
Abstract
Background
Cancer is a major health concern in China. Understanding the epidemiology of cancer can guide the development of effective prevention and control strategies. This study aimed to comprehensively analyze the cancer burden, time trends, and attributable risk factors of cancers in China and compare them with those in India.
Methods
We utilized the GLOBOCAN database for 2022, Cancer Incidence in Five Continents (C15 plus) series, and Global Burden of Disease (GBD) 2021 to extract data on cancer incidence, mortality, disability-adjusted life years (DALYs), and risk factors. Time-trend analysis was performed using a join-point regression model. Correlations between cancer DALY rates and risk factors were analyzed using linear regression.
Results
In 2022, China experienced 4,824,703 new cancer cases and 2,574,176 cancer-related deaths. Cancers also caused approximately 71.2 million DALYs in China in 2021. Compared with India, China has higher incidence, mortality, and DALY rates for various cancers. Breast and thyroid cancers in China have shown a rapid increase in the age-standardized incidence rate (ASIR), along with a substantial burden of lung, stomach, esophageal, and colorectal cancer. However, stomach and liver cancers in China showed a downward trend in ASIR. In 2021, diet low in milk was a major risk factor among females for colorectal cancer DALYs in China (23% of age-standardized DALYs) and India (22.9%). In China, smoking has been associated with increased DALYs due to lung cancer.
Conclusions
China has a heavier cancer burden than India. The heavy burden of lung, stomach, esophageal, and colorectal cancers, combined with the rising incidence of breast and thyroid cancers, pose a critical challenge to public health in China. Cancer burden may be reduced through public health initiatives that prioritize primary prevention, prompt identification, and therapeutic intervention.
Introduction
Cancer is a major public health issue worldwide. During the current century, cancer is likely to be the principal cause of premature mortality globally and the most significant barrier to further advancements in life expectancy. 1 The incidence and mortality rates of cancer vary among countries due to various factors, including socioeconomic status, health care accessibility, and lifestyle choices. High-income countries have high rates of cancer incidence. 2 Cancer mortality rates have generally decreased in high-income countries, whereas low- and middle-income countries have experienced increasing cancer mortality rates. 3 Low- and middle-income countries account for 70% of global cancer deaths. 4 Furthermore, disability-adjusted life years (DALYs) attributable to cancer have been steadily increasing over the past few decades, and are projected to continue rising for the next two decades.5,6
China and India are not only the world’s most populous countries but are also facing an increasing burden of cancer.7,8 Since 2000, the incidence and mortality rates of cancer have increased progressively in China.9,10 Smoking, air pollution, and alcohol use are the leading risk factors for increasing cancer burden in China. 11 Similarly, the incidence of cancer in India has risen from 0.6 million cases in 1991 to 1.4 million cases in 2015, indicating a significant increase in the burden of this disease over time. 12 The cancer mortality in India doubled between 1990 and 2016. 13
From 1990 to 2019, China experienced a significant increase in lung and colorectal cancer burden.14,15 Conversely, India has a lower burden of lung and colorectal cancer, but this is increasing due to rising tobacco use, air pollution, and dietary factors. 16 Breast cancer has emerged as a leading cause of morbidity among women in China and India, but has shown differing trends. In China, the incidence of breast cancer has surged with urbanization and lifestyle changes, leading to an age-standardized incidence rate (ASIR) close to that of Western countries, at approximately 35.6 per 100,000 women. 17 In India, the incidence of breast cancer is also rising but remains low. 16 This difference likely reflects variations in reproductive behavior and genetic predisposition.
In light of the increasing cancer burden in China and India, there is a need to develop and implement comprehensive strategies for cancer control. A comparative analysis of the cancer data from these two countries can provide valuable information and insights. This data-driven approach allows us to gain a deeper understanding of the trends, patterns, and determinants of the cancer burden. Our objective is that this comparative analysis may make a meaningful contribution to advancing cancer control measures in both countries.
Materials and Methods
Estimates of the incidence and mortality of cancer for the year 2022 were obtained from the GLOBOCAN 2022 database. 18 The Global Cancer Observatory website, managed by the International Agency for Research on Cancer (IARC), serves as a reliable and comprehensive resource for cancer incidence, mortality, and prevalence data pertaining to 36 different types of cancer across 185 countries or territories. 18 The methodology for delineating data sources and establishing a hierarchy of estimations has been extensively explained in literature. 19 To summarize, GLOBOCAN estimates were compiled on a national scale, utilizing the most reliable sources of cancer incidence and mortality information obtainable within a particular nation. The techniques employed to calculate the 2022 estimates are consistent with those utilized for prior years,20,21 with priority given to short-term projections and modelled mortality-to-incidence ratios when applicable. Validity is determined by the degree of representativeness and quality of the underlying data. 19 For trend analysis of ASIR of cancer, we used data from the Cancer Incidence in Five Continents (C15 plus) series. 22 All ASIRs and age-standardized mortality rates (ASMR) per 100,000 person-years were calculated using the 1966 Segi-Doll World Standard Population.23,24
Cancer DALYs and attributable risk factors for lung and colorectal cancers from 1990 to 2021 were retrieved from the Global Burden of Disease (GBD) database developed by the Institute for Health Metrics and Evaluation (IHME). 25 The GBD study 2021 was planned to present epidemiological data and attributable risk factors for diseases over the period 1990-2021.26,27 The GBD provides annual DALYs and their attributable risk factors for 204 countries and territories by age and sex. Our study provides estimates of DALYs per 100,000 population for 33 cancer sites in China and India in 2021, disaggregated by sex and age. To evaluate the trends in cancer-related DALYs, we also presented the percentage change in all-age- and age-standardized DALY rates in China and India from 1990 to 2021. Attributable risk factors for lung and colorectal cancer were included in this study. Risk factors for lung and colorectal cancers were ranked based on age-standardized DALY rates by sex and year. Descriptions of the risk factors and relative risks for lung and colorectal cancers can be found in a previous study. 28 Age-standardized DALY rates were calculated according to the GBD World Population Standard. 29 The data used in this study are publicly available, and the methods we used to gather information for this article did not involve human tissues or samples. Therefore, ethics approval and informed consent are not applicable to this study.
