 2 In Vietnam, CRC is the fifth common cause of cancer-related incidence. 3
Healthy dietary pattern and active lifestyle factors have been shown to decrease the incidence of CRC. 4 Therefore, determining the risk factors and possible preventative measures related to CRC is a crucial matter. Several studies have evaluated the influence of dietary factors, particularly nutrition, on the development and prevention of CRC. 5 The probable risk factors associated with CRC are inflammatory bowel disease, history of CRC in first-degree relatives, increased BMI, red meat intake, cigarette smoking, low PA, low vegetable consumption, and low fruit consumption. 6 -9
There is evidence that consumption of foods such as fish, polyunsaturated fatty acids, milk, dietary fiber, whole grains, fruits, nonstarchy vegetables, garlic, and cruciferous vegetables can reduce the risk of CRC. 10 -12 Thus, the exposure to risk factors for CRC may differ among countries and among regions in the same country due to regional variation in traditions, beliefs, cultures, lifestyle, and dietary habits. However, data on protective factors of CRC are quite limited in Vietnam. Data on CRC risk from Vietnam can yield useful insights for developing appropriate policy and program responses both in Vietnam and other similar settings in the world. Therefore, the aim of this study is to describe the lifestyle pattern by a case–control study design in Vietnam.
Methods
Study Design
This was a hospital-based, case–control study, conducted from January 2016 to May 2016 in the Bach Mai Hospital, Hanoi, Vietnam.
Study Participants
The study included 136 patients with colon and/or rectal cancer from Bach Mai Hospital, one of the largest hospitals in Vietnam. Cases were compared with 154 control participants from the same region. Both groups were frequency matched for their age and gender. The inclusion criteria for the case group were Vietnamese nationality and CRC diagnosed in any region of the colon and/or rectum, whereas the exclusion criteria were patients diagnosed with other types of cancer, regardless of age. Controls were recruited from patients’ visitors.
Study Setting
This study was conducted in Bach Mai Hospital, one of the largest central hospitals in Vietnam.
Sample Size and Sampling
We aimed to determine the association between PA and CRC risk, as 30% of Vietnamese adults do not meet WHO recommendations for PA. 13 This level of physical inactivity was used to estimate the required sample size. We further postulate that the odds ratio (OR) for CRC is 2.40. With frequency matching by age and sex between cases and controls on a 1:1 ratio, a total of 232 participants (116 CRC cases and 116 controls) should be required to attain 90% statistical power for such effect size at 5% level of significance. To compensate for potential refusal and withdrawal, 290 participants (136 cases and 154 controls) were recruited. The sample size was sufficient to detect moderate effect sizes for other dietary and lifestyle factors such as vegetable, tea, and coffee consumption.
Measurements
The dependent variable was a dichotomous cancer status (1: CRC diagnosis; 0: non-CRC diagnosis). Cases of CRC comprised 72 men and 64 women (median age = 60 years, range = 32-84 years) with incident, histologically confirmed cancer. Cancers of the colon and rectum and their anatomical subsites were defined according to the International Classification of Diseases, Tenth Edition.
The independent variables included individual characteristics such as age, sex, marital status, education, income, occupation, and family history of CRC. Lifestyle factors included smoking, alcohol drinking, PA (intensity and frequency), sitting time (ST), and other dietary factors such as tea, coffee, and vegetable consumption.
Data Collection
Eligible participants were asked to complete a questionnaire under the supervision of trained interviewers that included personal information as well as information regarding dietary habits. Usual food intakes and habits were assessed using an existing standard dietary questionnaire, including questions about daily intake frequency of fruits and vegetables, dairy products, poultry, and red and processed meat, as well as green tea and coffee. Intake of green leafy vegetables was measured on a weekly basis. Participants were educated about the serving size of each food item before beginning the questionnaire.
Data Analysis and Statistical Method
Statistical analyses were performed with SPSS software version 20. A t test was used to explore the differences between case and control groups for parametric variables, and comparison of the categorical variables was performed by the χ2 test. For each PA variable, the tertile among controls was used as the cutoff point, resulting in 3 increasing levels of exposure, whereas the lowest level was taken as the reference group. The association of total PA with CRC was expressed in terms of metabolic equivalent task hours per day (METs-h/d). Following the compendium of PAs, 14 intensity codes 8.5, 6.0, and 4.5 MET were assigned for strenuous sports, vigorous work, and moderate activity, respectively. Total PA was the sum of all types of PA that was classified into tertile for analyses (low, <2.0 METs-h/d; medium, 2.0-2.7 METs-h/d; high, >2.7 METs-h/d). Total ST was also divided into tertile (low, <1.5 h/d; medium, 1.5-3.0 h/d; high, >3.0 h/d). Unconditional logistic regression models were used to compute ORs with accompanying 95% confidence intervals (CIs) as estimates of associations of total PA and ST with CRC risk. Tests for linear trend were conducted to examine the dose–response relationship using continuous independent variables. All variables were adjusted for the potential confounders as recognized in previous studies. A P value <.05 was considered statistically significant.
