
Abstract
Despite guidelines recommending annual low-dose computed tomography (LDCT) screening for lung cancer, uptake remains low due to the perceived complexity of initiating and maintaining a clinical program—problems that likely magnify in underserved populations. We conducted a survey of community providers at Federally Qualified Health Centers (FQHCs) in Santa Clara County, California, to evaluate provider-related factors that affect adherence. We then compared these findings to academic providers’ (APs) LDCT screening knowledge, behaviors, and attitudes at an academic referral center in the same county. The 4 FQHCs enrolled care for 80 000 patients largely of minority descent and insured by Medi-Cal. Of the 75 FQHC providers (FQHCPs), 36 (48%) completed the survey. Of the 36 providers, 8 (22%) knew screening criteria. Fifteen (42%) FQHCPs discussed LDCT screening with patients. Compared to 36 APs, FQHCPs were more concerned about harms, false positives, discussion time, patient apathy, insurance coverage, and a lack of expertise for screening and follow-up. Yet, more FQHCPs thought screening was effective (27 [75%] of 36) compared to APs (P = .0003). In conclusion, provider knowledge gaps are greater and barriers are different for community clinics caring for underserved populations compared to their academic counterparts, but practical and scalable solutions exist to enhance adoption.
Introduction
Lung cancer is the second most common cancer, the deadliest, and a leading cause of life-years lost in the United States. 1,2 The 2011 National Lung Screening Trial (NLST) showed that chest low-dose computed tomography (LDCT) annually decreased lung cancer-associated mortality by 20% compared with chest x-ray (CXR) in high-risk patients. 3 Based on this, the US Preventive Services Task Force (USPSTF) issued a grade B recommendation for LDCT screening for lung cancer in 2014, 4 and the Centers for Medicare and Medicaid Services (CMS) began LDCT screening coverage in 2015. 5
The resources required for a successful clinical screening program have made implementation of LDCT screening challenging across a diverse group of health systems. 6 These include subspecialty coordination between providers and radiologists and structured reporting systems for CT results and patient follow-up. Additionally, education for referring providers and their patients alike is needed since primary care providers’ (PCP) knowledge, attitudes, and behaviors regarding LDCT screening may lead to low uptake, 7 -14 which are key barriers to implementation.
Santa Clara County (SCC), California, which includes the city of San Jose, has a population of nearly 2 million people, and 15% of this population lives in poverty. 15 From 2010 to 2014, the incidence of SCC lung cancer was 45.5 per 100 000 for non-Hispanic (NH) whites, 42.4 for blacks, 35.8 for Asians/Pacific Islanders, and 27.7 for Hispanics. 16 SCC has 8 primary care health professional shortage areas and 3 medically underserved areas/populations, areas designated by the Human Resources & Services Administration as having too few PCPs and high infant mortality, poverty, or elderly populations. 17 About 6% of patients younger than 65 years in SCC do not have health insurance, 15 which is less than the national average of 8.8% in 2016. 18 The adult smoking prevalence of SCC is 8.4%, 19 and although this is lower than surrounding counties and the national average, disparities do exist. The smoking prevalence in SCC among blacks and Hispanics is higher than NH whites, and this difference is greater for those with lower annual household incomes. 20 Medi-Cal, California’s Medicaid program, insures low-income adults (those at or below 138% of the federal poverty level), 21 seniors with disabilities, and covers lung cancer screening.
Differences in recommending lung cancer screening between academic and community physicians in SCC are not known, but based on other cancer screening programs like breast cancer, 22 we hypothesized it is lower in community populations. We therefore aimed to evaluate practice patterns and assess facilitators and barriers to lung cancer screening with LDCT by surveying SCC community providers and comparing these responses to a previous study examining those of academic providers (APs) in SCC. 23
Materials and Methods
To identify community partners, we first presented our proposal to the medical directors of the Community Health Partnership of SCC, 20 where we identified 4 community health centers for participation (Table 1). These clinics receive federal support as Federally Qualified Health Centers (FQHCs) or FQHC “look-alike” centers. 24,25
Community Health Center Characteristics.