Statistical Analysis
Join-point regression models were used to evaluate long-term trends in the incidence of the selected cancer types in China and India from 1993 to 2012. 30 We implemented a logarithmic transformation of the ASIRs and used up to three join points in the model. In this study, the annual percentage change (APC) was calculated. Trends were analyzed using the Joinpoint Regression Program (V.5.0.2, National Cancer Institute, 2023).
The correlations between DALY rates and risk factors for lung and colorectal cancers in the corresponding years were investigated using linear regression analysis. Statistical evaluations were conducted using the GraphPad Prism 10 software. Statistical significance was set at P < 0.05.
Results
Cancer Incidence, Mortality, and DALYs in China
According to data from GLOBOCAN 2022, China experienced 4,824,703 new cancer cases in 2022. This substantial number was distributed disproportionately between sexes, with 2,533,906 new cases among males and 2,290,797 new cases among females. The ASIR for all cancers was 201.6 per 100,000 in China. Males exhibited a higher ASIR (209.6 per 100,000), unlike females with an ASIR of 197.0 per 100,000. A supplementary table shows this in more detail (see Supplemental Table 1). When considering males and females together, lung cancer had the highest ASIR at 40.8 per 100,000, followed closely by breast cancer at 33.0 per 100,000 (note that this figure pertains exclusively to female breast cancer), thyroid cancer at 24.6 per 100,000, colorectal cancer at 20.1 per 100,000, liver cancer at 15.0 per 100,000, cervical cancer at 13.8 per 100,000, stomach cancer at 13.7 per 100,000, prostate cancer at 9.7 per 100,000, and esophageal cancer at 8.3 per 100,000 (Figure 1). ASIR and ASMR per 100,000 population in China and India in 2022. (A) ASIR and ASMR per 100,000 population of selected types of cancers in both sexes. (B) ASIR and ASMR per 100,000 population of selected types of cancers in males. (C) ASIR and ASMR per 100,000 population of selected types of cancers in females. Abbreviations: ASIR, age-standardized incidence rate; ASMR, age-standardized incidence rate.
As of 2022, 2,574,176 people in China have lost their lives owing to cancer. The ASMR for all cancers was 96.5 per 100,000 in China. Males had a higher ASMR of 127.5 per 100,000, whereas females had an ASMR of 67.8 per 100,000 (Supplemental Table 2). When we looked at the major causes of cancer-related deaths, lung cancer topped the list with an ASMR of 26.7 per 100,000, followed by liver cancer (12.6), stomach cancer (9.8), colorectal cancer (8.6), esophageal cancer (6.7), and breast cancer (6.1) (Figure 1).
According to the GBD 2021 assessment, cancer contributed to approximately 71.2 million DALYs in China. Among these
Examining the age distribution of cancer DALYs provides further insights into age-specific vulnerabilities and health care priorities. Leukemia emerged as the leading cause of cancer-related DALYs among children and adolescents. While, lung, stomach, colorectal, and liver cancers were the dominant contributors among the 40-59 years age group, impacting the most economically productive segment of the population. Breast cancer accounted for the largest proportion of DALYs in women aged 30-59 years, emphasizing the importance of accessible and timely screening and treatment programs. Among the elderly, lung, stomach, colorectal, and esophageal cancers remained the most significant contributors to DALYs, irrespective of gender. This pattern underscores the need for comprehensive cancer care strategies addressing the unique needs of older adults, including age-appropriate screening guidelines and supportive care measures (Figure 2). Number of disability-adjusted life years (DALYs) attributable to cancers by age and sex in 2021. (A) Number of DALYs attributable to cancers in China. (B) Number of DALYs attributable to cancers in India.
Time Trends of Cancer Incidence and DALYs in China
As illustrated in Figure 3, the findings indicate dynamic changes in cancer incidence rates over time, with variations observed between sexes and different types of cancer. The ASIR for all cancers among males remained moderately steady from 1993 to 2001 in China, but a decline was observed from 2001 to 2012. However, the ASIR for all cancers in females significantly increased from 1993 to 2001 (APC = 1.18%, P < 0.05) and from 2007 to 2012 (APC = 1.82%, P < 0.05). The ASIR for lung cancer showed downward trends in males from 1993 to 2012, with a notable decrease observed during 2001-2009 (APC = −3.30, P < 0.05). From 1993 to 2012, there were significant upward trends in the ASIR for breast cancer in females with a particularly rapid rise during the periods 1993 to 2001 and 2009 to 2012 (APC = 4.09%, P < 0.05 and APC = 4.44%, P < 0.05, respectively). Similarly, the ASIR also showed an increase in thyroid cancer, with the highest significant APC observed during 2008-2012 in males (APC = 22.88%, P < 0.05) and 2003-2012 in females (APC = 16.60%, P < 0.05). The significant increase in breast and thyroid cancer ASIR underscores the need for targeted interventions and resources to manage these rising trends. Conversely, during this timeframe, there were significant declines in the ASIR for stomach, liver, and esophageal cancers in both sexes. In addition, during 2002-2012 in males and 2000-2012 in females, there was a decline observed in the ASIR of colorectal cancer (APC = −0.13, P < 0.05 and APC = −0.70, P < 0.05, respectively). China experienced a downward trend in the ASIR for ovarian cancer during 2002-2012 (APC = −2.46%, P < 0.05). The ASIR for pancreatic cancer among females exhibited a modest increase from 1993 to 2012 (APC = 0.65%, P < 0.05) (Supplemental Figure 1). Trends in ASIR for selected cancers and all cancers by gender in China and India. Abbreviation: ASIR, age-standardized incidence rate.