Results
General Characteristics of the Study Sample
Table 1 presents the demographic information of the case and control groups of study. The average age of the case and control groups was about 58 years and males accounted for 50.6% for the control group and 52.9% for the case group. The majority of case and control participants were married, 95.4% for controls and 89.7% for cases. There was no significant difference between the case and control groups for occupation, education, smoking, alcohol consumption, and coffee consumption variables. High income, habit of tea drinking (more than 2.2 cups per day), and daily dietary habit of eating vegetables were significantly higher in the control group than that of the cases group.
Characteristics of Participants in the Study Group.
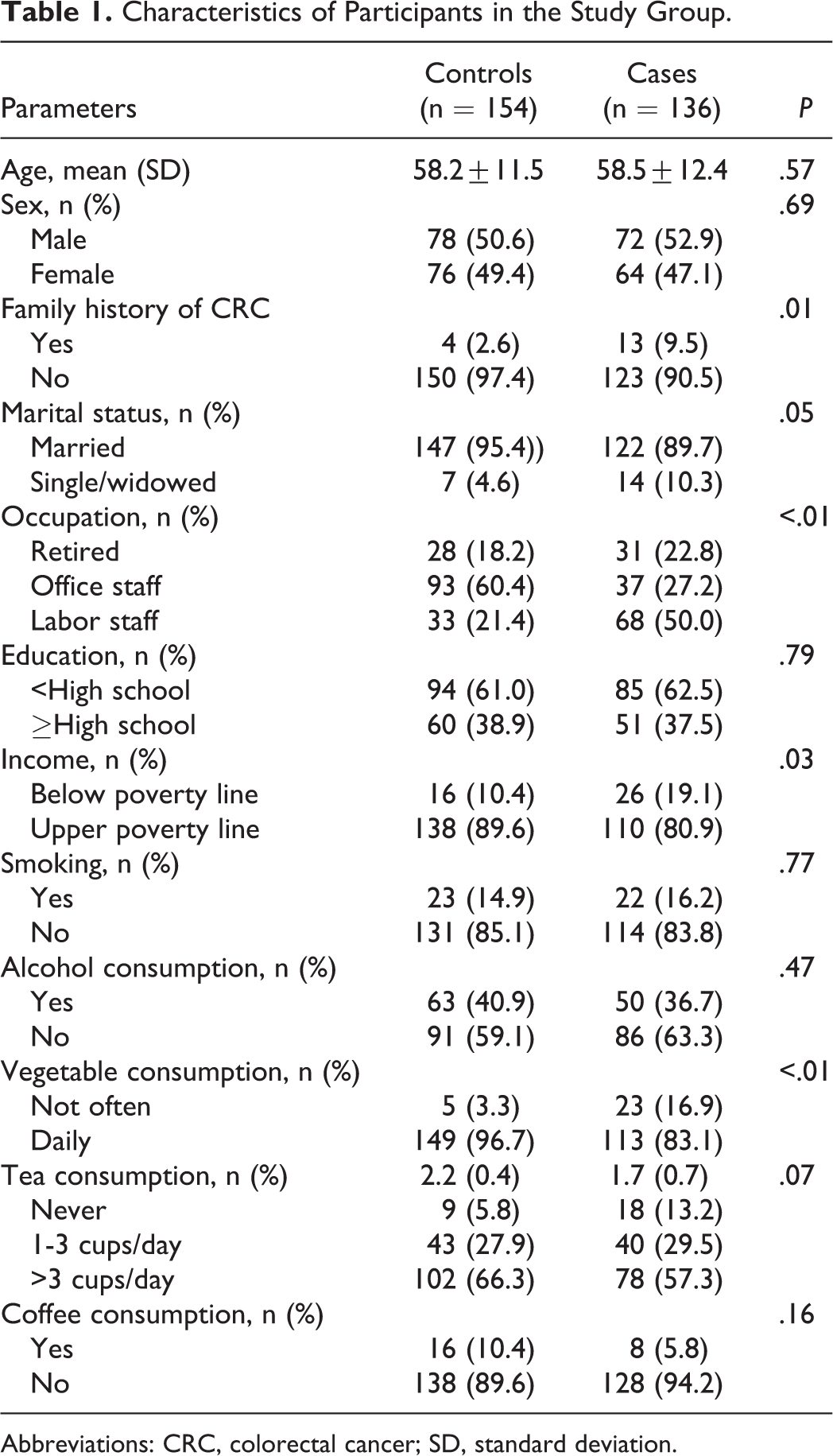
Abbreviations: CRC, colorectal cancer; SD, standard deviation.
