
Abstract
Background
With the use of immune-checkpoint inhibitors (ICIs) in advanced or metastatic non-small cell lung cancer (NSCLC), whether ICIs or chemotherapy is more effective still remains controversial. This study was conducted to evaluate the efficacy of programmed cell death 1 (PD-1), programmed cell death ligand 1 (PD-L1), cytotoxic T-lymphocyte protein 4 (CTLA-4) alone or in their combination vs chemotherapy in patients with advanced or metastatic NSCLC.
Methods
This meta-analysis was conducted from PubMed, Web of Science, Medline, Embase, and the Cochrane Library up to March 2021 to identify relevant randomized controlled trials. Primary endpoints were overall survival (OS) and progression-free survival (PFS). Secondary endpoint was adverse events (AEs). This meta-analysis’s Prospero registration number is CRD42022323570.
Results
The search process has identified 13 studies containing 7918 patients with advanced or metastatic NSCLC. The benefit of PD-1/L1 or CTLA-4 inhibitors alone or in combination compared with chemotherapy for advanced or metastatic NSCLC was elucidated in both OS [HR = .75, 95% CI (.70-.80), P < .001] and PFS [HR = .83, 95% CI (.73-.95), P < .001]. Besides, ICIs were associated with fewer AEs compared to chemotherapy.
Conclusion
PD-1/L1 or CTLA-4 inhibitors alone or in combination, with fewer AEs, was associated with significant improvements in terms of OS and PFS than chemotherapy in advanced or metastatic NSCLC.
Introduction
Lung cancer is the second most commonly diagnosed cancer and the leading cause of cancer-related death in 2020, to be more precise, the diagnosis rate was approximately 1 in 10 (11.4%), and the mortality rate was nearly 1 in 5 (18.0%) deaths worldwide. Additionally, about 85% of the lung cancer patients had what so called non-small cell lung cancer (NSCLC), which is one of the histological subtypes of lung cancer. NSCLC can be further sub-categorized into squamous cell carcinoma, adenocarcinoma and large cell carcinoma. About 75% of NSCLC patients are already in advanced or metastatic stage when they are diagnosed, and the 5-year survival rate is unfortunately low. 1
Applying cisplatin-based chemotherapy is currently the standard treatment guideline for advanced or metastatic NSCLC patients. However, the survival outcome was still disappointing. 2 Thus, improvements in treatment guideline for patients with advanced or metastatic NSCLC are urgently needed. With the use of immune checkpoint inhibitors (ICIs) in advanced or metastatic NSCLC, a number of studies have shown that the therapeutic effect of combine ICIs in chemotherapy is superior compared with conventional chemotherapy only, but the improvement is at the cost of increased adverse events (AEs). 3 The best-known ICIs are programmed cell death 1 (PD-1), programmed cell death ligand 1 (PD-L1), and cytotoxic T-lymphocyte protein 4 (CTLA-4). Herein, we investigated the efficacy and safety of adding PD-1/L1 or CTLA-4 inhibitors alone and the combination (PD-1/L1 + CTLA-4) compared with only giving chemotherapy in patients with advanced or metastatic NSCLC.
Materials and Methods
Search Strategy
This meta-analysis was conducted from PubMed, Web of Science, Medline, Embase, and the Cochrane Library as of March 2021 to find relevant studies. A combination of free text words and medical subject words was used to complete the subtopic search. Search criteria includes (“nivolumab” OR “ipilimumab” OR “sintilimab” OR “tislelizumab” OR “cemiplimab” OR “camrelizumab” OR “BMS 936558” OR “BMS 936559” OR “pembrolizumab” OR “lambrolizumab” OR “MK 3475” OR “pidilizumab” OR “CT 011″ OR “durvalumab” OR “MEDI 4736” OR “atezolizumab” OR “MPDL 3280a” OR “avelumab” OR “AMP 224” OR “PD-1” OR “PD-L1” OR "B7-H1” OR “CD274” OR “programmed death 1” OR “programmed death ligand 1” OR “CTLA-4 Antigen” [Mesh]) AND (“lung tumor” OR “lung cancer” OR “lung carcinoma” OR “lung neoplasm” OR “lung malignancy” OR “lung sarcoma” OR “Lung Neoplasms” [Mesh] OR “Carcinoma, Non-Small-Cell Lung” OR “squamous cell lung carcinoma” OR “lung adenocarcinoma” OR “large cell lung carcinoma”). Two researchers independently screened the titles, abstracts, and references of the retrieved articles. This meta-analysis’s Prospero registration number is CRD42022323570.