Figure 4(A) depicts the DALYs associated with 33 different cancer types in China. These cancer types were ranked on the basis of their DALYs. In 2021, lung cancer replaced stomach cancer as the leading cause of DALYs, holding this position in 1990. This shift in rankings may indicate changes in risk factors, health care practices, or environmental exposures over time. Leukemia has demonstrated a noteworthy decline in both all-age and age-standardized DALY rates (−53.54% and −55.89%, respectively) since 1990. Esophageal cancer has maintained its status as the third leading cause of cancer in terms of all-cause DALYs, despite a substantial reduction in age-standardized DALY rates (−51.45%) over the past 31 years. This could imply ongoing challenges in prevention or early detection efforts for esophageal cancer. Colorectal cancer has experienced an increase in its rankings, becoming the fourth leading cancer in terms of all-age DALYs. The all-age DALY rate for colorectal cancer increased by 58.84% from 1990 to 2021. Additionally, there have been substantial increases in both all-age- and age-standardized DALY rates for pancreatic and prostate cancers since 1990, indicating a need for targeted interventions and resources to address these rising trends. Conversely, the age-standardized DALY rates for laryngeal and uterine cancers decreased by 43.71% and 47.37%, respectively, suggesting potential successes in prevention or treatment strategies for these types of cancer. Rank changes in cancer DALYs from 1990 to 2021. (A) percent changes in all-age and age-standardized DALY rates in China from 1990 to 2021. (B) percent changes in all-age and age-standardized DALY rates in India from 1990 to 2021. Abbreviation: DALY, disability-adjusted life years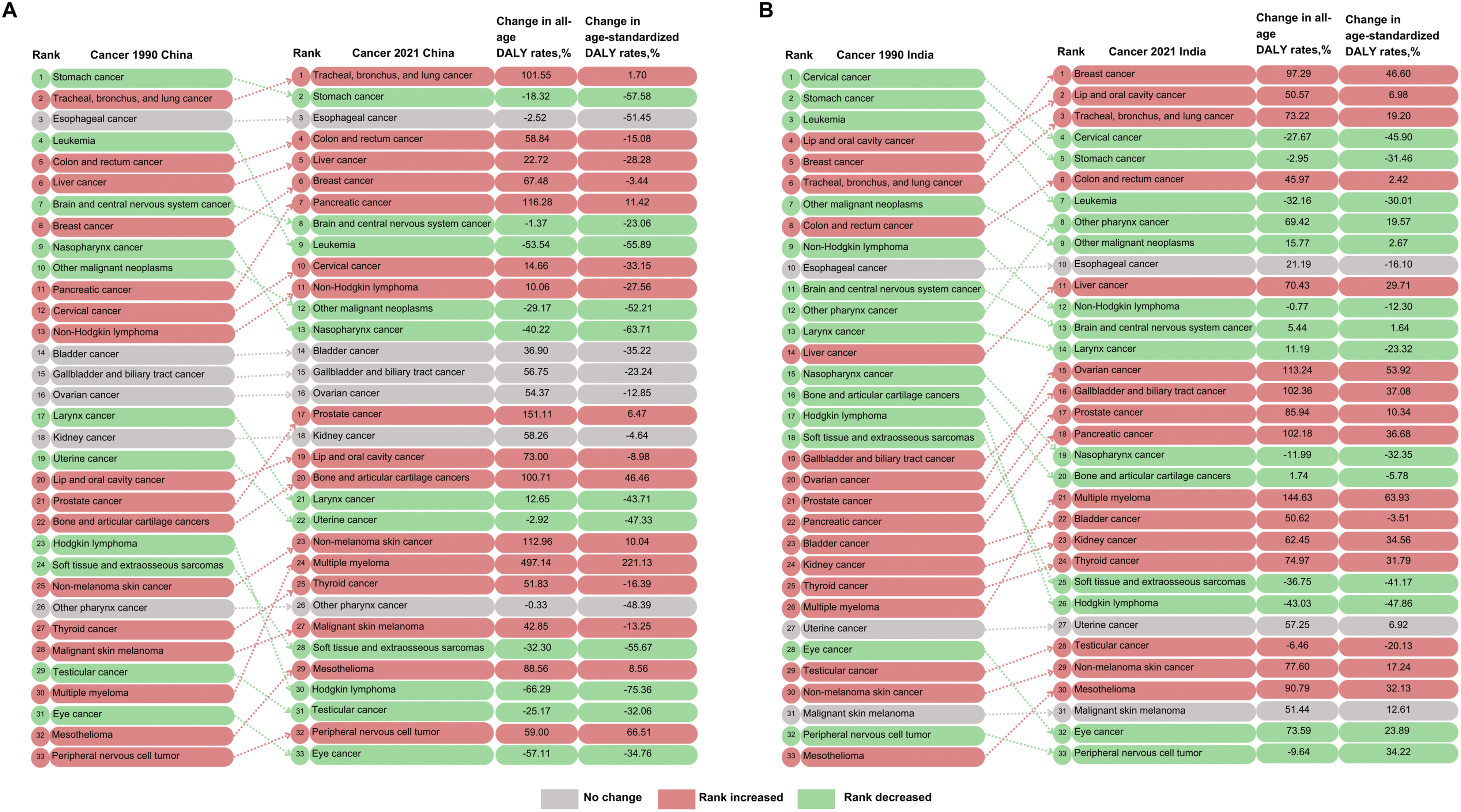
Comparison with India in Cancer Incidence, Mortality, and DALYs
According to GLOBOCAN 2022 data, there were substantial differences in cancer incidence and mortality rates between China and India. In China, the incidence and mortality rates of all cancers were higher than those in India. The ASIR per 100,000 in China was approximately two times higher for both males (209.6) and females (197.0) compared to the rates in India for males (97.1) and females (100.8) (Supplemental Table 1). China had an ASMR nearly two times higher than that of India for males (127.5 and 66.5 per 100,000, respectively), with a slightly higher ASMR observed for females (Supplemental Table 2).