Main Findings
Table 2 showed that moderate PA was inversely associated with reduced risk of CRC at a significant level (P < .01) and total PA was associated with decreased CRC risk.
Comparison of Activity Characteristics Among Control and Case Participants.a
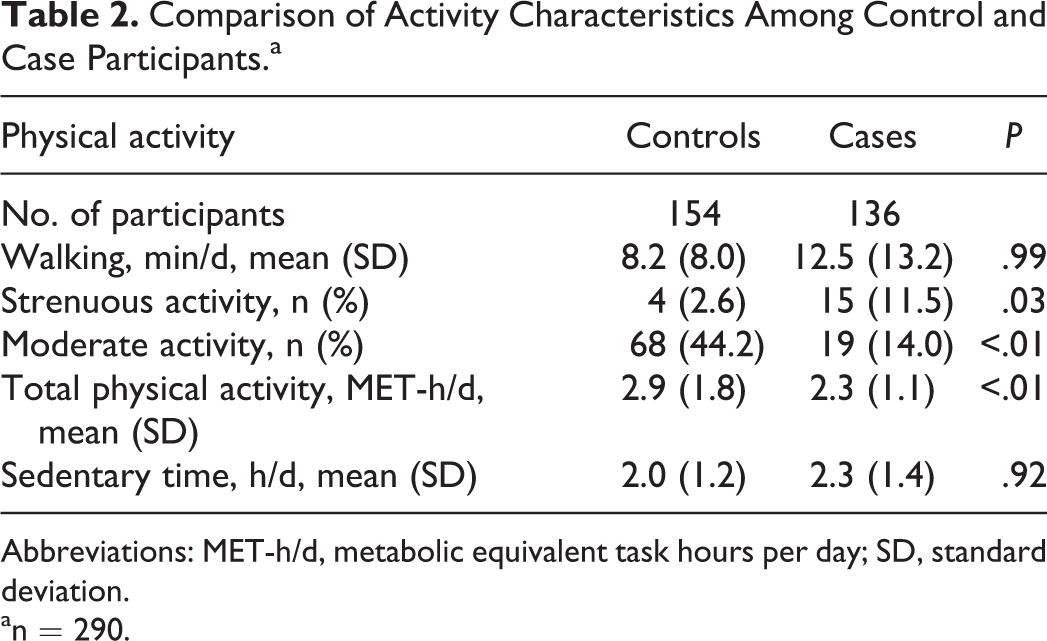
Abbreviations: MET-h/d, metabolic equivalent task hours per day; SD, standard deviation.
an = 290.
Participants who had moderate PA regularly had a statistically significant association in reducing risk of CRC: OR = 0.20, 95% CI: 0.11 to 0.36 and OR = 0.19, 95% CI: 0.10 to 0.36 for crude model and adjusted model, respectively (Table 3).
Independent Associations of Habitual Physical Activity and Sedentary Time With Risk of CRC.a

Abbreviations: CI: confidence interval; OR: odds ratio; PA: physical activity
an = 290.
bAdjusted for variables: age (year), sex (male/female), marital status (married/single or windowed), occupation (retired/office/labor), education (<high school/>high school), family history of colon diseases (yes/no), income (below poverty line/upper poverty line), smoking (yes/no), alcohol consumption (yes/no), and coffee consumption (yes/no).
cBased on unconditional logistic regression, treating total PA and sedentary time as continuous variable.
High total PA was inversely associated with CRC risk compared with low tertile of total PA in both crude and adjusted models: OR = 0.30, 95% CI: 0.12 to 0.76 and OR = 0.25, 95% CI: 0.09 to 0.74, respectively.
In addition, those who spent more than 3 hours per day sitting had 1.6 times increased risk of CRC. This relationship between ST and increased risk of CRC was determined to be statistically significant (P < .01) for both crude and adjusted models.
Discussion
The findings of a recent systematic review and meta-analysis suggest that higher PA, in terms of both recreational and occupational activity, was associated with a lower risk of colon and rectal cancer. 15 Dose–response analyses were supportive of the outcomes as compared between the highest versus lowest categories of PA.