Study Selection and Quality Assessment
Studies that were included meet the following criteria. (a) Type of literature: Phase II/III randomized controlled trials (RCTs); (b) Patients involved in the study were diagnosed with advanced or metastatic NSCC; (c) The intervention group was treated only with PD-1/L1 or CTLA-4 inhibitors alone or their combination. The control group was treated only with chemotherapy. (d) Data is available. Exclusion criteria are as follow. (a) Non-English articles; (b) Neoadjuvant therapy is involved in the treatment process; (c) The intervention group used immunotherapy in combination with other treatment methods, such as chemotherapy or radiotherapy; (d) Articles with the same research population. As for the last exclusion case, we analyzed the latest or most complete data available.
Methodological quality was assessed for the included clinical trials via the Cochrane Collaboration Tool. Each eligible study was appraised predominantly in six aspects: (a) the sequence generation; (b) allocation concealment; (c) blinding; (d) incomplete outcome data; (e) selective outcome reporting; (f) free of other bias. Risk of bias was assessed and categorized as “low risk”, “high risk” or “unclear risk”.
Data Extraction
The data for each study were extracted independently by two researchers. Unified opinions were reached by consulting a third researcher. The following information was used: (a) author, year of publication, treatment stage, intervention, medicine, follow-up time, and sample size; (b) patient gender, age, histological type of tumor, and PD-1/L1 tumor proportion score (TPS); (c) the primary outcome was overall survival (OS) and progression-free survival (PFS). The secondary outcome was AEs. This meta-analysis was conducted in accordance with the preferred report project guidelines provided by the Systematic Reviews and Meta-Analysis Protocol (PRISMA-P) 2015. 4
Data Analysis and Statistical Methods
Hazard ratios (HR) and 95% confidence intervals (CI) were calculated to support OS and PFS. Risk ratios (RR) and 95% CI were calculated to support AEs. I2 statistics were used to assess heterogeneity between studies. In order to investigate the sources of heterogeneity, predefined subgroup analyses were performed. Due to the complexity of control conditions and the diversity of therapeutic agents, random effects model was applied to improve the reliability of the results in this article. Sensitivity analysis was performed to verify the stability of the results. Egger’s test (P < .1) was used to evaluate publication bias. All the above meta-analyses were performed via Stata SE Version 12 (Stata Corporation). All the above statistical tests were bilateral, and P < .05 was considered as a statistically significant difference in mentioned parameters.
Results
Eligible Studies
20309 relevant clinical records were generated based on the search strategy. After screening and qualification assessment, a total of 13 qualified phase II/III RCTs,5-17 including 7918 patients with advanced or metastatic NSCLC, were selected to complete this meta-analysis. The detailed investigation and research selection process was shown in Figure 1. Meanwhile, the PRISMA checklist for our meta-analysis is given in Supplementary Table 1. A schematic flow for the selection of articles included in this meta-analysis.
Study Characteristics and Quality
Characteristics of Included Clinical Trials in the Meta-Analysis.

NA: not available; TPS: PD-1/L1 tumour proportion score.
