
Abstract
Background
Both tumor deposits (TD) and perineural invasion (PNI) have been identified as risk factors for poor survival in patients with non-metastatic colorectal adenocarcinoma (CRC). However, the adverse impacts of TD and PNI on the survival of patients with non-metastatic CRC have not been compared.
Method
Patients with non-metastatic CRC with known TD and PNI status were selected from the Surveillance, Epidemiology, and End Results (SEER) database. First, bivariate logistic regression analysis was utilized to identify the factors associated with TD and PNI status. Then, patients were divided into four groups, according to TD and PNI status. Propensity score matching (PSM) was performed to balance the baseline covariates. The impact of TD and PNI on survival was assessed by analyzing overall survival (OS) and cancer-specific mortality (CSM) rates. OS was calculated by the Kaplan–Meier method with log-rank analysis. CSM was estimated by competing risk analysis using the Fine and Gray model.
Results
A total of 70 689 patients with CRC met the inclusion and exclusion criteria. The positive rates of TD and PNI were 9.37% and 9.91%, respectively. For TD, the most important risk factor was N stage. With respect to PNI, the most significant factor was T stage. Tumor location, tumor size, differentiation grade, and serum CEA level were also correlated with TD and PNI status. After PSM, 1849 pairs were selected. Patients with TD+PNI+ status had the worst 5 year CSM and 5 year OS. In addition, the long-term survival outcomes of patients with TD+PNI− and TD−PNI+ status were comparable.
Conclusion
The adverse impacts of TD and PNI on the survival of patients with non-metastatic CRC were comparable. CRC patients with both TD and PNI positive had the worst survival outcome.
Keywords
Introduction
The International Duration Evaluation of Adjuvant Chemotherapy (IDEA) proposed that the choice and duration of chemotherapy regimen for patients with colon cancer should be personalized.1-3 So, it is of great importance to identify patients who are at higher risk of relapse or metastasis. The IDEA research stratified colon cancer patients into high risk group and low risk group, according to T stage and N stage only.
Tumor deposits (TD) are defined as isolated tumor foci found in the pericolic or perirectal fat or in the adjacent mesentery that are discontinuous with the primary lesion and with no evidence of residual lymph node tissue.4,5 TD have been reported to be a unique factor, different from lymph node metastasis, that predict poor prognosis in patients with colorectal adenocarcinoma (CRC).6,7
The generally accepted definition of perineural invasion (PNI) is the presence of tumor cells within any layer of the nerve sheath. Tumor cells surrounding at least 33% of the nerve circumference are also defined as PNI.8,9 Several studies have confirmed that PNI impacts the long-term survival of patients with CRC.10,11
TD and PNI are demonstrated to be risk factors for poor survival in patients with non-metastatic CRC. However, these two factors are not involved in the risk stratification model for personalized chemotherapy. Further data on the adverse impacts of TD and PNI on survival were lacking. Which factor has a greater impact on survival is not clear. There is no evidence that patients with CRC that is both TD and PNI positive have the worst outcome than those with CRC positive for either TD or PNI alone.
In this study, we analyzed clinical features associated with TD and PNI status and compared the survival of patients with non-metastatic CRC with positive TD and/or PNI status. Based on these analyses, we attempted to optimize the personalized chemotherapy regimen for CRC patients based on TNM stage system and TD, PNI status.
Patients and Methods
Patients
Patient data were retrieved from the following Surveillance, Epidemiology, and End Results (SEER) database: Incidence-SEER 18 Regs Custom Data (with additional treatment fields), Nov 2018 Sub (1975–2016 varying). CRC was identified by three variables “Site recode ICD-O-3/WHO 2008,” “Behavior and Histology recode-broad grouping,” and “Behavior code ICD-O-3,” with the values of “Colon and rectum,” “8140-8389 adenomas and adenocarcinomas,” and “Malignant”, respectively.
Patients with non-metastatic CRC who underwent radical surgery with no fewer than 12 harvested lymph nodes were enrolled in this study. Patients with missing values for race, specific tumor location, differentiation grade, TD status, PNI status, and tumor size were excluded from this study. In addition, patients who received radiotherapy before surgery were also excluded because tumor regression post-neoadjuvant therapy would interfere with the diagnosis of TD (Figure 1).
12
The flow diagram of selection process for the study population.
