
Abstract
People living with HIV (PLWH) have an increased risk of lung cancer compared to the general population. In 2013, the United States Preventive Services Task Force (USPSTF) released their lung cancer screening (LCS) guidelines. However, the impact of these guidelines has not been well established in PLWH. The objective of this retrospective descriptive study is to evaluate the frequency of lung cancer screening referrals and factors associated with LCS referrals using the 2013 USPSTF screening guidelines in at-risk PLWH. We collected demographic and clinical information on PLWH from electronic medical records from July 2016 to July 2018. Descriptive statistics, chi-square tests, t-tests, Wilcoxon rank sum tests, and Fisher’s exact tests were used for analysis. Only 14% of patients who met 2013 USPSTF screening guidelines were referred for screening. Patients who received a referral were more likely to have received tobacco cessation counseling. Patients who received and completed a referral were more likely to have hepatitis C infection. Quality improvement strategies are needed to improve rates of LCS in PLWH.
Keywords
Introduction
The introduction of combination antiretroviral therapy (cART) has led to a decrease in morbidity and mortality from Human Immunodeficiency Virus (HIV). In the United States, treatment with cART in people living with HIV (PLWH) has led to a near-normal life expectancy. 1 As PLWH live longer, there has been an increased incidence of chronic and age-related diseases, such as malignancy and specifically non-AIDS defining cancers (NADCs) as compared to the pre-antiretroviral era. 2 The risk for NADCs among PLWH varies from an increase of 2- to 5-fold for melanoma, lung cancer, and hepatocellular carcinoma and up to 10- to 30-fold for Hodgkin’s lymphoma and anal cancer relative to the general population. Additionally, other prevalent risk factors in PLWH may contribute to the increased risk for specific cancers, such as smoking, alcohol consumption, human papillomavirus (HPV) infection, and hepatitis C (HCV) infection. 3
Lung cancer is a common NADC diagnosis that occurs at younger ages, progresses rapidly, is diagnosed mostly in later stages, and has increased mortality in PLWH. 4 While the main risk factor is likely increased tobacco use, HIV infection itself may be an independent risk factor for the development of lung cancer. 5 HIV infection can also lead to immune system dysfunction and a state of chronic inflammation. 6 In addition, a decreased immunological defense system may lead to recurring infections, such as bacterial pneumonia, which can further contribute to chronic inflammation. 7 Both of these immunological and infectious factors are associated with the development of lung cancer in PLWH. 8 As lung cancer becomes prevalent in PLWH, it is imperative that providers focus on diagnostic strategies to decrease the overall morbidity and mortality.
Smoking cessation is an essential intervention in the prevention of lung cancer and is required by Medicare for all current smokers, including PLWH. Smoking is highly prevalent among PLWH with 50–70% reporting smoking cigarettes daily compared to 17.8% of the United States general adult population. 9 Many PLWH have contemplated smoking cessation (60–70%) or have tried to stop at least once (50–75%). 10 Smoking cessation could lead to a 34% decreased risk of development of NADCs, including lung cancer. 11 The European AIDS Clinical Society (EACS) has recently established smoking cessation guidelines specifically for PLWH. 12
In addition to smoking cessation, lung cancer screening (LCS) is an important tool in assessing at-risk PLWH. The U.S. Preventive Services Task Force (USPSTF) released LCS recommendations in 2013 which have been recently updated in March 2021. Their 2013 recommendations called for an annual screening for lung cancer with low-dose computed tomography in patients 55 to 80 years of age who have a 30 pack-year smoking history and who currently smoke or have quit within the past 15 years. 13 The updated recommendations for 2021 include expanding both the age range (50 to 80 years of age) and pack-year history (20 pack-years). 14 Given that PLWH are at an increased risk for lung cancer, it is vital to identify methods for implementation of LCS as part of primary HIV care. HIV clinics provide comprehensive care to PLWH including screening for hepatitis, tuberculosis, sexually transmitted diseases, and cancer including cervical cancer. For federally funded clinics, these services are usually tracked and reported to the HIV and AIDS Bureau as part of annual measures. However, there is a paucity of data on the current state of LCS in PLWH in the United States. We therefore conducted a retrospective study to determine the frequency of and factors associated with LCS using the 2013 USPSTF guidelines in at-risk PLWH.