Analysis of Overall Survival
OS was reported in all the included studies. Compared with chemotherapy alone, PD-1/L1 or CTLA-4 inhibitors alone or in combination (PD-1/L1 + CTLA-4) had been proved to be capable to prolong OS in patients with advanced or metastatic NSCLC [HR = .75, 95% CI (.70-.80), P < .001], as being detailly showed in Figure 2. PD-1/L1 or CTLA-4 inhibitors alone or in combination compared with chemotherapy alone could improve OS of patients both in the first [HR = .77, 95% CI (.70-.84)] and non-first line treatment [HR = .74, 95% CI (.67-.81)] (Table 2). As for different targets, PD-1 inhibitors [HR = .70, 95% CI (.64-.78)], PD-L1 inhibitors [HR = .80, 95% CI (.72-.88)], and PD-1/L1 + CTLA-4 inhibitors [HR .81, 95% CI (.68-.95)] have all improved the OS, and it seemed that the pharmacological effect of PD-1 inhibitors was more noticeable (Table 2). Among all of the relevant drugs, nivolumab [HR = .71, 95% CI (.62-.81)], pembrolizumab [HR = .72, 95% CI (.61-.85)], and atezolizumab [HR = .76, 95% CI (.66-.86)] had been used most commonly and all of them could extend OS in patients with advanced or metastatic NCSLC, compared with chemotherapy alone (Table 2). In all the included studies, both male [HR = .71, 95% CI (.63-.81)] and female [HR .80, 95% CI (.68-.94)] could benefit from PD-1/L1 or CTLA-4 inhibitors alone or their combination (Table 2). Six studies collaboratively showed both patients <65 years [HR = .74, 95% CI (.66-.82)] and patient ≥65 years [HR = .76, 95%CI (.65-.89)] could get a prolonged OS with PD-1/L1 or CTLA-4 inhibitors alone or their combination compared with chemotherapy alone (Table 2). PD-1/L1 and CTLA-4 inhibitors showed a greater improvement in OS than chemotherapy not only in patients with advanced or metastatic squamous NSCLC [HR = .76, 95% CI (.67-.87], but also in patients with advanced