
Abstract
Background
Cervical cancer (CCa) is the second most common type of cancer and a leading cause of death among adult women in Ethiopia. However, at the moment, there is a lack of evidence that can be generalizable as a whole to the country regarding the uptake of cervical cancer screening.
Objective
The aim of this review was to assess the pooled estimated uptake of CCa and to identify the major barriers to cervical cancer screening (CCS) uptake among adult women in Ethiopia.
Method
The review protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) with a registration number of CRD42022353954. The data were searched electronically using Google Scholar, PubMed, Medline, and Web of Science search engines. The heterogeneity of the literature was assessed using Cochran’s (Q) test and Higgin’s and Thomson’s (I2) statistic. The Rosenthal approach, Fail-safe N method, Egger’s test with a P-value <0.05, and funnel plot symmetry were used to detect publication bias. Random effect analysis was used to find out the pooled effect size. The Stata 17 software was used to perform analysis.
Result
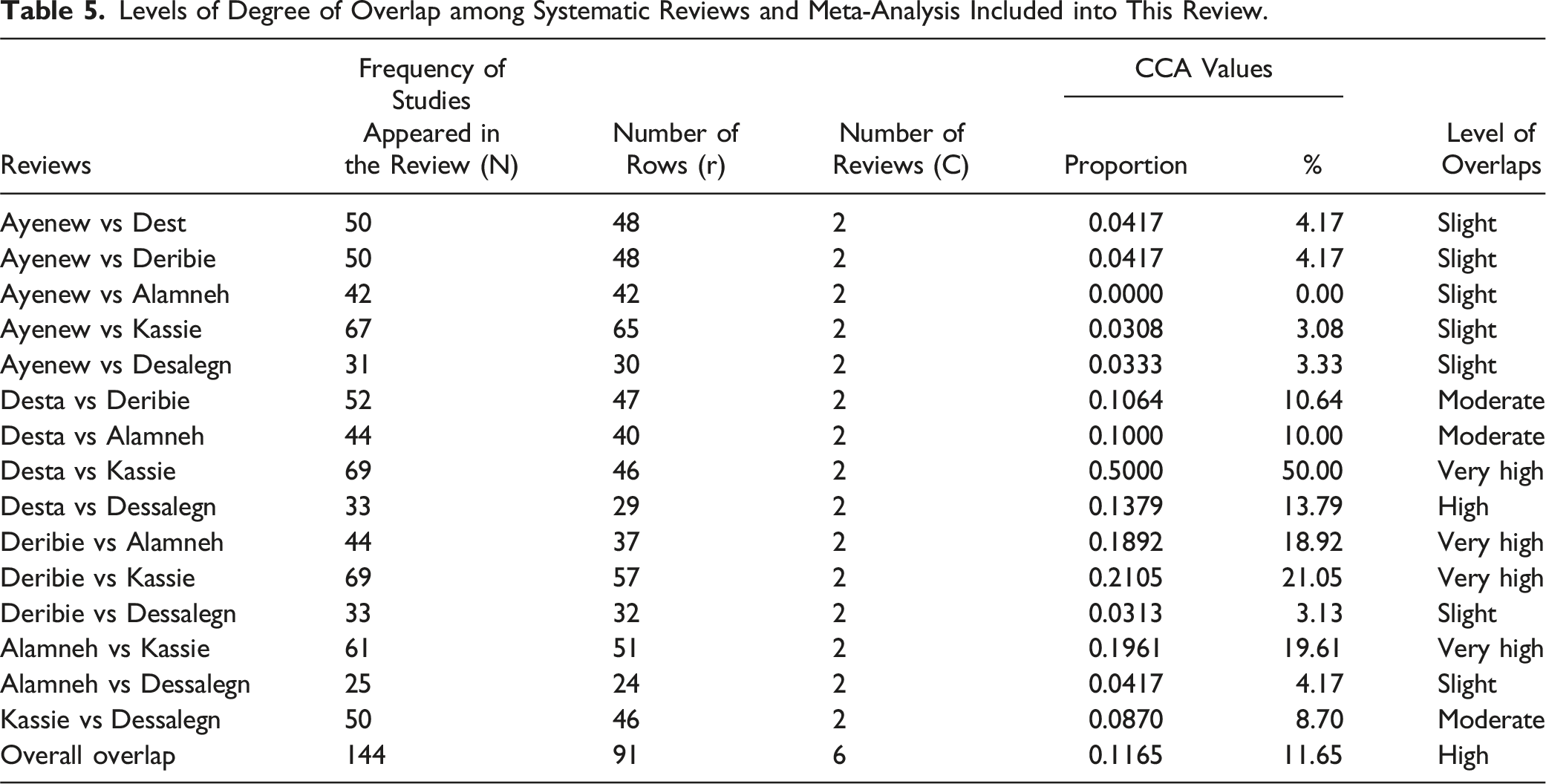
The pooled estimated uptake of CCS was 13.08% (POR 13.08; 95% CI: 10.24, 15.93; I2 = 81.93%). Common factors associated with uptake of CCS were adequacy of knowledge (POR = 3.48; 95% CI: 2.74, 4.23; I2 = 0%), attitudes of women (POR = 3.51; 95% CI: 2.96, 4.07; I2 = 0%), and perceived susceptibility (POR = 4.03; CI: 2.68, 5.39; I2 = 46.38%). A slightly high degree of overlap of studies was observed.