Materials and Methods
We conducted a retrospective chart review study of PLWH who were identified as potential candidates for LCS between July 1, 2016, and July 1, 2018. Initial screening included patients aged 55–80 with a confirmed diagnosis of HIV, who were actively receiving care at a Midwestern HIV clinic associated with an academic hospital, to establish continuity of care at the clinic. Exclusion criteria consisted of those who had never smoked, were deceased, had an unknown smoking pack-year history, and/or a prior lung cancer diagnosis. Universal sampling included all patients during this period who met inclusion/exclusion criteria were included.
We then divided the patients into 2 groups: those who met the 2013 USPSTF Lung Cancer Screening guidelines of being 1) an adult aged 55–80, 2) had a 30-pack-year smoking history, currently smoking or quit within the past 15 years, and 3) were in good health and can have curative lung surgery and those who did not meet the 2013 USPSTF LCS guidelines (Figure 1). Both groups were included for additional analysis. Flow Chart of Lung Cancer Screening Criteria.
Information obtained from the electronic medical record included the following: demographic information such as age, sex, race/ethnicity, HIV risk factor, and federal poverty level (FPL); clinical information including comorbid diabetes, hypertension, cardiovascular disease, current or history of hepatitis B and/or C, liver disease, and kidney disease was obtained based on corresponding ICD-10 codes; substance use information including tobacco use, history, and quit date, whether they had received tobacco cessation counseling, alcohol use, and illicit drug use; and HIV-related information such as date of HIV diagnosis and laboratory information including most recent HIV viral load and CD4 T-cell count. In addition to automatic prompts to screen for and record smoking status in the electronic medical records system, medical providers in our clinic conduct tobacco cessation counseling during each medical visit. Patients who express an interest in quitting are referred to the clinical pharmacist for continued counseling, follow-up, and pharmacological management. All patient information obtained was de-identified. We collected information on LCS referrals including the provider who ordered the screening and the status of completion of screening during the aforementioned time period. The American College of Radiology Lung-Reporting and Data System (Lung-RADS) recommendations were used for assessment and management after completion of initial LCS in those who met 2013 USPSTF LCS guidelines. 15 The study was approved by the institutional review board.
Subjects were divided into groups for comparison based on whether they received a screening referral. A screening referral is made after a shared-decision visit between the patient and provider to proceed with a low-dose CT for further evaluation. Those who were given a screening referral were further divided by whether they completed the screening. Groups were initially compared on age, sex, sexual orientation, race, poverty level, insurance status, alcohol and other substance use, smoking history, comorbidities, CD4 T-cell count, HIV viral load, duration of HIV, and frequency of healthcare visits using descriptive statistics. Differences between those who were given a referral or not were evaluated using Wilcoxon rank-sum tests and either chi-square tests or Fisher’s exact tests, as appropriate. Differences between those who did and did not complete screening after receiving a referral were compared using either Fisher’s exact tests or Wilcoxon rank-sum tests. All analyses were completed using STATA version 16.1 (StataCorp, College Station, TX).
Results
Of 347 patients included based on initial screening criteria, 91 patients were excluded because of having never smoked (8), were deceased (38), had an unknown smoking pack-year history (39), and/or a prior lung cancer diagnosis (6). Of the remaining 256 patients, the mean (SD) for age was 61(5) with an age range of 55–78. There were 104 patients (41%) who met the 2013 USPSTF lung cancer screening recommendations while the other 152 patients did not. Regardless of whether patients met USPTSF criteria, 22/256 (9%) of patients had a screening/referral order with 12/22 (55%) being completed. Patients who completed low-dose computed tomography (LDCT) 12/256 (4.7%) were considered as having completed LCS. In patients who did not meet USPTSF criteria, 8/152 (5%) had a screening/referral ordered with 2/8 (25%) being completed. In patients meeting USPTSF criteria, 14/104 (14%) had a screening/referral ordered with 10/14 (71%) being completed. Of those 10 that were completed, 2 (20%) were classified as “Negative,” while the other 8 (80%) were “Other” and consisted of 2 “Category Lung-RADS 1,” 5 “Category Lung-RADS 2,” and 1 “Category Lung-RADS 3”. An infectious disease provider ordered 12 (55%) screenings while a non-infectious disease provider ordered 10 (45%).