Figure 1 provides an overview of the selected types of cancers among males and females in China and India in 2022, based on ASIR and ASMR. Lung, colorectal, stomach, and esophageal cancers were among the top five cancers among males in both countries. Oral cavity (including lip) cancer was the leading cancer in males in India. However, in China, lung cancer was the leading cancer, with notably higher incidence rates of colorectal and liver cancers among males (24.7 and 22.7 per 100,000, respectively), compared to Indian men (6.1 and 3.9 per 100,000, respectively). Conversely, in India, the ASIR for males indicated a higher occurrence of laryngeal cancer than in China (4.5 and 2.2 per 100,000, respectively). Among Chinese women, the highest ASIR and ASMR were observed in lung and colorectal cancer. In contrast, Indian women had higher ASIR and ASMR for cervical and ovarian cancers. Notably, the ASIR for breast cancer and thyroid cancer in Chinese women was higher, whereas the ASMR was lower than that in Indian women. It is noteworthy that both sexes experienced elevated ASMR for liver, stomach, and esophageal cancers in China compared with India.
In 2021, there were variations in cancer burden between China and India. China exhibited a higher age-standardized DALY rate per 100,000 population for all cancers than India. The age-standardized DALY rate in China was 3469.64 per 100,000 population, while it stood at 2016.32 per 100,000 population for India, highlighting the disparities in cancer burden between the two countries. Across both countries, lung cancer emerged as the leading contributor to the overall cancer DALYs in males, indicating a common trend in the prevalence of this type of cancer among men in China and India. In China, aside from lung cancer, digestive cancers, such as stomach cancer, esophageal cancer, and colorectal cancer, also played a substantial role in cancer DALYs, suggesting a different pattern of cancer distribution compared to India. In contrast, the largest contributors to DALYs in Indian men were oral cavity (including lip) cancer, stomach cancer, other pharynx cancer, and colorectal cancer. Furthermore, in China, the primary contributor to DALYs among females was lung cancer, whereas in India, breast cancer played a leading role, featuring the gender-specific differences in cancer prevalence between the two countries (Additional file 3). When considering the distribution of cancer DALYs by age, leukemia emerged as the predominant contributor to DALYs in children and adolescents in both countries, underscoring the impact of this type of cancer on the younger population. In contrast to China, oral cavity (including lip) cancer had a higher impact on the younger population in India. Among females aged 30-49 years, breast cancer was the most common in India, whereas Chinese women were more affected by lung cancer, revealing age-specific differences in cancer prevalence among women in the two countries. In the elderly population in China, lung cancer remained the leading contributor to DALYs, whereas in India, it was colorectal cancer, identifying the age-related variations in cancer burden between the two countries (Figure 2).
Comparison with India in Time Trends of Cancer Incidence and DALYs
From 1993 to 2012, notable variations in cancer incidence were evident in both China and India. In contrast to China, India observed significant upward trends in ASIR for all male cancers (APC = 0.80%, P < 0.05). India also experienced upward trends in liver incidence rates, with APC = 40.98%, P < 0.05 and APC = 8.54%, P < 0.05 in males during (1993-1995 and 2004-2012, respectively), and APC = 2.24%, P < 0.05 in females between 1993-2012. The ASIR for lung cancer in Indian women significantly increased by APC = 4.65%, P < 0.05 during 1993-2012. Both China and India observed decreases in ASIRs for esophageal cancer; however, colorectal cancer rates showed an upward trend in India (APC = 3.87%, P < 0.05 in males during 1993-2012 and APC = 4.67%, P < 0.05 in females during 2000-2012). The incidence rates of female breast cancer and thyroid cancer in males increased in India, but remained consistently lower than those in China. The incidence rate of stomach cancer has remained stable in India (Figure 3). There was an upward trend in the ASIR for leukemia among females in India from 1993 to 2012 (APC = 2.09%, P < 0.05), in contrast to the trend observed in China (APC = 0.19%, P < 0.05). India experienced an increasing trend in the ASIR for pancreatic cancer in males during 2002-2012 (APC = 4.48%, P < 0.05). Nevertheless, Indian women experienced a significant decline in the ASIR for cervical cancer between 2000-2012 (APC = −4.71%, P < 0.05). In contrast, the ASIR for prostate cancer in China increased rapidly from 1993 to 2012 (from 1993 to 2002, APC = 11.94, P < 0.05, and from 2002 to 2012, APC = 4.42, P < 0.05) (Supplemental Figure 1).