or metastatic non-squamous lung cancer [HR = .66, 95% CI (.58-.76)] (Table 2). In these included studies, with PD-1/L1 or CTLA-4 inhibitors alone or their combination, both group of patients, with TPS ≥.01 [HR = .76, 95% CI (.71-.82)] and TPS < .01 [HR = .75, 95% CI (.58-.97] respectively, had a longer OS compared with patient group who were given chemotherapy only (Table 2). Forest plot of comparison: overall survival of PD-1/L1 or CTLA-4 inhibitors alone or in combination vs chemotherapy for advanced or metastatic non-small cell lung cancer patients (P < .001). Subgroup Analysis of Overall Survival. HR: hazard ratio; CI: confidence interval; TPS: PD-1/L1 tumour proportion score.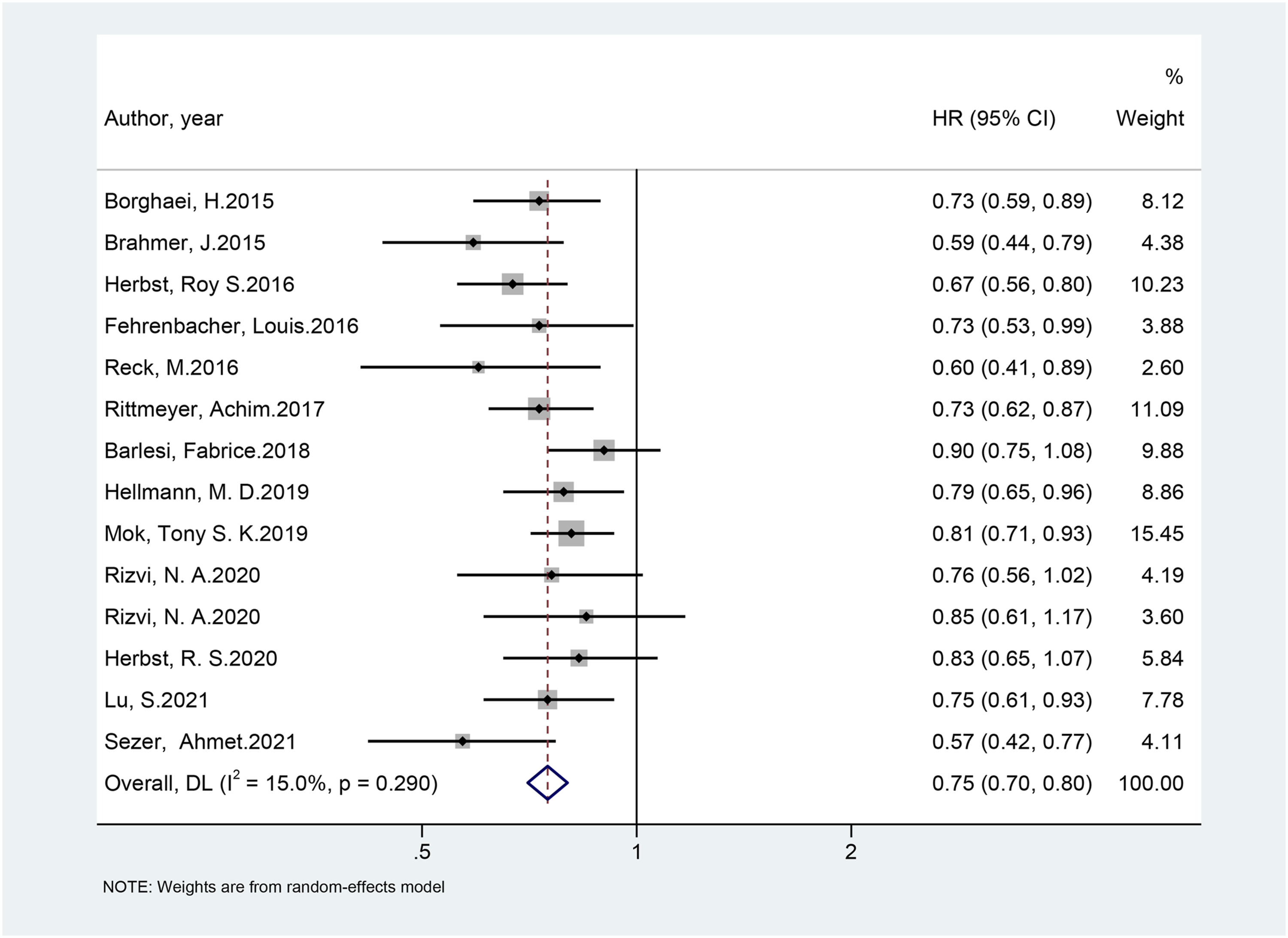

Analysis of Progression-Free Survival
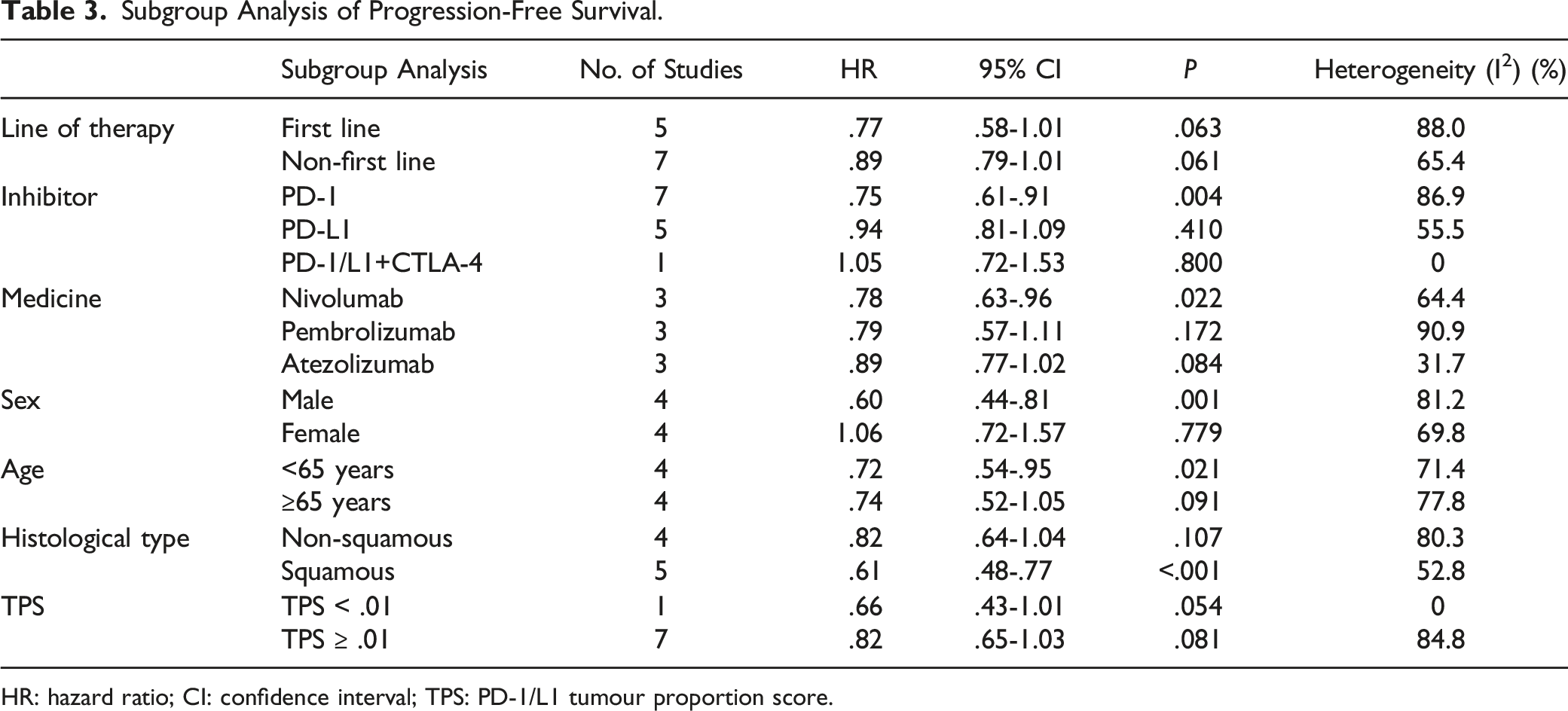
PFS was reported in 12 studies. Similar to OS, giving PD-1/L1 or CTLA-4 inhibitors alone or in combination resulted better in PFS than applying chemotherapy alone in patients with advanced or metastatic NSCLC [HR = .83, 95% CI (.73-.95), P < .001] (detailed data are shown in Figure 3). PD-1/L1 or CTLA-4 inhibitors alone or in combination was directly related to better clinical efficacy in both first-line [HR = .77, 95% CI (.58-1.01)] and non-first line treatment [HR = .89, 95% CI (.79-1.01)] (Table 3). Among PD-1 [HR = .75, 95% CI (.61-.91)], PD-L1 [HR = .94, 95% CI (.81-1.09)] and PD-1/L1+CTLA-4 [HR = 1.05, 95% CI (.72-1.53)] inhibitors, only PD-1 has showed a statistically significant improvement, comparing with chemotherapy alone, in PFS in patients with advanced or metastatic NSCLC (Table 3). As for nivolumab [HR = .78, 95% CI (.63-.96)], pembrolizumab [HR = .79, 95% CI (.57-1.11)], and atezolizumab [HR = .89, 95% CI (.77-1.02)], only nivolumab has demonstrated a statistically significant improvement in PFS in advanced or metastatic