Statistics Analysis
Bivariate logistic regression analysis was performed to identify factors associated with TD and PNI status. Then, all patients were divided into four groups according to TD and PNI status (TD−PNI- vs TD−PNI+ vs TD+PNI− vs TD+PNI+). The TD+PNI+ group was chosen as the reference group. The other three groups were matched with the reference group by propensity score analysis (PSM). The PSM was carried out using SPSS (https://sourceforge.net/projects/psmspss/files/psmatching3.04/). The matching ratio was 1:1, and the caliper value was set as .05.
The Wilcoxon rank-sum test was used for non-normally distributed data. The χ2 test was performed to compare the enumeration data. The overall survival rate was calculated by the Kaplan–Meier method with the log-rank test. The cause of mortality was classified into the following two subsets: death from CRC and death attributed to other diseases. The cumulative incidence of cause-specific mortality was calculated by competing risk analysis using “cpmrsk” package in R. All statistical analyses were performed using the SPSS 22.0 (SPSS Inc, Chicago, IL, USA) and R software (version 4.0.3; http://www.r-project.org/). Two-sided P < .05 was considered statistically significant.
Results
Patient Characteristics
Characteristics of patients enrolled in risk factor analysis for TD and PNI.

TD, tumor deposit; PNI, perineural invasion; CEA, carcinoma embryonic antigen.
aIncluding borderline and untested.
bIncluding cecum, ascending colon, and hepatic flexure.
cIncluding splenic flexure, descending colon, and sigmoid colon.
dIncluding rectosigmoid junction and rectum.
Risk factors for TD- and PNI-positive status
Risk factors associated with TD and PNI status according to the logistical regression model.

TD, tumor deposit; PNI, perineural invasion; OR, odds ratio; CI, confidence interval; CEA, carcinoma embryonic antigen.
The impact of TD and PNI on oncological outcome
Baseline characteristics of patients with different TD/PNI status before and after PSM.

PSM, propensity score matching; TD, tumor deposit; PNI, perineural invasion; CEA, carcinoma embryonic antigen.
aIncluding borderline and untested
bIncluding cecum, ascending colon, and hepatic flexure
cIncluding splenic flexure, descending colon, and sigmoid colon
dIncluding rectosigmoid junction and rectum
The median OS times were 81 months and 53 months for patients with TD-negative and TD-positive status, respectively. Patients with TD-positive status had a significantly worse OS rate (P < .001) and higher cancer-specific mortality rate (P < .001) than those with TD-negative status. The 1-, 3-, and 5-year OS rates were 85.3%, 62.2%, and 45.4% in the TD-positive group, and 88.0%, 68.6%, and 56.9% in the TD-negative group, respectively (Figure 2(A)). The corresponding cancer-specific mortality rates for the TD-positive group at 1-, 3-, and 5- years were 8.7%, 24.5%, and 35.4%, respectively. In contrast, the cancer-specific mortality rates for the TD-negative group were 6.6%, 19.5%, and 27.2% at 1, 3, and 5 years, respectively. The TD-positive group had a higher rate of death attributed to other causes, such as heart diseases and diabetes (P = .022) (Figure 2(C)). Overall survival (A, B) and cause-specific mortality (C, D) of patients with different TD or PNI status after propensity score matching.
The median OS times were 71 months and 55 months for patients with PNI-negative and PNI-positive status, respectively. The PNI-positive group had a significantly worse OS rate (P < .001) and higher cancer-specific mortality rate (P < .001) than the PNI-negative group. The 1-, 3-, and 5-year OS rates were 85.6%, 62.2%, and 47.5% for the PNI-positive group and 87.6%, 68.7%, and 55.1% for the PNI-negative group, respectively (Figure 2(B)). The corresponding cancer-specific mortality rates for the PNI-positive group at 1, 3, and 5 years were 8.4%, 24.5%, and 34.8%, respectively. In contrast, the cancer-specific mortality rates for the PNI-negative group were 6.8%, 19.4%, and 27.6% at 1, 3, and 5 years, respectively. There was no significant difference in the number of patients who died due to other causes between these two groups (P = .452) (Figure 2(D)).