Changes in cancer DALYs in India were noticeably different from those in China (Figure 4). Although stomach cancer was still in the top five leading cancers DALY in both countries since 1990, their all-age and age-standardized DALY rates declined over this period in both countries. In contrast to China, the largest changes in cancer DALYs in India were observed for breast and lung cancers. All-age DALY rates of breast cancer and lung cancer have increased by 97.29% and 73.22%, respectively, since 1990, leading to an increase in their position from fifth and sixth to the first and third, respectively. India has experienced a noticeable increase in both all-age and age-standardized DALY rates for liver, gallbladder, ovarian, and bladder cancers, highlighting the importance of prioritizing efforts for the prevention, early detection, and treatment of these specific cancer types. The significant drop in rankings for cervical cancer may indicate improvements in prevention or treatment strategies for this type of cancer in India.
Attributable Risk Factors for Lung and Colorectal Cancers in China and India
In 2021, smoking was the leading risk factor for lung cancer DALYs in males in both countries, contributing to 80.8% (age-standardized DALYs) in China and 54.2% in India. Diet low in fruits was the leading risk factor for lung cancer DALYs among Indian women (20.2%), followed by household air pollution from solid fuels (17.5%). In contrast, smoking was the top risk factor for lung cancer DALYs among Chinese women (23.2 %), followed by ambient particulate matter pollution (21.3%). The primary risk factor for colorectal cancer DALY in males in both countries was diet low in whole grains, accounting for 18.0% in China and 17.1% in India. Diet low in milk emerged as the top contributor to colorectal cancer DALY in females across China (23.0%) and India (22.9%) (Figure 5). Attributable risk factors of age-standardized lung and colorectal cancers-related DALYs percent by sex in 2021. (A) China. (B) India. Abbreviation: DALY, disability-adjusted life year.
This study also examined the correlations between age-standardized DALY rates and risk factors for lung and colorectal cancer in the corresponding years from 1990 to 2021. Over the past three decades in China, smoking was strongly associated with increased lung cancer DALY rates in both males (r = 0.9896, R2 = 0.9792, P < 0.0001) and females (r = 0.8842, R2 = 0.7818, P < 0.0001) (Figure 6fig6). Residential radon was significantly linked to increased DALY rates for lung cancer in China and India (r = 0.9974, R2 = 0.9949, P < 0.0001 and r = 0.9981, R2 = 0.9963, P < 0.0001, respectively), whereas household air pollution from solid fuels showed no association with lung cancer DALY. Ambient particulate matter pollution in India was significantly correlated with increased DALY rates for lung cancer (r = 0.9130, R2 = 0.8336, P < 0.0001) (Figures 6 and 7). Linear regression of selected risk factors and age-standardized lung cancer-related DALYs rate in China. (A-C) Smoking in corresponding years by sex from 1990 to 2021. (D-F) Ambient particulate matter pollution in corresponding years by sex from 1990 to 2021. (G-I) Household air pollution from solid fuels in corresponding years by sex from 1990 to 