Demographic and Clinical Characteristics of Patients Who Received Lung Cancer Screening Referral.

All tests are chi-square tests except as noted.
Abbreviations: MSM; men who have sex with men, FPL; federal poverty level, VA; Tricare/Veterans Administration, RW; Ryan White Part C—a federal grant that is awarded to HIV clinic.
aas of July 1, 2018.
bWilcoxon rank-sum test.
cFisher’s exact test.
Demographic and Clinical Characteristics of Patients Referred and Completed Lung Cancer Screening.
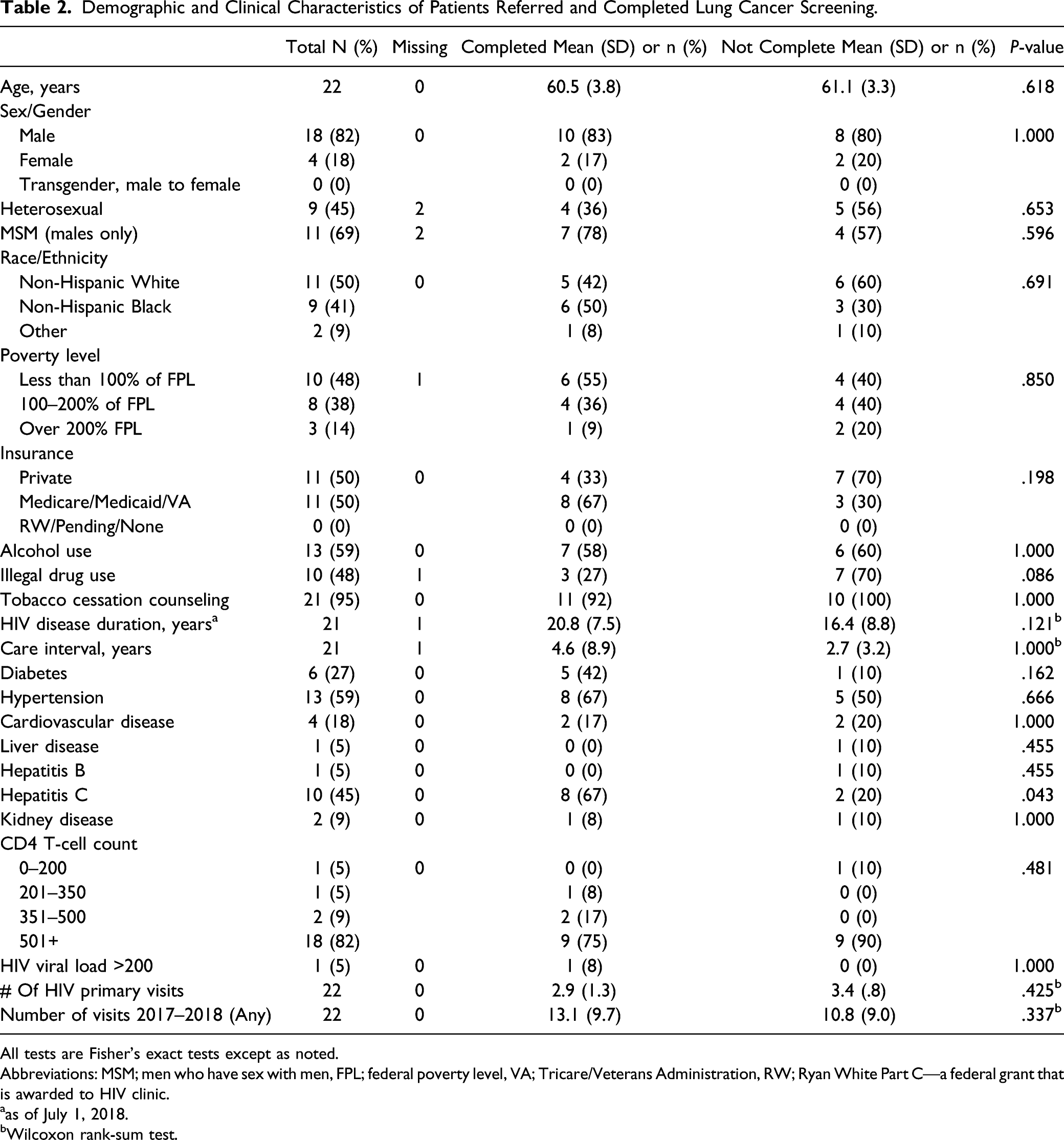
All tests are Fisher’s exact tests except as noted.