Abbreviations: EMR, electronic medical record; FQHC, Federally Qualified Health Center; MD, doctor of medicine; NP, nurse practitioner; PCP, primary care provider.
Two members of the research team (MJ, VSN) held an on-site lung cancer didactic session after the completion of a survey to FQHC providers (FQHCPs) in 2016. The 25 question survey consisted of provider demographics, knowledge, attitudes, barriers, and concerns regarding lung cancer screening for each clinic. This survey was modified from a previous version used to query APs based on the input from a multidisciplinary panel of clinical and lung cancer screening experts (VSN, AL, BS) and population health scientists (SSM, IC, AH). 13,26,27 Community providers included physicians, nurse practitioners, and physician assistants, and providers answered the survey either online or by paper (Supplement 1). All study-related processes and materials were approved by the Stanford Institutional Review Board (protocol number 35961). Informed consent was obtained from all individual participants included in this study, and the surveys were completed on a voluntary basis.
We analyzed these community provider responses and compared them with responses from 36 academic primary care physician providers at Stanford University in SCC, who had answered an online survey 1 year earlier as described previously. 23 Briefly, these Stanford PCPs were recruited by a member of the study team (BS) by e-mail to complete a self-administered online survey including 27 questions using the Qualtrics platform (Qualtrics, Provo, Utah).
We defined “knowledgeable providers” as those who correctly identified LDCT lung cancer screening eligibility criteria based on NLST and/or National Comprehensive Cancer Network (NCCN) guidelines for smoking status and age. By the NLST, eligible individuals were 55 to 74 years old with at least a 30 pack-year smoking history and were either current smokers or former smokers who had quit within the past 15 years. By NCCN guidelines, individuals who were 50 to 80 years old with at least a 20 pack-year smoking history were also eligible. Groups of providers were compared descriptively and statistically using a Fisher exact or χ2 test.
Compliance With Ethical Standards
All procedures performed in studies involving human participants were in accordance with the Ethical Standards of the Institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Results
The community health centers care for approximately 80 000 patients largely of Asian/Pacific Islander and Hispanic descent, and primarily insured by Medi-Cal (Table 1). Of the 75 FQHCPs, 36 (48%) invited to participate completed the survey. Of this, 22 (61%) were physicians, 12 (33%) nurse practitioners, and 2 (6%) physician assistants. In all, 29 FQHCPs (81%) were female. In total, 19 (53%) reported their race/ethnicity as Asian/Pacific Islander, 12 (33%) as NH white, 1 (3%) as black, 3 (8%) as Other, and 1 (3%) did not report race/ethnicity.
For comparison, 36 (41%) of 87 of the APs responded to the survey, 31 of which completed it in its entirety. All were physicians, 24 (77%) were female, 17 (55%) were NH white, 12 (39%) were Asian/Pacific Islander, 2 (6%) were Hispanic, and 2 (6%) reported Other. Regarding their patient population, 27 (82%) APs self-reported that ≤5% of their patients were uninsured and 28 (88%) reported that ≤25% of their patients were Hispanic.
In regard to knowledge, FQHCPs reported being less aware of NCCN (P = .001), USPSTF (P = .003), CMS (P = .005), and NLST (P = .002) lung cancer screening guidelines compared to APs (Figure 1). Eight (22%) FQHCPs were considered knowledgeable of LDCT screening based on the NLST and NCCN criteria compared to 11 (31%) of the APs (22% vs 31%, P = .15; Table 2). Based on knowledge of lung cancer screening guidelines, 4 out of 8 knowledgeable FQHCPs (50%) ordered an LDCT compared to 12 of 28 not knowledgeable FQHCPs (43%; P = 1.0). Additionally, 1 of 8 knowledgeable FQHCPs (13%) ordered a CXR over the past 12 months for lung cancer screening compared to 15 of 28 not knowledgeable FQHCPs (54%; P = .053).

FQHC provider (FQHCP) awareness of LDCT screening guidelines compared to academic providers (APs). The FQHCP awareness of LDCT screening guidelines (n = 36) was compared to academic provider awareness (n = 36). Bar charts are shown by type of provider group (FQHCP vs AP) and stratified by color within each bar according to answer type (shown in legend). FQHC indicates Federally Qualified Health Center; USPSTF, US Preventive Services Task Force; CMS, Centers for Medicare and Medicaid Services; LDCT, low-dose computed tomography.