2021. (J-L) Residential radon in corresponding years by sex from 1990 to 2021. Abbreviation: DALY, disability-adjusted life years. Linear regression of selected risk factors and age-standardized lung cancer-related DALYs rate in India. (A-C) Smoking in corresponding years by sex from 1990 to 2021. (D-F) Ambient particulate matter pollution in corresponding years by sex from 1990 to 2021. (G-I) Household air pollution from solid fuels in corresponding years by sex from 1990 to 2021. (J-L) Residential radon in corresponding years by sex from 1990 to 2021. Abbreviation: DALY, disability-adjusted life years.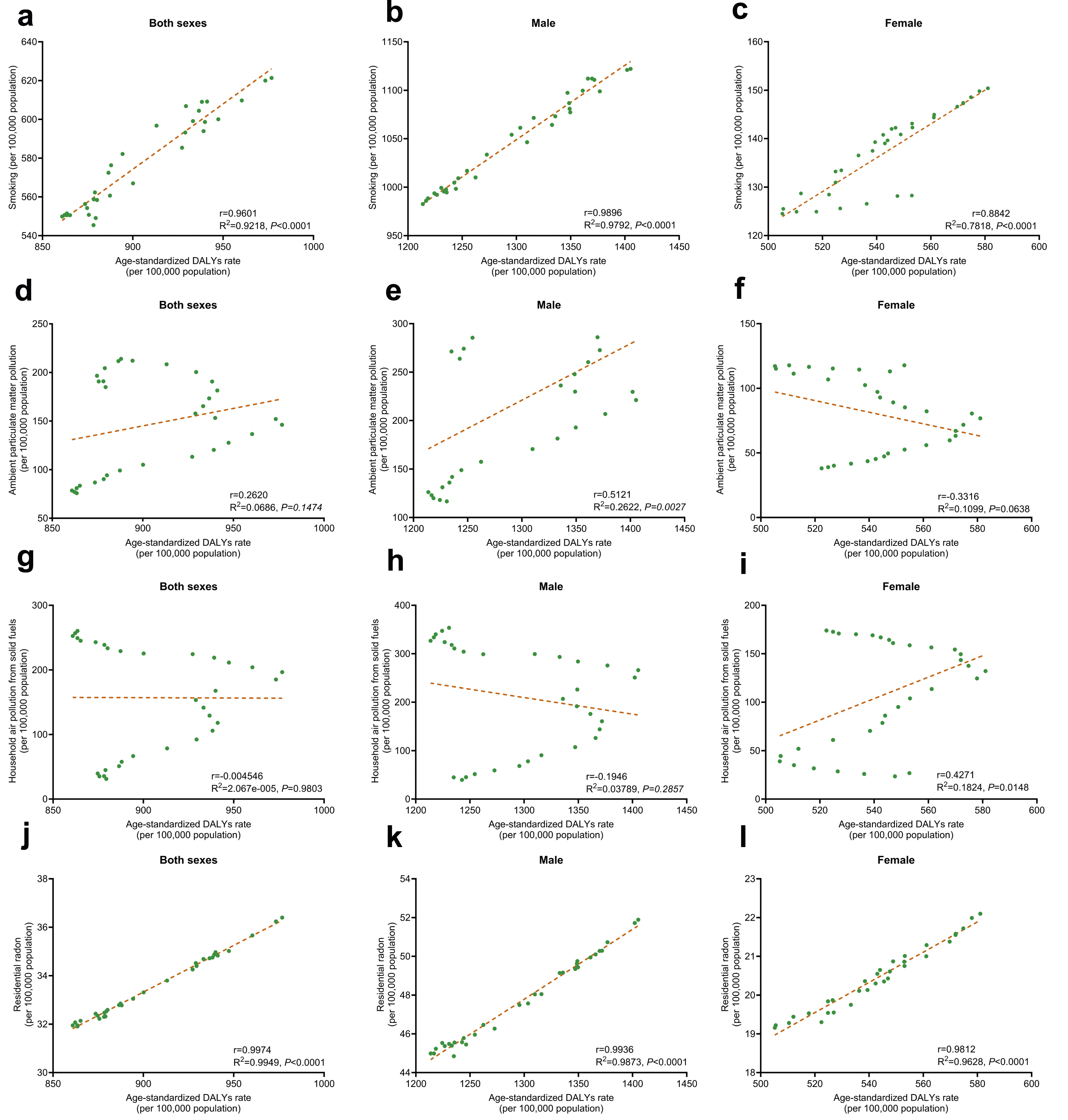

Regarding colorectal cancer, certain dietary habits have shown a significant positive correlation with increased DALY rates in both countries. Diet low in whole grains exhibited a very strong positive correlation with increased DALY rates (r = 0.9993, R2 = 0.9987, P < 0.0001 in China and r = 0.9989, R2 = 0.9978, P < 0.000 in India). Diet low in milk also demonstrated a strong positive correlation with increased DALY rates (r = 0.9990, R2 = 0.9980, P < 0.0001 in China and r = 0.9976, R2 = 0.9951, P < 0.0001 in India). Diet high in red meat showed a significant positive correlation with increased DALY rates (r = 0.9694, R2 = 0.9397, P < 0.0001 in China and r = 0.8997, R2 = 0.8094, P < 0.0001 in India) (Figures 8 and 9). Smoking was strongly associated with increased DALY rates for colorectal cancer in Chinese women (r = 0.9930, R2 = 0.9861, P < 0.0001). These findings underscore the importance of dietary choices in the prevention and management of colorectal cancer, suggesting that increasing the intake of whole grains and milk while reducing the consumption of red meat could potentially lower the risk of this disease in both countries. Linear regression of selected risk factors and age-standardized colorectal cancer-related DALYs rate in China. (A-C) Diet low in milk in corresponding years by sex from 1990 to 2021. (D-F) Diet low in whole grains in corresponding years by sex from 1990 to 2021. (G-I) Diet high in red meat in corresponding years by sex from 1990 to 2021. (J-L) Smoking in corresponding years by sex from 1990 to 2021. Abbreviation: DALY, disability-adjusted life years. Linear regression of selected risk factors and age-standardized colorectal cancer-related DALYs rate in India. (A-C) Diet low in milk in corresponding years by sex from 1990 to 2021. (D-F) Diet low in whole grains in corresponding years by sex from 1990 to 2021. (G-I) Diet high in red meat in corresponding years by sex from 1990 to 2021. (J-L) Smoking in corresponding years by sex from 1990 to 2021. Abbreviation: DALY, disability-adjusted life years.

Discussion
Based on the GLOBOCAN 2022, CI5 Plus, and GBD 2021 databases, we comprehensively compared cancer statistics 2022, DALYs 2021, time trends, and attributable risk factors for lung and colorectal cancers in China and India. Our findings indicated that China had a higher incidence, mortality, and DALY rates of various cancers than India. Moreover, the incidence of breast, thyroid, and prostate cancers, as well as the DALY burden of lung and pancreatic cancers, has increased rapidly in China, accompanied by a substantial burden of stomach, esophageal, colorectal, and liver cancers.