NSCLC patients compared to chemotherapy alone (Table 3). In the study of PFS, only male patients [HR = .60, 95% CI (.44-.81)] who had received treatment with PD-1/L1 or CTLA-4 inhibitors alone or in their combination achieved better treatment outcomes than chemotherapy alone eventually. Female [HR = 1.06, 95% CI (.72-1.57)] patients, on the other hand, have indicated no statistically significant improvement (Table 3). When it comes to different age groups, PD-1/L1 or CTLA-4 inhibitors alone or their combination improved the efficacy of PFS both in patients <65 years [HR = .72, 95% CI (.54-.95] and ≥65 years [HR = .74, 95% CI (.52-1.05)]. However, the difference was not statistically significant in the ≥65 years age group (Table 3). As for histological types, both patients with squamous [HR = .61, 95% CI (.48-.77)] and patients with non-squamous [HR = .82, 95% CI (.64-1.04] had a longer survival if they were given PD-1/L1 or CTLA-4 inhibitors alone or in their combination comparing to those who had received chemotherapy alone. However, only patients with squamous subtype had statistically significant improvement in treatment outcomes (Table 3). In these included studies, comparing pharmacological treatment with PD-1/L1 or CTLA-4 inhibitors alone or in combination with chemotherapy alone, there was a better prognosis in terms of PFS in patients with TPS ≥.01 [HR = .82, 95% CI (.65-1.03)] and patients with TPS <.01 [HR = .66, 95% CI (.43-1.01], though the difference is not statistically significant (Table 3). Forest plot of comparison: progression-free survival of PD-1/L1 or CTLA-4 inhibitors alone or in combination vs chemotherapy for advanced or metastatic non-small cell lung cancer patients (P < .001). Subgroup Analysis of Progression-Free Survival. HR: hazard ratio; CI: confidence interval; TPS: PD-1/L1 tumour proportion score.