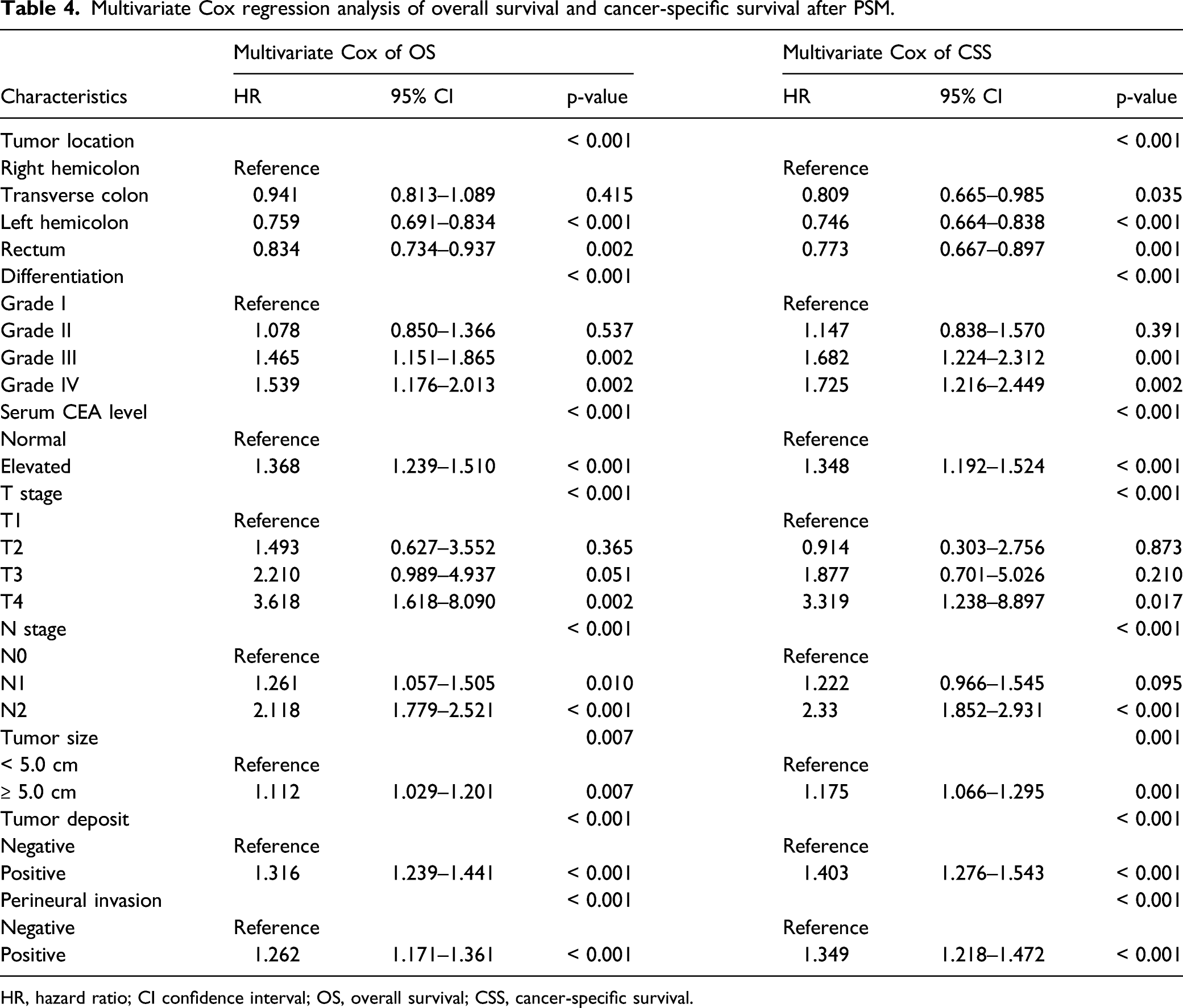
We also compared the adverse influence of TD and PNI on survival. As shown in Figure 3, patients with CRC simultaneously positive for TD and PNI had a worse 5 year OS rate than the other three groups (73.8% vs 65.5% vs 64.0% vs 55.3%, P < .001). Patients who were positive for TD or PNI had similar 5-year OS rates (P = .300) (Figure 3(A)). A similar pattern was observed with respect to cancer-specific mortality (Figure 3(B)). We further quantitatively analyzed the impact of TD and PNI on survival through Cox regression analysis. As shown in Table 4, the HR values of TD and PNI for OS were 1.316 and 1.262, respectively (P < .05). For cancer-specific survival, the HR values of TD and PNI were 1.403 and 1.349, respectively (P < .05). Overall survival (A) and cause-specific mortality (B) for patients with different TD and PNI status after propensity score matching. Multivariate Cox regression analysis of overall survival and cancer-specific survival after PSM. HR, hazard ratio; CI confidence interval; OS, overall survival; CSS, cancer-specific survival.