Abbreviations: MSM; men who have sex with men, FPL; federal poverty level, VA; Tricare/Veterans Administration, RW; Ryan White Part C—a federal grant that is awarded to HIV clinic.
aas of July 1, 2018.
bWilcoxon rank-sum test.
Discussion
Our study evaluated the factors associated with referral and completion of LCS in PLWH in a Midwestern HIV clinic. Our main finding was a low rate of LCS referral and completion in PLWH. In addition, tobacco cessation counseling was associated with increased rates of LCS referral. Interestingly, hepatitis C infection was associated with both increased rates of LCS referral and completion. Identification of factors associated with LCS is important as it can aid in development of strategies to improve LCS in PLWH.
In this retrospective study, we evaluated PLWH who received LCS referral and those who completed referral. Two groups were established: patients who met and those who did not meet the 2013 USPSTF guidelines. Lung cancer screening referrals and completion were low in both groups with slightly higher referral rate in those who met the 2013 USPSTF guidelines. Lung cancer screening rates in PLWH are not well characterized compared to the general population. The National Lung Cancer Screening trial evaluated LCS for detection of malignancy and mortality reduction in the general population. 16 This data was later used for development of the 2013 USPSTF guidelines. However, after implementation there have been limited data on the rates of LCS. In 2016, an analysis of the Lung Cancer Screening Registry was conducted to determine the rates of screening in the general US population who met the 2013 USPSTF recommendations. The rates for LCS were 2.0% in the general population and 2.1% in the Midwest. 17 Compared to the general population in the Midwest, our clinic population had an increased rate of LCS (2% vs 10%) in PLWH who met the 2013 USPSTF LCS guidelines. Engagement in healthcare among PLWH is greater than the general population. However, the rates among both groups are low and highlight the need for an emphasis in preventative care in general and specialty care medicine. Nevertheless, adherence to LCS recommendations in PLWH remains low and warrants further investigation to identify barriers to screening referral and completion.
Lung cancer screening and tobacco cessation counseling are part of the lung cancer prevention and management paradigm. However, their utility and implementation are not well understood. Tobacco cessation counseling is addressed prior to LCS referral. The observed association between tobacco cessation counseling and referral for LCS suggests that these strategies are being utilized for LCS prevention (Table 1). A study by Cao et al suggested that there are more health benefits from intervention methods, such as cessation counseling, compared to screening alone. 18 Conversely, tobacco cessation counseling was not associated with completion of LCS. This is likely multifactorial including lack of patient adherence or provider follow-up during the screening process. However, these factors were not assessed in our study. Currently, the National Cancer Institute-Lung Population-based Research to Optimize the Screening Process Initiative is evaluating the use of cessation programs during LCS. 19 A study utilized an opt-out strategy during LCS where patients were able to see their provider and a tobacco treatment counselor during their visit, which led to increased referrals for LDCT and increased patient satisfaction with counseling services. 20 Ultimately, other barriers exist that prevent effective implementation of tobacco cessation during LCS, such as patient motivation and provider reimbursement, that future studies can provide further input into.