The observed differences in the cancer burden between China and India are attributable to China’s rapid economic development and aging population. These factors precipitate lifestyle and environmental changes, which, in turn, contribute to the rising cancer burden. 31 Additionally, certain genetic mutations are more prevalent in East Asian populations,32,33 which may partly explain the higher incidence of certain cancers in China than that in India. A study in China identified TP53 (51.4%), LRP1B (13.4%), PIK3CA (11.6%), KRAS (11.1%), EGFR (10.6%), and APC (10.5%) as the most frequently mutated cancer genes. 34 Disparities in health care access significantly affect cancer diagnosis, treatment, and survival rates. In China, health care services are predominantly concentrated in urban areas, leading to delays in diagnosis and treatment of rural populations. This urban-rural divide can exacerbate disparities in cancer burden. To reduce the cancer burden in China, it is crucial to establish a strong primary public health system, especially in rural areas. 35 It is also essential to revise the National Catalogue of Medical Insurance to include more treatments, improve medical insurance financing, and reform hospital payment methods. 36 Data collection biases can affect the accuracy of cancer statistics. Differences in cancer registry coverage, diagnostic capabilities, and reporting practices between China and India can influence the observed cancer incidence and mortality rates.
Our study found that in China, lung cancer had the highest incidence and mortality among both men and women, ranking first and posing a significant challenge owing to its poor prognosis and substantial DALY burden. 37 In China, smoking was strongly associated with an increased lung cancer DALY burden and remained a leading risk factor in 2021. Smokers have a 20-fold greater relative risk of lung cancer than nonsmokers. 38 China and India are the leading countries among the list of 10 countries with the largest number of tobacco smokers, accounting for approximately two-thirds of the world’s smokers. 39 China has a higher smoking rate (26.59%) than India (12.84%).40,41 In China, tobacco smoking was found to be responsible for an estimated 75.04% of lung cancer deaths in males and 18.35% in females. 42 Other major risk factors for the lung cancer burden in China include ambient particulate matter pollution and household air pollution from solid fuels. 43 In contrast, in line with our current findings, a prior study utilizing data from six population-based cancer registries in India demonstrated that oral cancer exhibited the highest incidence among males, followed by lung cancer. 44 The ASIR per 100,000 for oral cancer in Indian men (14.7) was higher compared to China (1.0) and other neighboring countries such as Pakistan (12.1), Bangladesh (13.6), and Sri Lanka (14.0). 18 The higher incidence of oral cancer among Indian men can be attributed to the widespread use of smoked and non-smoked tobacco products. 45 Therefore, comprehensive tobacco control strategies are needed to reduce the cancer burden. Over the past few decades, strong tobacco control policies have led to a significant decline in smoking prevalence across Europe. 46 These include taxation on tobacco products, advertising bans, and smoke-free policies, all of which have proven effective in reducing tobacco use.47,48 The University of Texas MD Anderson Cancer Center launched the End Tobacco Program in 2012 to combat the burden of tobacco-related cancers and their associated health risks. This statewide initiative was aimed at promoting cancer control. By 2021, the program had yielded significant success. The adult smoking rate in Texas decreased from 19.2% in 2014 to 13.2%. 49 The governments of China and India should undertake similar initiatives to address significant tobacco control challenges.
Breast cancer poses a major health concern for women in China, as evidenced by its increasing incidence. 50 Our findings revealed a higher ASIR for female breast cancer in China than in India, while the ASMR was lower in China. According to prior research, China had a relatively low breast cancer incidence compared to other countries; however, during the 1990s, especially in urban areas, this incidence climbed more than twice as quickly as the global rate. 51 The ASIR increased from 46.34 per 100,000 individuals aged 20 years and above in 2003 to 68.78 per 100,000 in 2017, with a significant Average Annual Percentage Change (AAPC) of 2.5%. 52 The increasing incidence of breast cancer can be linked to changes in risk and demographic factors as well as the widespread practice of mammography screening.53,54 China’s breast cancer cases are projected to rise by 22.9% between 2015 and 2030 due to population expansion and aging. 54 Breast cancer mortality rate in India increased by 1.1% per year from 2000 to 2019. 55 The ASMR per 100,000 for breast cancer in Indian women (13.7) was also higher than in Bangladesh (7.6) and Sri Lanka (11.2). 18 The high breast cancer mortality rates in India can be attributed to delayed diagnosis, economic challenges, fear, denial, and the tendency of patients to present with advanced or metastatic disease. 56
Our trend analysis indicated a rapid increase in the ASIR for thyroid cancer in China. The ASIR for thyroid cancer in men increased from 1.3 per 100,000 in 1998 to 9.2 in 2012, with a significant APC of 17.3%. Women also saw a dramatic increase, with the ASIR of thyroid cancer increasing from 3.1 per 100,000 in 1998 to 25.5 in 2012, with a significant APC of 18.9%. 57 In 2022, thyroid cancer ranked third in terms of incidence in China, accounting for 9.7% of all new cancer cases. China exhibited a higher ASIR per 100,000 for thyroid cancer (24.6) compared to India (1.5) and other neighboring countries, such as North Korea (3.3), Russia (8.0), and Pakistan (1.6). 18 The increased incidence of thyroid cancer in China has been attributed to factors such as exposure to ionizing radiation and overdiagnosis. 58 However, the relatively low thyroid cancer mortality rate in China suggests that increased cancer awareness has led to early diagnosis and treatment. We also observed that prostate cancer incidence rates have increased significantly in China. The ASIR of prostate cancer increased at a rate of 12.6% annually between 2000 and 2005 and then further increased at a slower rate of 4.7% annually between 2005 and 2011. 10 This increase may be due to improvements in detection and screening methods, which have led to the diagnosis of more cases. 59