To the best of our knowledge, we are the first to have retrospectively examined active lifestyle patterns including PA, ST associations, and healthy dietary habits with CRC risk among Vietnamese adults. Our study contributed to evidence that high levels of PA, including moderate and total PA, were inversely associated with odds of CRC after adjusting for confounders in the full model: OR = 0.20 and 0.25, respectively (Table 3). The findings were a higher level of reduced CRC risk compared to other regions such as European 16 or North Amerian 17 but were consistent with reports in the Asian region. 18 This could be explained by the fact that the Vietnamese retain a more traditional diet while the United States and Europe are becoming more highly processed. 15
A sedentary lifestyle was associated with a slightly increased risk of CRC, that is, spent 1.5 to 3.0 h/d seated (7%), but becomes more robust for those who spent more than >3.0 h/d (57%) in a sedentary position after adjusting for confounding factors. Our findings were similar to a systematic review-meta analysis by Biswas et al. 19 who reported increased risks ranging from 6% to 40%. However, they differed from the recent systematic review by Mahmood et al 15 who observed increased risks ranging from 50% to 60%.
In our study, those who had a habit of eating vegetables daily were inversely associated with CRC risk, statistically significant with P < .05. Eating more fruits and vegetables can reduce the risk of bowel cancer because they contain vitamins and minerals. It was revealed that antioxidant vitamins and minerals help prevent cellular damage that can lead to cancer cells. Fruits and vegetables increase the amount of fiber, increasing the weight of waste, which helps to eliminate waste better. 20
In particular, the beneficial role of antioxidant-rich foods and beverages has received much attention. 21 Tea, especially green tea, is widely consumed in Asia. 22 It contains bioactive compounds including catechins 21,23 which have been demonstrated to increase insulin sensitivity and prevent glucose metabolism disorder among in vitro and in vivo studies. 24 -26 Our findings demonstrated those who had a habit of drinking tea at 1 to 3 cup per day or more was associated with a reduced risk of CRC, but not statistically significant. This finding was consistent with a recent meta-analysis, which reported tea consumption has an inverse impact on CRC risk. The summary OR of CRC for the highest versus lowest tea consumption was 0.93 with 0.87 to 1.00 of 95% CIs. 27
Inflammation was evident in the etiology of CRC. 28 Inflammation can make cell proliferation, microenvironmental changes, and oxidative stress, which can promote carcinogenesis. 29 Adipose tissue secretes predominantly cytokines (pro-inflammatory factors) such as adipokines. 30 These cytokines affect insulin sensitivity through activation of adenosine monophosphate protein kinase. Physical activity is related to lower levels of pro-inflammatory cytokines and higher levels of adiponectin. 31 Sedentary behavior may raise the levels of pro-inflammatory cytokines while decreasing levels of adiponectin. Reports suggest that regular exercise increases the number and activity of macrophages, natural killer cells, and cytokines results in killing cancer cells. Shorter gut transit time with vigorous exercise has been shown to reduce exposing time of potential carcinogens in food residues. 32
Several limitations should be mentioned in this study. Firstly, a cause–effect relationship between exposures and CRC cannot be established due to the retrospective cross-sectional design. Secondly, there are inherent biases from this observational study. To minimize selection bias, only patients with incident CRC were chosen, while controls were recruited from patients’ visitors. These controls were frequency matched to the cases by age and sex but were unlikely to share the same risk profiles. Thirdly, recall bias may lead to spurious associations between exposures and the outcome of interest. 33 In this study, the direct interview of both case and control groups by the same trained interviewers was done to reduce recall bias and improve the accuracy of information obtained. Finally, our findings cannot be generalized to the entire Vietnamese population because all participants were recruited from the same catchment area.
In summary, we have demonstrated that active lifestyle patterns, including regular moderate PA, daily vegetable consumption, and daily green tea consumption, are inversely associated with a reduced level of CRC risk among Vietnamese adults. This study may provide useful evidence for developing effective community-based interventions or appropriate policy in Vietnam.
Footnotes
Authors’ Note
The protocol of this study was approved by the Scientific and Ethical Committee in Biomedical Research, Hanoi University of Public Health (Approval Number 159/2015). All human subjects in the study were asked for their consent before collecting data, and all had complete rights to withdraw from the study at any time without any threats or disadvantages.
Acknowledgments
The authors would like to thank the patients of the Department of Polyclinic Research, Bach Mai Hospital for involving and facilitating the collection of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.