Conclusion and Recommendation
The pooled estimated CCS is low. Factors like adequacy of knowledge of CCa, attitudes of women, and perception of susceptibility among women showed a significant association with cervical cancer screening uptake. Creating a platform where women can get adequate and focused information about cervical cancer and screening is crucial.
Introduction
According to a 2023 study, cancer is estimated to be a leading cause of premature mortality worldwide. 1 Cancer is the second leading cause of morbidity and mortality in the world next to cardiovascular disorders (CVD). 2 In low Human Development Index (HDI) countries, cervical cancer (CCa) accounted for the leading cause of preventable premature cancer deaths, representing 26.3% of the total preventable years of life lost (YLLs) due to cancer. 1
Cervical cancer is the second most common type of cancer and one of the leading causes of death among women in Ethiopia. 3 The uptake of cervical cancer screening (CCS) varies globally. It is high among high income countries and low among low-income countries. Cervical cancer screening adherence rates have consistently been higher in more developed regions with a higher Socio-Demographic Index (SDI). In 2019, the global adherence rate among women aged 20-69 years was 33.66%. This rate was twice as high in high-income countries (HICs) at 75.66% compared to low- and middle-income countries (LMICs), which had an adherence rate of only 24.91%. CCS utilization is too low 5.28% in Africa. 4 A systematic review of studies in sub-Saharan countries showed a slightly higher uptake of CCS at 12.87% compared to the overall African uptake. 5 One of the studies conducted in Uganda showed 47%, higher uptake of CCS. 6 One of the community-based cross-sectional surveys conducted in Ethiopia (2017), which covers all regions and two city administration, shows an extremely low CCS rate 2.9%. 7 But recent studied showed incremental uptake of CCS ranging from 13.8% in Durame, 8 19.8% in Hawasa town 9 to 36% in Asossa zone, Benishangul region. 10
A global systematic review identified significant associations between various factors influencing CCS utilization. These factors include demographic characteristics like marital status, education level, healthcare access, and employment status, lifestyle factors such as body mass index (BMI), smoking, alcohol consumption, and physical activity, and personal history elements like parity, mental illness, and chronic diseases. 4
Another systematic review of “Barriers and Facilitators for Cervical Cancer Screening among Adolescents and Young People,” which included studies from all levels of countries (LMICs and HICs), showed three major categories of barriers: (1) Lack of knowledge/awareness: 26 studies reported a lack of knowledge, 3 studies reported a lack of physician recommendation, 4 studies reported misinformation about the necessity of screening in the absence of symptoms, and fear of pelvic examination as major barriers to the low uptake of cervical cancer screening; (2) Negative perceptions toward the cervical cancer screening test were the second major category of barriers to uptake: 10 studies reported fear of the screening procedure, 16 studies reported embarrassment, 2 studies reported discouragement due to the gender of the screening provider (male providers), 2 studies reported stigma, and 2 studies reported lack of privacy as major barriers; and (3) Systemic barriers such as low accessibility of services, lack of trained screening providers, gender preference, lack of transportation, the cost of screening, and time constraints were reported by 6, 1, 1, 2, 6, and 3 studies, respectively, as major systemic barriers to cervical cancer screening uptake. 11
Many studies have been conducted in various parts of Ethiopia, identifying various types of barriers. The study in Hossana showed that a lack of awareness and poor attitudes toward cervical cancer can influence the uptake of CCS. 12 The barriers to CCS uptake in Ethiopia vary by location and time to time; a study conducted in Addis Ababa (2020) shows that being a rural resident, having a low income, and having an unlikely chance of accessing CCS are significant factors 13 ; in Dire Dawa (2020), being younger, unemployment, lack of knowledge, and recommendation by health care providers; and in Arba Minch (2016), lack of knowledge, a poor (fatalistic) attitude toward CCa, low perceived susceptibility, having many contending issues, financial constraints, and emotional barriers were identified as factors affecting CCS uptake. 14 Some systematic reviews and meta-analyses conducted in Ethiopia identified barriers and factors affecting CCS uptake. However, these reviews do not include all important factors that can influence cervical cancer screening uptake. This may emerge from the findings of the studies included, which could result from using a non-standardized tool and including various target participants (e.g., women from the general population and HIV-positive women), who may face different barriers. This will complicate the design interventions to overcome these barriers.