Patient demographic and clinical information were evaluated to identify specific factors that are associated with LCS referral and completion. Hepatitis C infection was significantly associated with referral and completion for LCS. Approximately a third of PLWH in the US have HIV/HCV co-infection. This population has an increased morbidity and mortality when compared to HIV or HCV mono-infections. 21 In addition, tobacco use in patients with HIV/HCV co-infection was significantly higher at 48% compared to the national rate of 14%. 22 Providers interacting with this population may focus on medical management of HIV/HCV co-infection to reduce morbidity and mortality. Specifically, during treatment for HCV, patients are more likely to interact with the medical system. The duration of treatment for HCV is approximately 12–24 weeks and thus leads to additional opportunities for healthcare maintenance management and follow-up, including LCS. 23 Overall, the association of HCV with LCS in our study may be multifactorial and requires further evaluation.
Important limitations of our study design are the relatively small sample size within a 2-year time period and retrospective collection of data from the electronic health record. Statistical analysis of a small sample size does not allow for multivariable analysis. It would be important to study robust HIV clinics and evaluate LCS rates and referral, including significant variables that may influence these two. In addition, this is a single center study and certain differences may be noted compared to other centers which does not allow for generalization of these results. Collection of data from the electronic health record may have limited our ability for effective assessment and evaluation. For example, data entry of tobacco use and history is self-reported and is entered by various healthcare professionals and can limit data quality and accuracy. Free text fields can lead to incorrectly recorded data about smoking pack-years or years since quitting in evaluation for LCS. 24 Therefore, LCS rates may be adversely affected due to under- or over-reported rates of pack-year history. In addition, we were not able to determine the status of hepatitis C whether it was a current or historic infection. Our study was conducted at a single academic medical center in the Midwest, and the results may not be generalizable to all PLWH. Lastly, we did not evaluate the patient’s beliefs and attitudes toward LCS and tobacco cessation counseling. Prior research has shown that patient-related barriers often impact adherence with LCS. Patients are less likely to participate in screening due to the associated financial burdens of screening, lack of education about lung cancer, concerns about radiation exposure from CT imaging, and if they are an active smoker. 25 In future studies, these limitations should be considered and evaluated to improve our understanding of LCS in PLWH.
As a result of this study, opportunities arise for quality improvement initiatives and continued research within our patient population for improved LCS. Integration of tobacco cessation counseling for prevention of and management during LCS can aid in reducing mortality in PLWH. Future studies should include assessment of patient’s attitudes and beliefs toward LCS and tobacco cessation counseling to determine which personal factors may be associated with LCS.
In conclusion, the rates of LCS in PLWH are inadequate and create an opportunity for quality improvement programs in HIV clinics. Currently, the 2021 USPSTF guidelines for LCS have expanded the inclusion criteria of patients recommended for screening. However, the guidelines used for the general population may not be sufficient for certain populations, such as PLWH who have increased risk for malignancy due to underlying disease factors. This discrepancy highlights the need for continued research in PLWH to determine if specific LCS guidelines may be needed in the future. Subsequently, providers must be aware of maintaining adherence to the current USPSTF guidelines to provide adequate and optimal care to at-risk PLWH. Overall, improving rates of LCS in PLWH is imperative as it is considered a standard of care for healthcare maintenance.
Footnotes
Acknowledgments
We thank Dr. Purnima Guda, PhD, for her assistance in collecting electronic medical record information; Matthew Anderson, MPH, for his assistance in development of a RedCAP data tool; and Deanna Hansen, for her administrative support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Department of Internal Medicine, University of Nebraska Medical Center.
Ethics Statement
Ethical approval to report this case was obtained from University of Nebraska Medical Center IRB (# 019-19-EP). All procedures in this study were conducted in accordance with the University of Nebraska Medical Center (# 019-19-EP) approved protocols. Informed consent for patient information to be published in this article was not obtained as the study was eligible for a waiver for informed consent due the only record linking the subject and the research would be the informed consent form and the principal risk would be potential harm resulting from a breach of confidentiality.