Comparison of Knowledgeable FQHC and Academic Provider Screening Practices and Beliefs.

Abbreviation: LDCT, low-dose computed tomography.
a 25 patients of 28 not knowledgeable community providers responded to the question.
FQHCPs and APs did not have statistically different attitudes about the overall effectiveness of lung cancer screening (P = .11), and each group discussed screening with patients at a statistically similar rate independent of knowledge base (P = .23 for FQHCPs and P = .69 for APs; Table 2). There were no differences in FQHCP concerns between knowledgeable and not knowledgeable providers regarding false-positive rates, potential harm, patient comorbidities, patient unwillingness to undergo screening, the potential for patients being lost to follow-up, a shortage of trained providers in their area, or the resources and training needed to facilitate shared decision making.
In regard to barriers, we compared the answers of those who did discuss LDCT for lung cancer screening with those who did not (Supplement Q14). For providers who discussed screening, 40% of FQHCPs versus 19% of APs reported not having enough time (P = .02; Figure 2). More FQHCPs than APs (87% vs 50%) reported encountering patients who cannot afford or lack adequate insurance (P = .001). Among providers who did not discuss lung cancer screening, 33% of FQHCPs versus 10% of APs reported being concerned about the shortage of trained providers in the area (P = .002). More FQHCPs than APs (22% vs 0%) reported encountering patients who were unable or unwilling to undergo LDCT (P = .0002) (Table 3).
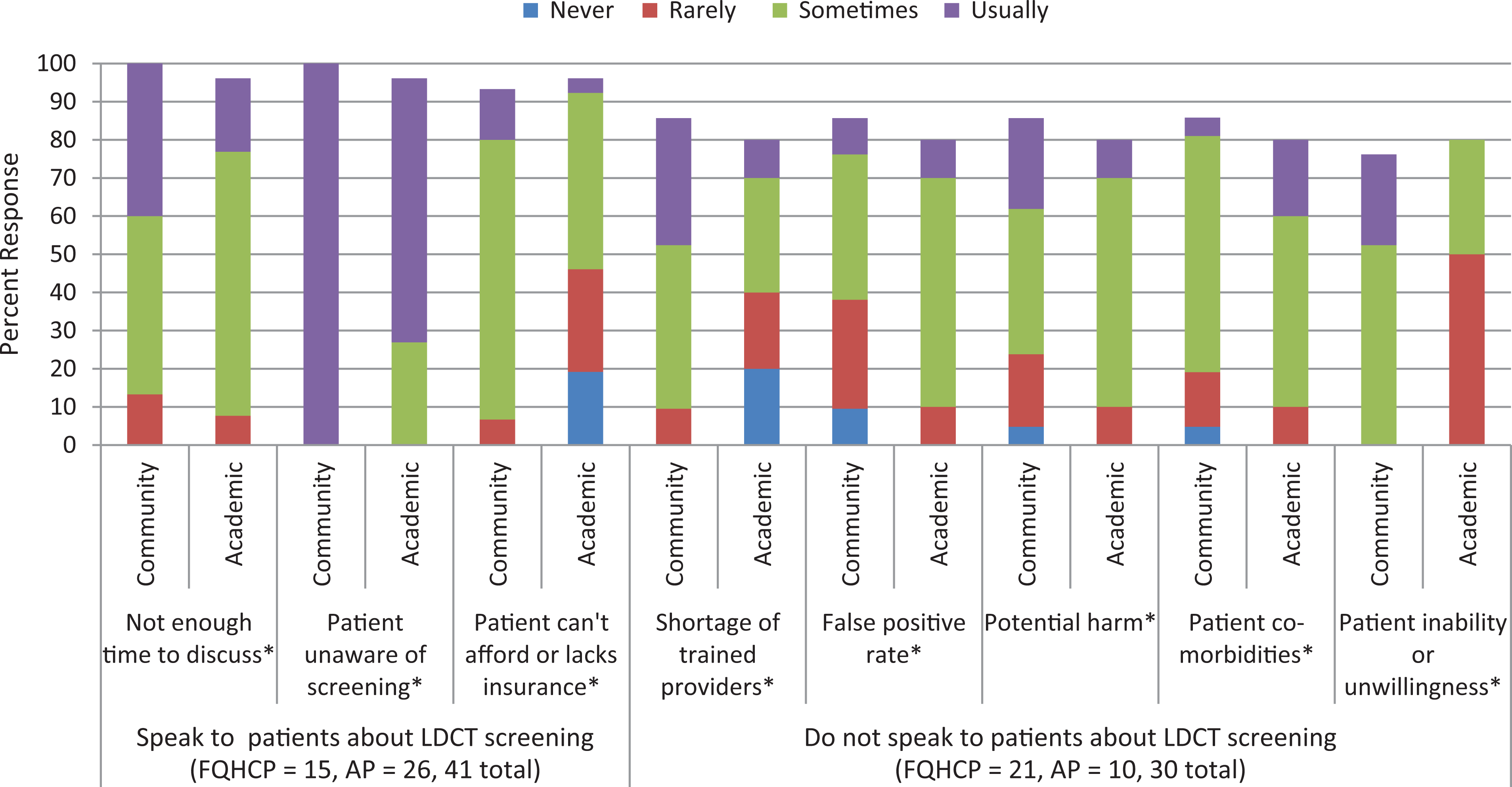
FQHC provider (FQHCP) beliefs of LDCT screening barriers compared to academic providers (APs). Differences in FQHC provider opinions based on whether or not they spoke to their patients about LDCT screening (yes = 15, no = 21) and overall (n = 36) were compared to academic providers’ responses who answered the same questions 1-year prior (spoke to patients about screening = 26, did not speak to patients about screening = 10, overall = 36). Bar charts are shown by type of provider group (FQHCP vs AP) and stratified by color within each bar according to answer type (shown in legend). FQHC indicates Federally Qualified Health Center; USPSTF, US Preventive Services Task Force; CMS, Centers for Medicare and Medicaid Services; LDCT, low-dose computed tomography.
FQHC Provider Awareness, Practice Patterns, Beliefs, and Concerns About LDCT.a

Abbreviations: CMS, Centers for Medicare and Medicaid Services; FQHC, Federally Qualified Health Center; LDCT, low-dose computed tomography; USPSTF, US Preventive Services Task Force.
aVariables by groups shown by number and percent in parentheses.
bOne missing response.
cThree missing responses.
d P value <.05.