Therefore, addressing various types of barriers may need high level of evidence to influence policy makers to promote cervical cancer screening, treatment and reduction of suffering among women caused by cervical cancer. This umbrella review explored the major barriers to cervical cancer screening uptake and aims to contribute to the development of policy-based interventions to increase cervical cancer screening rate. Additionally, this review summarizes evidence from research conducted in Ethiopia and provides findings that may be generalizable to women in a general population. This review has the potential to inform interventions that address barriers and improve the uptake of CCS among targeted women and researchers working to enhance CCS uptake.
Questions for Review
What is the uptake of cervical cancer screening in Ethiopia?
What are the major barriers affecting CCS uptake among adult women in Ethiopia?
Objectives
The aim of this review was to assess the pooled estimated uptake and identify the major barriers to CCS uptake among adult women in Ethiopia.
Methods and Materials
Protocol Registration
The PROSPERO registration protocol was used to register the umbrella review. The review protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) with a registration number of CRD42022353954.
Data Search Strategy
Electronic database search engines like Google Scholar, PubMed, Medline, Web of Science, Science Direct, and Hinari were used to search for systematic reviews and meta-analyses on cervical cancer screening uptake and barriers in Ethiopia. Search terms were developed based on adapted PICO questions to identify relevant systematic reviews and meta-analyses. Keywords such as “cervical cancer screening”, “utilization”, “prevalence”, “uptake”, “practice”, “VIA”, “cervical cancer”, “pre-cervical cancer screening”, “barriers”, “knowledge”, “attitude”, “determinants”, “ predictors,” “associated factors, and Ethiopia” were used to identify articles. We employed “AND” and “OR” Boolean operators. A PRISMA critical appraisal follow-up chart was used to determine the number of studies.
Eligibility Criteria
Systematic reviews and meta-analyses conducted from 2010 to July 2022, published in English and conducted in Ethiopia were included. This review included systematic reviews and meta-analyses that reported either the utilization or uptake of cervical cancer screening or the cervical cancer screening predictors, determinants, or barriers in Ethiopia. All non-systematic reviews and meta-analyses and qualitative systematic reviews and meta-analyses were excluded.
Risk of Bias Assessment
The JBI critical appraisal instrument for systematic reviews and research syntheses was used to assess the quality of systematic reviews and meta-analyses for inclusion in the umbrella review. Two independent reviewers (EM and HA) conducted the critical appraisal of each research synthesis and decided whether to include or exclude it from the review. Eleven (11) questions from the JBI were used to assess the quality of systematic reviews or meta-analyses. Each question was answered as “yes”, “no”, or “unclear”. With Not applicable (“NA”) is also provided as an option. A mean of score 7 was deemed an acceptable quality for the study to be inclusion in the umbrella review. Systematic reviews and Meta-analysis with a mean score of less than 7 were excluded from the review. Disagreement between two reviewers was not evident at the time of quality assessment using JBI checklists.
Data Extraction
The standardized JBI data extraction tool was used to extract relevant data from the included systematic review and meta-analysis. The data were extracted by two reviewers (EM and HA). There were no disagreements between the reviewers. The information regarding the objectives of the included review, participants, setting and context, the number of databases searched, the date range of database searches, the date range of included studies for each outcome of interest, the number and types of studies the country of origin of primary research studies in the synthesis, the instrument used to appraise the primary studies, and quality rating were used to extract the data.