Analysis of Adverse Events
Subgroup Analysis of the Most Common Adverse Events.

Publication Bias and Sensitivity Analysis
When it comes to OS, no significant publication bias was elucidated via Egger’s test (P = .126, Supplementary Figure 1), and sensitivity analysis indicated that the result was insensitive to the included studies (Supplementary Figure 2). As for PFS, Egger’s test showed that there was no statistically significant publication bias (P = .1, Supplementary Figure 3), and sensitivity analysis indicated that the result was insensitive to included studies (Supplementary Figure 4).
Discussion
With the gradual application of ICIs in treating advanced or metastatic NSCLC, the awareness of ICIs’ efficacy has been widely raised by scientists and researchers. Previous studies have shown that ICIs combined with chemotherapy can effectively improve survival in patients with advanced or metastatic NSCLC compared to single treatment of conventional chemotherapy, suggesting that ICIs are really effective in patients with advanced or metastatic NSCLC. 18 But the efficacy of ICIs vs conventional chemotherapy remains controversial.
PD-1/L1 inhibitors and CTLA-4 inhibitors are considered as the promising ones of ICIs at present. Herein, the meta-analysis was conducted to evaluate the efficacy of PD-1/L1 or CTLA-4 inhibitors alone or in combination (PD-1/L1 + CTLA-4) vs conventional chemotherapy in patients with advanced or metastatic NSCLC, setting up PFS as and OS as primary endpoints and AEs as secondary endpoints. The results suggested that PD-1/L1 or CTLA-4 inhibitors alone or in combination can improve OS as well as PFS and these advantageous outcomes are in relationship with fewer AEs in patients with advanced or metastatic NSCLC compared to conventional chemotherapy. The results also elucidated that patients can benefit differently from ICIs depending on their disease subgroups. Sensitivity analysis indicated that the results is in good stability.
The pharmacological mechanism of ICIs had been discovered in several studies and has been confirmed in clinical studies. PD-1/L1 inhibitors can block the competitive binding of PD-1 and PD-L1, resulting in the up-regulation T cells in terms of growth and proliferation. This up-regulation leads to the improvement in T cells’ recognition to tumor cells, then activates the immune function, to be more precise, attack and specifically kill tumour cells. In other words, the anti-tumor effect of ICIs is achieved by mobilizing the body’s own immune function. Several preclinical studies 19 have shown that blocking CTLA-4 can restore the activity of T cells and drastically prolong the survival time of memory T cells, hence restoring the body’s immune function against tumor cells and improving the control rate of tumor. One of the biggest advantages of using immunotherapy over chemotherapy is that the pharmacological effect of immunotherapy can be long-lasting. In melanoma, a large number of super-survivors have a more than 10-year survival after clinical intervention and are clinically cured. Furthermore, in the study of Yixin Zhou, 3 PD-1/PD-L1 inhibitor plus chemotherapy, compared with chemotherapy, has contributed to improved PFS and OS in first-line therapy in NSCLC, but at the expense of increase in treatment-related AEs. However, in this research, PD-1/L1 or CTLA-4 inhibitors alone or in combination seemed to merit over chemotherapy alone not only in promoting survival time but also in reducing drug AEs in NSCLC patients. To conclude, patients with advanced or metastatic NSCLC seem to benefit more from ICIs compared to conventional chemotherapy.
Obviously, the effect of ICIs depends on the how functional the patient’s autoimmune system is, which may be related to treatment lines. Herein, the first-line immunotherapy appears to be more helpful improving PFS in patients compared to the non-first line ICIs. The research results of Ma Amrein 20 et al show that traditional platinum-contained chemotherapy would have negative impact on the immune microenvironment. Therefore, patients with different treatment lines would have different cell signaling process depending on their autoimmune function due to different times of treatment. To conclude, immunotherapy seems to be very promising on the first line because repeated use of chemotherapy would make more immune compromised patients, which is harmful and a potential burden to national health system. The immune function is the most vital factor that need to be considered when deciding whether the first-line treatment of NSCLC patients should be chemotherapy or immunotherapy.