Despite these barriers and concerns faced by SCC community providers, more FQHCPs believed LDCT screening was very effective in reducing cancer-related mortality compared to APs (25% vs 11%, P = .0003). Additionally, as many FQHCPs (86%) were interested in participating in continuing medical education regarding lung cancer screening compared to APs (82%), with the majority preferring an on-site (44%) or online (22%) lecture.
Discussion
We evaluated provider knowledge, attitudes, and behaviors regarding LDCT lung cancer screening at FQHCs in comparison to APs within the same county to understand the landscape of screening within SCC and to evaluate LDCT practice patterns between different health systems. We show that FQHCPs reported more limitations that affected LDCT lung cancer screening practice, and while FQHCPs were less informed than APs about screening, more thought it was effective and wanted to learn about it.
Cancer screening and subsequent follow-up care for patients in underserved communities is challenging and contributes to health-care disparities. 28 Survival rates for cancer are lower in more deprived neighborhoods and lower income is associated with higher risk patients who have a higher prevalence of smoking, obesity, and physical inactivity. For lung cancer, those living below the poverty level have a 52% to 75% higher incidence rate 28 and patients with lung cancer without access to care present with more advanced disease that is less amenable to treatment, 29 including likely curative surgery for early-stage disease. A prior study of a military health system showed that black and white patients with lung cancer with equal access to care had similar survival, suggesting that disparities in lung cancer screening, such as race in this case, are mainly a result of inequalities in access to high-quality cancer care. 30
Published studies demonstrate that insurance coverage, 14 time constraints, 31 difficulty managing associated screening findings, and false positives 8,32,33 are all provider-level barriers to screening uptake. Some of these perceived barriers have been recently published as obstacles for clinical lung cancer screening programs in underserved populations. A study by Guichet et al. described the LDCT practices in south Los Angeles County, a minority, socioeconomically disadvantaged, and high-risk patient population. They reported a number of challenges contributed primarily by their patients’ low socioeconomic status that affected inadequate follow-up after screening, which may ultimately decrease the mortality benefit and cost-effectiveness of lung cancer screening initially described in the NLST. 34 Our study adds to this literature by demonstrating that FQHCPs perceive these barriers as a greater threat to successful screening compared to APs, regardless of FQHCPs having the appropriate screening criteria knowledge.