Analysis of Degree of Overlap in Meta-Analysis
The degree of overlap among studies across systematic reviews was assessed using the corrected cover area formula. Corrected covered areas (CCAs) are calculated using the following formula:
15

Most of the time, overlap can occur when systematic reviews on the same topic include one or more similar or identical primary studies. Citation matrices were generated to assess the overlap in studies across systematic reviews and meta-analyses. Corrected covered areas (CCAs) were calculated, with values interpreted as CCA = 0-5 indicate slight overlap; 6-10 indicate moderate overlap; 11-15 indicate high overlap; and >15 is very high overlap. 16 The overlapping data from the same primary studies reported across multiple systematic reviews may include: overlapping risk of bias assessments; pooled effect estimates across similar outcomes; and meta-analysis results (e.g., I2 heterogeneity statistics), or overlapping certainty of the evidence assessments.
Data Processing and Analysis
For each meta-analysis, the reviewers estimate the effect size of cervical cancer screening using a random-effects model, and a forest plot is used to assess the effect size. The authors evaluate heterogeneity using Cochrane’s Q and I2 statistics and the small study effect (Egger’s test); the reviewers also estimate the evidence of excess significance bias. Evidence from each screening was graded according to pre-specified criteria (JBI`s criteria). The extracted data were entered into an Excel spread sheet and imported into Jamovi R-based software version 2.2.5 and Stata version 17. Heterogeneity (I2) was evaluated as follows: I2 ≤ 25% indicates low, 25%-50% moderate, and ≥75% substantial heterogeneity. 17 Higher P-values (P > 0.01) were used to declare heterogeneity 18 and a P-value <0.01 indicates no heterogeneity. A random-effects meta-analysis model was used to estimate the pooled prevalence of CCS uptake and the pooled effect of barriers in the reviews. A restricted maximum likelihood model was used to estimate the pooled prevalence of CCS uptake. The Rosenthal approach (Fail-Safe N method) and Egger’s tests, with a P-value less than 0.05, were used to indicate the presence of publication bias. The symmetry of the funnel plot also indicates publication bias. A forest plot is used to estimate the pooled prevalence of uptake of CCS at 95% confidence intervals. In this plot, the size of each box indicates the weight of the study, while each crossed line represents a 95% confidence interval.
Ethical Approval
This review does not include the direct involvement of any human participants or human material. However, ethical approval was obtained from the Addis Ababa University College of Health Science Institutional Review Board (IRB) with letter number 081/22/SPH dated October 25, 2023, as part of a PhD curriculum.
Results
Searching for the Result