China and India have experienced an upward trend in the DALY burden of colorectal and pancreatic cancers between 1990 and 2021. In China, the incidence of pancreatic cancer has increased by 82.11% over the past 30 years, while the mortality rate has increased by 79.46%. 60 Since 1991, Indian women have experienced a sharp increase in pancreatic cancer incidence rates, with a significant AAPC of 3.7%. Indian men also saw an increase but at a slower rate of 1.2% annually. 61 The increase in pancreatic cancer burden in both countries is attributed to modifiable risk factors such as smoking, excessive alcohol consumption, and high red meat consumption.62,63 Our trend analysis showed that the ASIR for colorectal cancer declined in China from 2000 to 2012. However, recent trend analysis from 2000 to 2018 has shown an upward trend in the ASIR of colorectal cancer, with (AAPC = 2.7%, P < 0.05 in males) and (AAPC = 1.1%, P < 0.05 in females). 64 In India, colorectal cancer incidence rates increased by 20% between 2004 and 2014. 65 Additionally, the mortality rate significantly increased from 2000 to 2019, with (APC = 1.0%, P < 0.05). 55 In both countries in 2021, a diet low in milk was the leading risk factor for colorectal cancer DALY burden in females, with a strong association with increased DALY rates in both sexes. This is consistent with evidence that dairy consumption is inversely associated with the risk of colorectal cancer.66,67 Other risk factors, such as a diet high in red meat and alcohol intake, were also linked with increased colorectal cancer burden. 68
In contrast to India, China showed downward trends in ASIR for liver and stomach cancer. This decline in liver cancer incidence can be attributed to a reduction in risk factors such as hepatitis B infection. 69 The decrease in stomach cancer incidence can be attributed to several factors, including the reduction in Helicobacter pylori infection.70,71 Moreover, the ASIR for esophageal cancer has decreased in both countries, which is consistent with previous findings.72,73 This decline may be associated with increased intake of fruits and vegetables.74,75 One study indicated that fruit and vegetable consumption increased in China from 1991 to 2009. 76 Both countries experienced a downward trend in leukemia DALY burden between 1990 and 2021, with China’s leukemia mortality rate dropping by 2.5% annually from 2012 to 2017, 77 which could be attributed to advancements in cancer diagnosis and treatment. However, leukemia accounts for a significant portion of the burden of DALY among children and adolescents in China in 2021. Genetic mutations could be the reason for the heavy burden of leukemia in Chinese children. 78 The heavy burden of leukemia in this age group is concerning, as it not only affects the quality of life of young patients but also imposes a significant economic burden on families and health care systems.
Several studies have reported an increasing cancer burden in India.12,79 The proportion of deaths attributed to cancer showed a clear rise between 2000 and 2018, increasing from 3.6% to 6.4%, while cancer incidence is projected to rise by 12% from 2020 to 2025. 80 Our trend analysis also indicated that the ASIR for all cancers increased gradually in both sexes in India during 1993-2012. This is because of several factors, including rapid urbanization, an aging population, unhealthy and sedentary lifestyles, indoor and outdoor air pollution, and genetic and hereditary factors. 80 In 2022, Indian women experienced higher incidence and mortality rates of cervical and ovarian cancers than Chinese women. Low HPV vaccination rates are considered a significant contributing factor to the heavy burden of cervical cancer in India. 81 A high burden of ovarian cancer in the Indian population is associated with a high prevalence of inherited genetic mutations. 82 In England, multi-cancer early detection (MCED) screening has led to a significant 17% annual reduction in cancer mortality among 100,000 screened individuals. 83 Therefore, the Indian government should prioritize promoting early detection and screening, vaccination, improving health care infrastructure, and ensuring affordable and equitable access to cancer treatment.
Limitations
This study had some limitations. First, differences in health care systems and data collection methods in each country could lead to inaccurate comparisons of estimates. Second, the time trend analysis of cancer incidence was based on data from a limited number of cancer registries in China (Hong Kong, Jiashan, Shanghai, Harbin, and Zhongshan) and India (Chennai), which collectively covers a relatively small proportion of the population in each country. Lastly, trends since 2012 could not be evaluated due to data limitations.
Conclusions
Our study highlights significant differences in the cancer burden between China and India, with China having a higher burden of cancer. China is facing a major health care challenge owing to the heavy burden of lung, stomach, esophageal, and liver cancers, as well as the increasing burden of breast, colorectal, pancreatic, prostate, and thyroid cancers. Our analysis identified smoking as a key risk factor contributing to the increased lung cancer burden in China. To effectively address the distinct patterns of cancer in China, comprehensive interventions are needed, including targeted health education, cancer awareness initiatives, promotion of healthy lifestyles, implementation of effective cancer screening methods, and stringent tobacco control regulations.
Supplemental Material
Supplemental Material - Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India
Supplemental Material for Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India by Syed Adnan Rahmat and Yutong He in Cancer Control
Supplemental Material
Supplemental Material - Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India
Supplemental Material for Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India by Syed Adnan Rahmat and Yutong He in Cancer Control
Supplemental Material
Supplemental Material - Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India
Supplemental Material for Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India by Syed Adnan Rahmat and Yutong He in Cancer Control
Supplemental Material
Supplemental Material - Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India
Supplemental Material for Cancer Burden and Attributable Risk Factors of Cancers in China: Epidemiological Insights and Comparisons With India by Syed Adnan Rahmat and Yutong He in Cancer Control
Footnotes
Authors’ Contributions
Y.H. and S.A.R. conceived and designed the study. S.A.R. analyzed the data and drafted the manuscript. Y.H. revised the manuscript accordingly. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Publicly available datasets were analyzed in this study. The data can be found on the Global Cancer Observatory website https://gco.iarc.fr/and the Global Burden of Disease Study 2021 ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.