In addition, previous studies have suggested that the efficacy of ICIs is associated with TPS of patients. It is generally believed that TPS has a predictive effect on the efficacy of ICIs in NSCLC patients. 21 Unfortunately, this trend has not been found here. This may result from the small sample size in research process, especially for the subgroup analysis with TPS < .01. Common thresholds for TPS classification include 1%, 50%, etc., so another rational assumption is that the dissimilarity may due to the not appropriate threshold for grouping scheme which is 1% in this study. Since distinction in classification criteria of defining high and low expression of TPS may lead to different therapeutic effects as well as prognosis judgment, it is very necessary to determine a recognized and effective classification threshold.
No matter first-line or second-line treatment for advanced or metastatic NSCLC, there are promising PD-1 inhibitors and PD-L1 inhibitors in clinical treatment. Previous studies have shown that the effect of PD-1 inhibitors and PD-L1 inhibitors in improving OS, in patients with NSCLC, are similar. 22 However, in this study, the effects of the different inhibitors seemed to result differently in prognosis. Undeniably, it is reasonable to suspect the advantage of ICIs due to the lack in enough RCTs being conducted with PD-L1 inhibitors. But among the most commonly used three ICIs, nivolumab, pembrolizumab, and atezolizumab, both PD-1 inhibitors (nivolumab and pembrolizumab) have better pharmacological effects than the PD-L1 inhibitor (atezolizumab). We seemed to have reached the same conclusion that PD-1 inhibitors are more promising in treating patients with advanced or metastatic NSCLC. Theoretically, PD-1 antibody can bind to PD-1 protein on T cells’ cell membrane. This process will block the binding between PD-1 and PD-L1/PD-L2 at the same time. PD-L1 antibody, however, can only interact with PD-L1 and specifically block the binding between PD-1 and PD-L1. Therefore, T cells might still be inhibited by the interaction between PD-1 and PD-L2 using anti-PD-L1 treatment. 23 All above proved the presumed theory that PD-1 inhibitors showed greater potential than PD-L1 inhibitors in treating patients with advanced or metastatic NSCLC, which may be related to the subtle differences in the mechanism of action between PD-1 antibodies and PD-L1 antibodies. Due to the inadequate number of studies, the efficacy of PD-1/L1 inhibitors combined with CTLA-4 inhibitors and PD-1/L1 inhibitors can not be accurately compared.
The therapeutic effect of ICIs is influenced not only by drug types, but also by the biological characteristics of patients, including male and female. Compared to no significant differences being observed between age subgroups, the distinction between genders is obvious. Male with advanced or metastatic NSCLC appears to benefit more from ICIs than the female in this study. There may be several rational reasons leading to this dissimilarity. Firstly, the incidence of tumor histology of NSCLC in male and female are different, to be more detailed, female is more likely to be diagnosed with adenocarcinoma, 24 which is more sensitive to chemotherapy than squamous NSCLC. 25 Hence, female tends to benefit less than male in treatment with ICIs. Moreover, some other studies have revealed the potential impact of estrogen on tumor development. The estrogen content in females was significantly higher than that in males. As for women in different ages, the therapeutic effect can be difference as well. Survival of postmenopausal female undergoing chemotherapy is better, but premenopausal female tends to have a worse prognosis than postmenopausal female and the male. 26 Besides, several studies have suggested that estrogen upregulates both PD-1 and PD-L1 and may play an important role in the PD-1 /PD-L1 signal pathway.27,28 These sex-based immunological differences may be the reason why the male in this study benefits more from ICIs than female. Therefore, how sex affects the therapeutic effect of immunotherapy in cancer treatment is what need to be focused in future studies.