A total of 4126 studies were identified using various search strategies. About 4120 studies were excluded. Finally, six systematic reviews and meta-analyses were retrieved. A PRISMA flow diagram was used to show how the studies were identified. Systematic reviews and meta-analysis conducted from 2010 to July 2022, published in English language and conducted in Ethiopia were included. Individual studies and qualitative systematic reviews were excluded from the review. Only systematic reviews and meta-analyses that reported on the utilization or uptake of cervical cancer screening as well as predictors, or determinants, or barriers to CCS in Ethiopia were included (Figure 1). PRISMA follow diagram for study identification.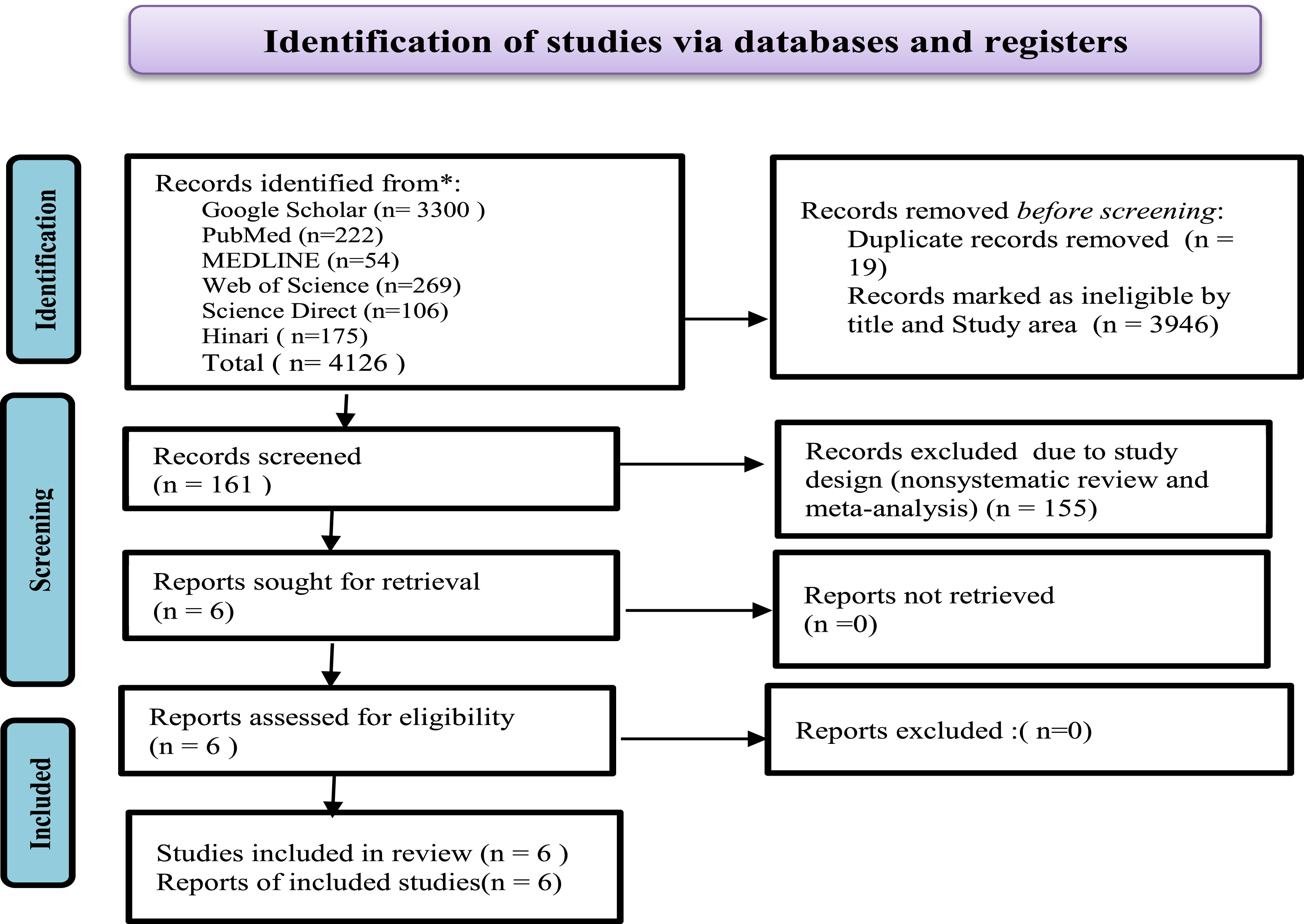
Quality and Characteristics of the Included Systematic Review and Meta-Analysis
Characteristics of Systematic Reviews and Meta-Analysis Included Into Umbrella Review.

N:B: Y = 1, N = 0.
Forest Plot Showing the Estimated Pooled Prevalence of Cervical Cancer Screening Utilization in Ethiopia; Umbrella Review.

Pooled Estimate of Cervical Cancer Screening Uptake
In this umbrella review, six systematic reviews (SRs) and meta-analyses (MAs) were included.19-24 A random effects model was computed to estimate the pooled estimated effect size of uptake of cervical cancer screening in Ethiopia. A forest plot is used to show the pooled estimated effect size and heterogeneity. The estimated pooled uptake of cervical cancer screening utilization or uptake among reproductive age women in Ethiopia was found to be 13.08% (POR = 13.08%, 95% CI: 10.24%, 15.93%; I2 = 81.93%, P < 0.00). The result of this review showed that there is a substantial level of heterogeneity among the systematic reviews and meta-analysis included in this review. The result of the Galbraith plot analysis showed no outlier study. All systematic reviews and meta-analyses included in this review fail with the 95% confidence interval line of the Galbraith plot. This indicates that even though I2 indicates substantial heterogeneity, the heterogeneity is not significant (Figures 2 and 3). Forest plot showing the estimated pooled prevalence of cervical cancer screening utilization in Ethiopia; umbrella review. Assessment of heterogeneity of the systematic review and meta-analysis included into the review (Galbraith plot) indicating no outlier of effect size.

Sensitivity Analysis
Only one systematic review and meta-analysis fulfill the criteria for conducting a sensitivity analysis. Five out of six systematic reviews and meta-analyses19-23 included study subjects who were from the general population, but one of the systematic reviews and meta-analyses had study subjects with different characteristics (HIV-positive study participants).
24
This article was selected for sensitivity analysis because its study subjects are a special population (HIV-positive women), and it has the largest effect size compared to the articles included in the umbrella review. Therefore, sensitivity analysis was conducted by removing this SR and MA with a special study population.