Subgroup Analysis
TD and PNI were significantly associated with N stage and T stage. However, it is not clear whether the impact of TD and PNI on patient survival changes with different TNM stages. Hence, we stratified matched patients into subgroups with respect to T stage and N stage. As shown in Figure 4 and Supplementary Figure S3, patients who were simultaneously positive for TD and PNI had the worst 5 year cancer-specific survival, and the survival curves of patients with stage III CRC in the TD−PNI+ group overlapped that of those in the TD+PNI− group. Cancer-specific survival of patients with different TNM stage.
Because TD and PNI status were also correlated with histological differentiation, patients who had a poor differentiation grade were more likely to be TD-and PNI-positive. We also investigated whether the impact of TD and PNI on patient survival would change with different histological differentiation. Grade I (well differentiated) and Grade II (moderately differentiated) were grouped as “well differentiated”. Grade III (poorly differentiated) and Grade IV (undifferentiated) were classified into the “poorly differentiated” group. Patients in the TD+PNI+ group had the worst prognosis. Patients in the TD-positive or PNI-positive groups had comparable outcomes (Figure 5). The same pattern was observed with respect to different tumor locations (Figure 6). Cancer-specific survival of patients with different differentiation grade. Cancer-specific survival of patients with different tumor location.

From the above subgroup analysis, we found that the adverse impact of TD and PNI did not change with TNM stage, histological differentiation, or tumor location. Hence, TD and PNI status were independent prognostic factors associated with worse survival.
Discussion
In this study, we compared the impact of TD and PNI on the survival of patients with non-metastatic CRC in 1849 pairs of matched patients by using PSM to balance the baseline covariates. We found that the long-term survival outcomes of patients in the TD+PNI− and TD−PNI+ groups were comparable, and that those in the TD+PNI+ group had the worst 5-year OS and 5-year cancer-specific mortality rates. To the best of our knowledge, this is the first study comparing the survival impact of TD and PNI with such a large population.
The former largest population study investigating the prognostic value of TD and PNI enrolled approximately 60 495 cases. 12 However, approximately 30% of cases in that study lacked information on TD status or PNI status, and the baseline covariates were not balanced. Thus, that study did not compare the prognostic impact of TD and PNI. In our study, we enrolled 70 689 CRC patients with complete data, and the baseline covariates were well balanced through PSM with a standardized difference of less than 5%.
In addition, we utilized competing risk analysis to estimate the cancer-specific mortality associated with TD and PNI. Competing risk analysis has been used in the analysis of survival data in recent years. The primary event of interest is often precluded by competing events. For example, if the primary event of a study is death attributed to CRC, death due to non-CRC diseases, such as cardiovascular diseases, is a competing event. The occurrence of competing events leads to the overestimation of CRC-specific survival. Competing risk analysis can reduce the overestimation of cancer-specific mortality.13,14 Our use of the largest population to date in combination with the aforementioned statistical methods increases the reliability of our research.
Several studies have investigated risk factors associated with TD and PNI. These studies identified age, T stage, N stage, and differentiation grade as risk factors.15-17 Our result is consistent with those studies, except for age. This difference may result from population size and different demarcation of age.
Interestingly, our study found that TD and PNI status differed by tumor location. The positive rate of TD and PNI increased from the right hemicolon to the rectum (for TD, right hemicolon: reference, transverse colon: OR = 1.199, left hemicolon: OR = 1.356, rectum: OR = 1.718). This phenomenon has only been reported in one other study. Kim CW et al reported that the extra nodal extension rates differed significantly among patients with right colon (36.9%), left colon (42.6%), and rectal (48.7%) cancers. 18 The mesentery becomes thinner from the right hemicolon to the left hemicolon and ends at the rectum. Thus, rectal cancer is more likely to be TD- and PNI-positive. Another interesting finding of our study is the relationship between tumor size and PNI status. We found that patients with tumor sizes less than 5.0 cm were more likely to be PNI-positive. This may be caused by the aggressive feature of small size tumor. Several studies suggested that small size tumor had worse survival compared with large size tumor, if the TNM stage of CRC patients were similar.19-23
Our study also quantitatively analyzed risk factors related to TD and PNI status through bivariate logistic regression analysis. For TD, the most important risk factor was N stage. With respect to PNI, the most significant factor was T stage. The relationship between TD and N stage has been reported. 12 However, the most significant risk factor for PNI has never been reported.