Encouragingly, in addition to therapeutic efficacy, ICIs also outperform conventional chemotherapy in terms of AEs in treatment of advanced or metastatic NSCLC. In this study, comparing with conventional chemotherapy, ICIs not only obviously improve survival time in patients with advanced or metastatic NSCLC, but also decrease the incidence of a majority of AEs. In this analysis, most RCTs chose paclitaxel or platinum as chemotherapy agents. According to previous studies, although paclitaxel and docetaxel are clinically active in NSCLC chemotherapy, they are problematic due to relating severe dose-limiting toxicity, the most prominent among which is neutropenia.29,30 In this research, PD-1/L1 or CTLA-4 inhibitors alone or in combination significantly decreased the incidence of neutropenia compared to the incidence of that in patients treated with chemotherapy. On the other hand, PD-1/L1 or CTLA-4 inhibitors alone or in combination is associated with a higher incidence of rashes, which may be related to immunologic derangement. But there was no significant difference in the incidence of severe rash between treatment groups with immunotherapy or chemotherapy. Overall, the incidence of adverse reactions in patients’ NSCLC treatment is lower in immunotherapy than in chemotherapy.
Similarly, the study of Ferrara, R. 31 suggests that single-agent ICI in people with NSCLC and PD-L1 ≥ 50% probably leads to a higher overall survival rate and may lead to a higher progression-free survival and overall response rate when compared to platinum-based chemotherapy and may also lead to a lower rate of adverse events. On the one hand, our study yielded supportive findings. On the other hand, through the rich subgroup analyses, we found that the advantage of immunotherapy over chemotherapy alone persisted in each subgroup analysis. Therefore, the therapeutic promise of immunotherapy alone in advanced NSCLC may be very substantial. Immunotherapy alone may be a good option for patients with advanced NSCLC who do not tolerate immunization plus chemotherapy.
There are some limitations in this study. First of all, the sample sizes of included studies were not exactly same. Studies with small sample sizes may be one of the limits in the credibility of results. Secondly, some important gene mutation indicators, such as epidermal growth factor receptor and anaplastic lymphoma kinase, have been reported to be essential in affecting the therapeutic effect of PD-1/L1 inhibitors. Unfortunately, the related analysis is failed to be performed due to insufficient data. Moreover, most of the patients enrolled in this meta-analysis were from the West, and numerous parallel studies in Asia and other regions are in need. Of course, in order to explore the efficacy of PD-1/L1 or CTLA-4 inhibitors alone or in combination more comprehensively, more studies and analyses should be conducted to compare with other mainstream therapies such as radiotherapy.
Conclusion
To sum up, PD-1/L1 or CTLA-4 inhibitors alone or in combination have a better therapeutic effect and fewer AEs than conventional chemotherapy in patients with advanced or metastatic NSCLC. But the accurate therapeutic effect varies among different subgroups, such as different sex groups. These findings have a positive impact on the promising application of ICIs and are important in clinical practice when it comes to giving patients advice and helping clinicians decide appropriate treatment options.
Supplemental Material
Supplemental Material - PD-1/L1 With or Without CTLA-4 Inhibitors Versus Chemotherapy in Advanced Non-Small Cell Lung Cancer
Supplementary Material for PD-1/L1 With or Without CTLA-4 Inhibitors Versus Chemotherapy in Advanced Non-Small Cell Lung Cancer by Luyong Guo, Jiali Liang, Wei Dai, Jiayu Li, Yuexiu Si, Wei Ren, Yan Lu, and Danqi Chen in Cancer Control.
Supplemental Material
Supplemental Material - PD-1/L1 With or Without CTLA-4 Inhibitors Versus Chemotherapy in Advanced Non-Small Cell Lung Cancer
Supplementary Material for PD-1/L1 With or Without CTLA-4 Inhibitors Versus Chemotherapy in Advanced Non-Small Cell Lung Cancer by Luyong Guo, Jiali Liang, Wei Dai, Jiayu Li, Yuexiu Si, Wei Ren, Yan Lu, and Danqi Chen in Cancer Control.
Footnotes
Author Contributions
Each author contributed significantly to concept and development of the present paper. LYG and DQC designed the research process. JLL and WD searched the database for corresponding articles and extracted useful information from the articles above. JYL and YXS used statistical software for analysis. WR and YL drafted the meta-analysis. All authors had read and approved the manuscript and ensured that this was the case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Data supporting findings reported in this study are available in the supplementary materials.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.