24
The estimated pooled effect size of CCS uptake among the general population women after removing SR and MA (with HIV positive women) was reduced from 13.08% to 12.50% (POR 12.50%; 95% CI: 9.68, 15.38; I2 = 82.98% and P < 0.001). Even though the pooled estimate of cervical cancer screening uptake is reduced from 13.08 to 12.50%, the heterogeneity is still high and increased from 81.93% to 82.98%. The result of sensitivity analysis does not show any difference in heterogeneity and indicates no significance in heterogeneity (Figure 4). Forest plot for pooled estimated effect of CCS uptake among women in general population.
Publication Bias
Assessment of Publication Bias of Systematic Reviews and Meta-Analysis Included into the Umbrella Review.

Note. Fail-safe N Calculation Using the Rosenthal Approach.

Funnel plot for assessment of heterogeneity among SR and MA included into the umbrella review.
Trim and Fill Analysis
Results of Trim and Fill Analysis to Detect and Adjust Publication Bias among Systematic Reviews and Meta-Analysis Included into Umbrella Review.


Barriers to Cervical Cancer Screening Utilization or Uptake
Five out of six systematic reviews and meta-analyses19,21-24 included in this review indicate that women with adequate knowledge were more than three times (POR = 3.48; 95%CI: 2.74, 4.23; I2 = 0%, P = 0.84) more likely to utilize cervical cancer screening compared to women who have inadequate knowledge about cervical cancer and screening. The result of this analysis showed that there is no heterogeneity (I2 = 0%) among the SR and MA included in this review, and the funnel plot also indicates symmetry of the plots, justifying that there is no publication bias (See Figures 1 and 2 of the supplementary file).
The analysis of three SRs and MAs19,21 showed that women with favorable attitudes toward CCS were 3.51 (POR = 3.51; 95% CI: 2.96, 4.07; I2 = 0.00%, P = 0.65) times more likely to utilize CCS compared to women with an unfavorable attitude toward CCS uptake and no heterogeneity (I2 = 0.00%), and the funnel plot also shows no publication bias among the reviews included in this review. (See Figures 3 and 4 of the supplementary file).
The other variables indicated as a barrier to uptake of CCS by SRs and MAs were having a history of STI infection in women in their lives. This was reported by SR and MA.19,22 SR and MA by Ayenew et, al (2021) and Desta et, al (2021) showed that women with histories of STIs were 4.86 times (POR = 4.86; 95% CI : 2.57, 7.15; I2 = 0.00, P < 0.001) more likely to uptake cervical cancer screening.
Only three out of six SR and MA19,22,24 indicated that the women`s perceived susceptibility to contracting CCa was reported as a barrier to uptake of cervical cancer. In this review, we identified that the pooled estimate of perception of susceptibility of women to acquire CCa is more than 4 times (POR = 4.03; CI: 2.68, 5.39; I2 46.38%, P = 0.15) higher to utilize CCS compared to women who do not perceive themselves susceptible . A low level of heterogeneity was observed among studies (I2 = 46.38%). Egger`s test (P-value = 0.417) among the reviews indicates that there is publication bias. (see Figure 5 and Table 1 of the supplementary file)
Only one out of six SRs and MAs showed significant association of between history of multiple sexual partners, getting advice from health care providers, and age of women and CCS uptake (OR = 5.01, 95% CI:2.61, 9.61; I2 = 70.2%, P = 0.009 ), (OR = 4.58, 95% CI:3.26.6.43; I2 = 55.9%, P = 0.034), and (OR = 4.58, 95% CI:2.81.7.46; I2 = 5.0%, P = 0.367), respectively. 19
Degree of Overlaps
Levels of Degree of Overlap among Systematic Reviews and Meta-Analysis Included into This Review.
Discussion
The overall estimated pooled effect size for cervical cancer screening utilization in Ethiopia was 13.08%. This review indicates a higher uptake of CCS compared to country profiles by WHO 25 but lower compared to global systematic reviews and meta-analyses, which show CCS utilization varying from 11.70% in South Africa to 82.57% in Denmark, confirming higher CCS utilization in high-income countries (75.66%). The results of this study show much lower CCS utilization compared to Europe (65.36%) and America (75.03%), but higher than Africa (5.28%). 4 The variation in CCS utilization may be due to differences in socio-economic factors, healthcare infrastructure, and awareness campaigns on screening rates. In high-income countries, better government funding, accessibility, and availability of services can ensure higher utilization. In low-income countries, including Ethiopia, barriers such as lack of infrastructure, insufficient awareness, cultural taboos, and the cost of screening services lead to low utilization of CCS services. The low rate of CCS utilization in Ethiopia may lead to high morbidity and mortality among women due to CCa, given that cervical cancer is highly preventable through early detection and treatment. The finding of this study suggests that a significant portion of women in Ethiopia are at risk of late-stage diagnosis, 26 which could reduce survival rates. Efforts to improve CCS utilization should focus on enhancing healthcare accessibility ((especially in rural and underserved areas), increasing awareness, reducing stigma (engaging community leaders to address cultural and social barriers), and ensuring the affordability of screening services.