The lack of FQHCP and AP knowledge of LDCT lung cancer screening guidelines across various health-care systems is consistent with several reports from other academic and community health centers, 10,26,31 but no study to date has compared these 2 populations directly within the same provider region.
Study limitations here include, first, a limited sample size of providers. Additionally, surveys to APs were administered a year earlier than those for community providers and LDCT screening awareness had likely increased during this time period, which may explain the lack of differences detected in provider knowledge between the 2 groups. Lastly, FQHCPs included a spectrum of practitioners while APs were exclusively physicians, and this may have accounted for some measured differences in knowledge.
Although we were unable to ascertain whether FQHCPs ordered LDCTs appropriately, we did show that they ordered as many CXRs as LDCTs for screening and that knowledgeable FQHCPs were less likely to order CXRs. This agrees with recent data suggesting that knowledgeable providers are more likely to adhere to guidelines. 9 Since our providers stated that medical education is sought, outreach to providers is one simple step to improve lung cancer screening adoption. Online didactics provided by specialists could be easily implemented within the current structure of the academic medical system that houses experts who are often “siloed,” with our data suggesting it would be well received. The Extension for Community Healthcare Outcomes model (ECHO), 35 which was developed to provide specialty care services for complex disease processes at community-based health centers using a remote didactic system, is an example of one potential solution that has proven successful.
While improving provider education on screening guidelines is an important step forward, similarities in LDCT screening concerns between knowledgeable and not knowledgeable providers among the FQHCPs suggest that focusing on this one important requirement for program initiation is not a complete solution. Systematic changes that streamline screening to make it less of a time burden for providers, insurance solutions that adequately cover the underinsured, increasing PCP access to subspecialist referral, and improving resources for patient education and smoking cessation may facilitate screening success based on our study findings. Lee et al. describe specific effective recruitment methods for lung cancer screening in underserved communities that includes a proactive screening coordinator, transportation assistance, and personalized postscreening navigation as a few examples to improve LDCT uptake in this high-risk patient population. 36
Understanding provider concerns and overcoming barriers to guideline-recommended LDCT for lung cancer screening in diverse patient populations are essential in order to improve appropriate uptake of screening. Further studies evaluating LDCT screening practices across different health-care systems will be vital in order to improve timely and effective cancer diagnosis and treatment for all patients.
Supplemental Material
Supplemental_Blinded_-_Qualtric_Survey - An Analysis of Lung Cancer Screening Beliefs and Practice Patterns for Community Providers Compared to Academic Providers
Supplemental_Blinded_-_Qualtric_Survey for An Analysis of Lung Cancer Screening Beliefs and Practice Patterns for Community Providers Compared to Academic Providers by Marjon Khairy, Duy K. Duong, Salma Shariff-Marco, Iona Cheng, Jennifer Jain, Anupama Balakrishnan, Lynn Liu, Aarti Gupta, Ranjani Chandramouli, Ann Hsing, Ann Leung, Baldeep Singh, and Viswam S. Nair in Cancer Control
Footnotes
Authors’ Note
S. S. M., I. C., A. H., A. L., and V. S. N, designed the study. D. K. D., M. K., S. S. M., I. C., and V. S. N. drafted the manuscript. A. B., L. L., A. G., R. C., and B. S. provided oversight of provider accrual for the study. J. J. performed statistical analyses. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Genentech Independent Research Grant: Establishing effective cancer screening methods for patients of lower socioeconomic status.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.