TD and PNI are associated with poor disease-free survival and OS. As two different types of locoregional spread pathway, TD and PNI have their own characteristics. It was reported that TD in combination with lymph node metastasis was a strong predictor for liver (odds ratio [OR] = 5.5), lung (OR = 4.3), and peritoneal metastases (OR = 5.5). 15 As for PNI, a meta-analysis involving 22 900 patients demonstrated that PNI was significantly correlated with increased local recurrence (risk ration [RR] = 3.2, 95% CI: 2.33–4.44). 24 Nozawa H et al retrospectively reviewed 496 patients with pathological T3 or T4 colon cancer who did not receive preoperative treatment, and found that obstruction was more frequent in PNI-positive group than PNI-negative group (39 % vs 24%, P < .05). 25 He also reported that colitis-associated CRC was more likely to be PNI-positive, compared with sporadic CRC without obstruction (90% vs 45%, P = .007). 26 Some research investigated the onset of TD and PNI from the view of genetic mutation. A high BRAF mutation rate was observed in TD-positive patients. 27 Compared with PNI-positive patients, the expression of FLT1, FBXW7, FGFR1, SLC20A2, and SERPINI1 was significantly up-regulated in PNI-negative group. 28 However, detailed molecular mechanism of TD and PNI still remains unclear.
In the 8th edition of the AJCC TNM staging system for CRC, TD is considered only if lymph node metastasis is absent and is classified as N1c. Nagtegaal ID et al found that allocating TD into the nodal category N1c and only considering TD in the absence of lymph node metastasis resulted in the loss of valuable prognostic information. 15 Delattre JF et al proposed that TD should be added to the TNM staging system to better define the duration of adjuvant chemotherapy for patients with stage III CRC. 29 For CRC patients with T3–4 stage, positive TD status, and none lymph node metastasis, combined chemotherapy regimen is recommended. Our study demonstrated that the adverse impacts of TD and PNI on the survival were comparable. Hence, we proposed that CRC patients of T3-4N0M0PNI+ should be also treated as stage III. Combined chemotherapy regimen is recommended. We also found that patients in the TD+PNI+ group had the worst outcome. Based on the IDEA research, we proposed that 6 months of adjuvant chemotherapy regimen would be rational for CRC patients with both TD and PNI positive.
This study has several limitations that should be noted. First, the detailed information about surgery was not recorded in the SEER database. The extent of lymph node resection was not clear. Patients with CRC who received D3/D2 lymphadenectomy have superior OS.30-32 To avoid this limitation, we only enrolled patients with at least twelve harvested lymph nodes. Second, detailed information about chemotherapy was not recorded in the SEER database. We do not know whether the patients’ adjuvant chemotherapy was complete and standard. Third, our study was retrospectively designed, and some bias existed. To avoid this limitation, we utilized the PSM method. However, the limitation associated with PSM is inevitable. It is possible that residual confounders between the groups could have been omitted in the analysis.33,34 In addition, RAS gene status and MSI/MMR status, which influences the survival of patients with CRC,35-37 were not recorded in the SEER database, so these baseline factors were not analyzed in this study.
Conclusion
The adverse impacts of TD and PNI on the survival of patients with non-metastatic CRC were comparable. CRC patients with both TD and PNI positive had the worst survival outcome.
Supplemental Material
sj-pdf-1-ccx-10.1177_10732748211051533 – Supplemental Material for Tumor Deposits and Perineural Invasion had Comparable Impacts on the Survival of Patients With Non-metastatic Colorectal Adenocarcinoma: A Population-Based Propensity Score Matching and Competing Risk Analysis
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211051533 for Tumor Deposits and Perineural Invasion had Comparable Impacts on the Survival of Patients With Non-metastatic Colorectal Adenocarcinoma: A Population-Based Propensity Score Matching and Competing Risk Analysis by Bin Luo, Xianzhe Chen, Guanfu Cai, Weixian Hu, Yong Li1, and Junjiang Wang in Cancer Control
Footnotes
Acknowledgment
We acknowledged Miss Zhan for contribution to figure editing.
Author Contributions
BL and XZC collected the data. BL analyzed the data, reviewed the literature, and contributed to the manuscript drafting. JJW and WXH revised the manuscript. GFC is responsible for quality control. YL is responsible for research design and revision of the manuscript. All authors issued final approval for the version to be submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by Science and Technology Program of Guangzhou (NO.: 201904010020), and Funding for Outstanding Young Medical Talents of Guangdong Province (KJ012019439)
Ethics Approval
The approval for use of all the data was obtained through a request submitted to the SEER database. There was no need to get approval from the institutional review board.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.