The result of this review is supported by a systematic review and meta-analysis conducted among sub-Saharan countries (12.87%). 27 This finding suggests that Ethiopia is not an outlier but part of a broader regional pattern of low screening rates. Sub-Saharan Africa faces several overarching healthcare challenges, such as a lack of well-equipped health infrastructure (especially in rural areas), limited awareness about the importance of CCS, cultural and social barriers (including stigma, taboos, or misconceptions about CCS), and economic challenges in accessing healthcare services that could contribute to low CCS uptake. To improve CCS utilization in Ethiopia, it is crucial to integrate screening into primary healthcare, create mobile and outreach service opportunities, implement education and awareness campaigns, as well as provide affordable and accessible services.
Two SRs and MAs by Ayenew et al (2021) and Desta et, al. (2021) showed that women with histories of STIs were 4.01 and 5.39 times more likely to undergo cervical cancer screening, respectively. The result of this study is supported by the study conducted in Addis Ababa among female nurses. 28 This consistency across studies highlights that a history of STIs is a key motivating factor for cervical cancer screening, especially when individuals are made aware of the associated risks. Moreover, this suggests that raising awareness about the connection between STIs and cervical cancer could enhance screening rates both in the general population and among specific groups, such as healthcare workers.
Five out of six SR and MA19,21-24 identified inadequate knowledge as a barrier to cervical cancer screening (CCS). This indicates that women with adequate knowledge about CCS are 3.48 times more likely to utilize screening compared to those with low knowledge. The results of this review align with a systematic review of studies from low- and middle-income countries, which also identified a lack of knowledge or awareness as a barrier to the uptake of CCS.
Refs. 5,29,30. Inadequate knowledge was identified by this study as a major barrier to cervical cancer screening (CCS) and is a key finding in five out of six systematic reviews (SRs) and meta-analyses (MAs). These studies indicate that women with sufficient knowledge about cervical cancer and its screening procedures are more likely to utilize CCS services than those with inadequate knowledge. The result of this study underscores the critical importance of awareness and the need for educational interventions as part of comprehensive cancer prevention strategies. Addressing the issues of increasing knowledge significantly improves CCS utilization.
The result of this review indicated women with favorable attitudes are more likely to utilize cervical cancer screening. It is supported by the SR and MA conducted among African HIV women. 31 Although HIV-positive women are a vulnerable population with greater exposure to healthcare information than women in the general population, a positive attitude toward healthcare services influences the health-seeking behavior of both HIV-positive and general population women. The consistent findings across the studies highlight the significance of addressing attitudes in public health education campaigns designed to increase CCS utilization. Positive attitudes may reflect not only heightened awareness but also trust in the healthcare system and perceived accessibility of services. Consequently, enhancing healthcare infrastructure, offering culturally appropriate information, and ensuring respectful, supportive healthcare experiences can help foster favorable attitudes, ultimately leading to increased screening uptake rates.
Three SR and MA19,22,24 explored women`s perception of susceptibility as a facilitator to uptake cervical cancer screening. These three SR and MA showed that women who perceived they were susceptible to contracting cervical cancer were 4.03 times more likely to uptake cervical cancer screening compared to women who did not perceive they were susceptible to CCa. The result of this review is supported by SR and MA conducted in Australia and sub-Sharan Africa.27,30 The similarity may stem from women who perceive themselves as susceptible wanting to know if they are free of CCa, leading them to undergo screening. The relationship between perceived susceptibility and screening utilization is a significant concept in health psychology and public health. Designing public health interventions that effectively convey personal risk can greatly contribute to increasing CCS uptake, especially when combined with accessible, supportive, and culturally tailored screening services. Helping women recognize their susceptibility to cervical cancer and offering CCa screening can enhance early detection rates and reduce the overall burden of the disease.
From all SR and MA included in this umbrella review, only one SR and MA 19 indicates history of having multiple sexual partners of women as factors affecting CCS utilization. This result is supported by study conducted Gonder, Ethiopia 32 Women with multiple sexual partners were five times more likely to undergo CCS. Having multiple sexual partners may expose them to STIs, which can result in ulcers, discharge and pain in the reproductive organs especially in the vagina and vulva. Women who experience such health problems in their reproductive organs may think they are at risk of contracting CCa. This concern leads women to consider and undergo CCS. Giving attention to behavioral education during health education provision is crucial.
Women in their 30s were 4.58 times more likely to utilize CCS. The result of this review is supported by the large-scale survey in Germany, 33 the Sub-Saharan SR and MA, 27 and the national survey of Spain. 34
As women age, their exposure to information about cervical cancer tends to increase, enhancing their understanding of the disease. They may witness others suffering from cervical cancer and receive information from various mass media sources. This heightened awareness often leads to greater concern for their own health. As a result, they may start to think about and worry more about cervical cancer, prompting them to seek cervical cancer screenings (CCS). This increased concern often drives women to prioritize their health by seeking cervical cancer screenings (CCS), highlighting how age and awareness impact proactive healthcare behaviors.
Only a single SR and MA 19 included in this umbrella review showed that getting advice from health care providers (HCPs) will promote CCS uptake. According to this review, women who get advice from HCPs are more than 4 times likely to uptake CCS service. The result of this review was supported by a systematic review and meta-analysis conducted among Asian women living in America, 35 a national survey in Spain 34 and SR and MA in Nigeria. 36 Women who receive recommendations from healthcare providers (HCPs) are more likely to participate in cervical cancer screening (CCS), highlighting the strong influence of professional advice on health-related choices. The trust individuals have in their healthcare providers amplifies the effectiveness of HCPs advice, particularly in the context of preventive care. By creating a supportive and informative dialogue, HCPs can significantly boost screening rates, leading to earlier detection and improved outcomes for cervical cancer treatment.
All SR and MA included in this umbrella review failed to explore other important barriers, such as psychological barriers (anxiety, embarrassment or shyness, fear of pain, fear of test results), structural barriers (lack of time, location of screening services, lack of transportation, accessibility of screening services, and preference for the gender of the HCP), socio-cultural and religious barriers (lack of social support, lack of family and spousal support, trust in God), and other barriers like myths and misconceptions that may have significantly influenced CCS uptake.
The strength of this review is its applicability to the entire country of Ethiopia, as the studies included in the SR and MA came from all regions. However, there is no similar umbrella review in Ethiopia or sub-Saharan countries. Consequently, the findings of this review were compared to systematic reviews and meta-analyses conducted in high-income countries and country-level studies, which could be a significant limitation.
Conclusion
The result of this umbrella review showed a low-level CCS utilization compared to WHO’s CCa elimination target. Factors like inadequacy of knowledge about CCA and CCS, history of having STIs, history of having multiple sexual partners, age of women, perception of susceptibility to contract cervical cancer, getting advice from healthcare providers, women’s educational status, and attitudes toward up taking CCS were explored and significantly associated with CCS uptake. But all of the reviews failed to explore other variables, such as psychological barriers (anxiety, embarrassment or shyness, fear of pain, fear of test results), structural barriers (lack of time, location of screening services, lack of transportation, accessibility of screening services, and preference for the gender of the HCP), socio-cultural and religious barriers (lack of social support, lack of family and spousal support, trust in God), and other barriers like myths and misconceptions that may have significantly influenced CCS uptake.
Healthcare providers should provide health education to increase women’s awareness and level of knowledge so that the women will understand the benefits of early screening utilization. We recommend researchers explore the barriers like psychological, structural, sociocultural and religious and other barriers like myths and misconceptions that may have significantly influenced CCS uptake and designing interventions to reduce the influence of these barriers on CCS uptake is crucial.
Supplemental Material
Supplemental Material - Cervical Cancer Screening Utilization and Barriers to Uptake in Ethiopia: An Umbrella Review
Supplemental Material for Cervical Cancer Screening Utilization and Barriers to Uptake in Ethiopia: An Umbrella Review by Ebrahim Mohammed, Girma Taye, Mathewos Assefa, Haji Aman, Adamu Addissie, and Ahmedin Jemal in Cancer Control.
Footnotes
Acknowledgments
We, the authors, want to acknowledge the authors of the systematic reviews and meta-analyses included in this review.
Author Contributions
Ebrahim Mohammed, Girma Taye, Adamau Addissie, Ahmedin Jemal, and Mathewos Assefa participated from conceptualization to manuscript writing. Haji Aman participated from data extraction, data analysis, and manuscript writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.