
Abstract
Objective
This study aims to explore the expectations of physiotherapeutic treatment of long-term side effects (LTSEs) after cancer among patients treated in physiotherapy clinics.
Methods
This a qualitative interview study based on a phenomenological approach. Adult patients with LTSEs after cancer were recruited through The Danish Cancer Society and a private physiotherapy clinic in Denmark. Individual semi-structured interviews were carried out using Microsoft Teams based on an interview guide piloted before the interviews. Interviews were audiotaped and transcribed verbatim. Sampling was conducted with a focus on variation in LTSE. The data were analyzed using Malterud’s principles of systematic text condensation and coded in NVivo 12.
Results
2 males and 8 females with an average age of 55.8 years were interviewed for between 40 and 60 minutes from October to November 2020. Four main themes emerged from the interviews 1 : The importance of the physiotherapist’s approach, 2 the benefits of meeting patients with similar symptoms, 3 the importance of receiving knowledge, and 4 patients seeking to maintain their current state more often than aiming to improve their condition.
Conclusions
Patients consulting a physiotherapy clinic with LTSE after cancer prefer the physiotherapist to have knowledge about cancer and to be emphatic. Furthermore, patients prefer to meet like-minded people and expect support to maintain their current condition rather than improve their condition.
Introduction
The worldwide 5-year prevalence of cancer is almost 5 in 1000 and is slightly more prevalent among women than men. 1 After receiving a cancer diagnosis, the global 5 year net survival rate is estimated at 42.6%, with survival in high-income countries being higher than in low-income countries. 2 The number of cancer survivors continues to increase because of both advances in early detection and treatment. 3
Long-term side effects (LTSEs) can be defined as “a problem that is caused by a disease or treatment of a disease and may continue for months or years.” 4 Among cancer survivors, about 86% experience one side effect and fatigue is the most reported side effect in cancer or cancer treatment. 5 Other common LTSEs are tight surgical scars, lymphedema, pain, reduced function, sexual problems, anxiety, and depression. These often have a significant impact on the quality of life and overall mortality. 6 In addition, socio-demographic and psychosocial factors are important to consider when identifying people at risk of long-term LTSE. 7
Patients express needs for healthcare support to cope with LTSEs and almost 30% of all patients express a need for physical rehabilitation to address physical deficits after ending cancer treatment. 8 Consequently, patients are often referred to physiotherapists for the treatment of pain and other LTSE. Physiotherapeutic treatment is found to be effective,6,9 and physical therapy is even reported as most relevant among people with higher numbers of LTSE. 10 However, physiotherapists are often not aware of the relationship between cancer and the symptoms that present. If they are aware, they are unsure of the choice of treatment. This may lead to overestimated goalsetting for rehabilitation and unrewarding results for patients. 11 In the literature, most physiotherapy-led interventions include exercise alone or as part of multicomponent intervention programs. 12 Physiotherapy interventions with endurance training, aerobic exercise, and resistance training are found relevant and effective in the treatment of LTSEs in cancer survivors.13,14 However, lymphatic drainage interventions after axillary lymph node dissection for breast cancer have not been found to be effective. 15
Previous research has shown that some patients feel isolated and, therefore, benefit from training while others highlight the importance of professional and being involved in exercise like walking and running to tailor physical activity to suit patients with LTSE. 15 Furthermore, qualitative research has shown positive experiences of team training because of the opportunity for social interaction and discussions of common questions and concerns with other cancer survivors. 16 Additionally, qualitative research has found that individually tailored courses addressing individual needs effectively facilitate physical activity among women even though they may suffer from cancer-related fatigue. 17
The body of evidence for treating LTSE is, however, limited, and further knowledge on treating this increasing group of patients in physiotherapy is needed to gain insight and to improve the physiotherapeutic treatment of LTSE. Hence, this study aims to investigate the expectations of physiotherapeutic treatment among patients with LTSE.
Methods
This is a qualitative study of patients with LTSE in physiotherapy practice is reported according to the consolidated criteria for reporting qualitative studies (COREQs). 18
Study Design
This is an interview study focusing on the participants’ experienced lifeworld as the specific reality in which they live their lives. The study is thereby inspired by the phenomenological approach where the preunderstanding was sought to be put aside. 19 RKJ, SJ, and SVG wrote down their preunderstanding and saved these prior to interviewing. They had chosen this subject based on their interest to the field, which had arisen during their clinical practice training.
Research Team and Reflexivity
This interview study has been conducted as part of a larger research project about developing interventions to improve primary care treatment of LTSE in Denmark. The wider research project was conducted in collaboration with the Department of Physiotherapy at University College in Northern Denmark, The Research Unit for General Practice at the Department of Clinical Medicine in Aalborg, the Quality Unit for General Practice in the North Denmark Region, and DEFACTUM (a public research institution in Denmark focusing on increasing social equality in health). RKJ, SJ, and SVG were supervised by MFA (Lecturer at UCN, PT, MSc), MK (Regional consultant for primary care physiotherapy, PT, MPQM), JLT (Professor, GP, PhD), and AR (Lecturer at UCN, Senior researcher, PT, PhD).
RKJ, SJ, and SVG received information about participants agreeing to participate from MK and AR. They repeated study information and scheduled an appointment for interviewing. RKJ, SJ, and SVG had no prior knowledge about the participants. The participants knew this study was part of RKJ’s, SJ’s, and SVG’s thesis and they were informed that the interview study was part of a research project to provide information on the development of interventions to patients and possible educational interventions to clinicians.
SJ conducted all interviews. She did this during her physiotherapy studies where she completed her final thesis in collaboration with RKJ and SVG. She had no prior experience in interviewing. However, she had received training in interview techniques such as open-ended questions, active listening, and probing as part of her theoretical and clinical training as a physiotherapist.
Sampling
Danish-speaking cancer survivors experiencing either lymphedema, pain, fatigue, reduced balance or reduced mobility, aged 18+ years, and treated for LTSE by physiotherapists working in the Danish physiotherapy clinics fulfilled inclusion criteria and participants with some form of cognitive impairment or mental disorder were excluded. Sampling was aimed to achieve a maximum variation on types of LTSE.
Method of Approach
Information about the study was displayed in different relevant groups, an email was sent to 118 physiotherapists in the North Denmark Region and directly to patients via social media. They responded to MFA and MK, who gave contact information to RKJ, SJ, and SVG. RKJ, SJ, and SVG contacted patients by email or phone to further inform about the study and eventually schedule an appointment for interviewing.
Sample Size
A prior we had decided on a minimum of 8 interviews with an aim to reach saturation. Saturation was discussed between RKJ, SJ, SVG, and MFA.
Non-Participation
Among twelve participants contacted to participate in an interview, one was excluded because the person had not received treatment by a physiotherapist. Another rejected participation: This person was not interested in the subject.
Ethics
All patients gave written informed consent prior to enrollment in the study. This is a non-intervention and interview study and The North Denmark Region Committee on Health Research Ethics has stated that according to Danish law their approval is not needed.
The Setting for Data Collection
Interviewing was conducted online using Microsoft Teams. We expected all participants were in their own homes. However, we did not systematically plan to ask for this information. Interviews were audiotaped with a dictaphone and on a mobile phone as a back-up. We encouraged participants to be alone. Also, the interviewer (SJ) was alone during interviewing. Transcriptions were not returned to participants.
Data Collection
Interview Guide.
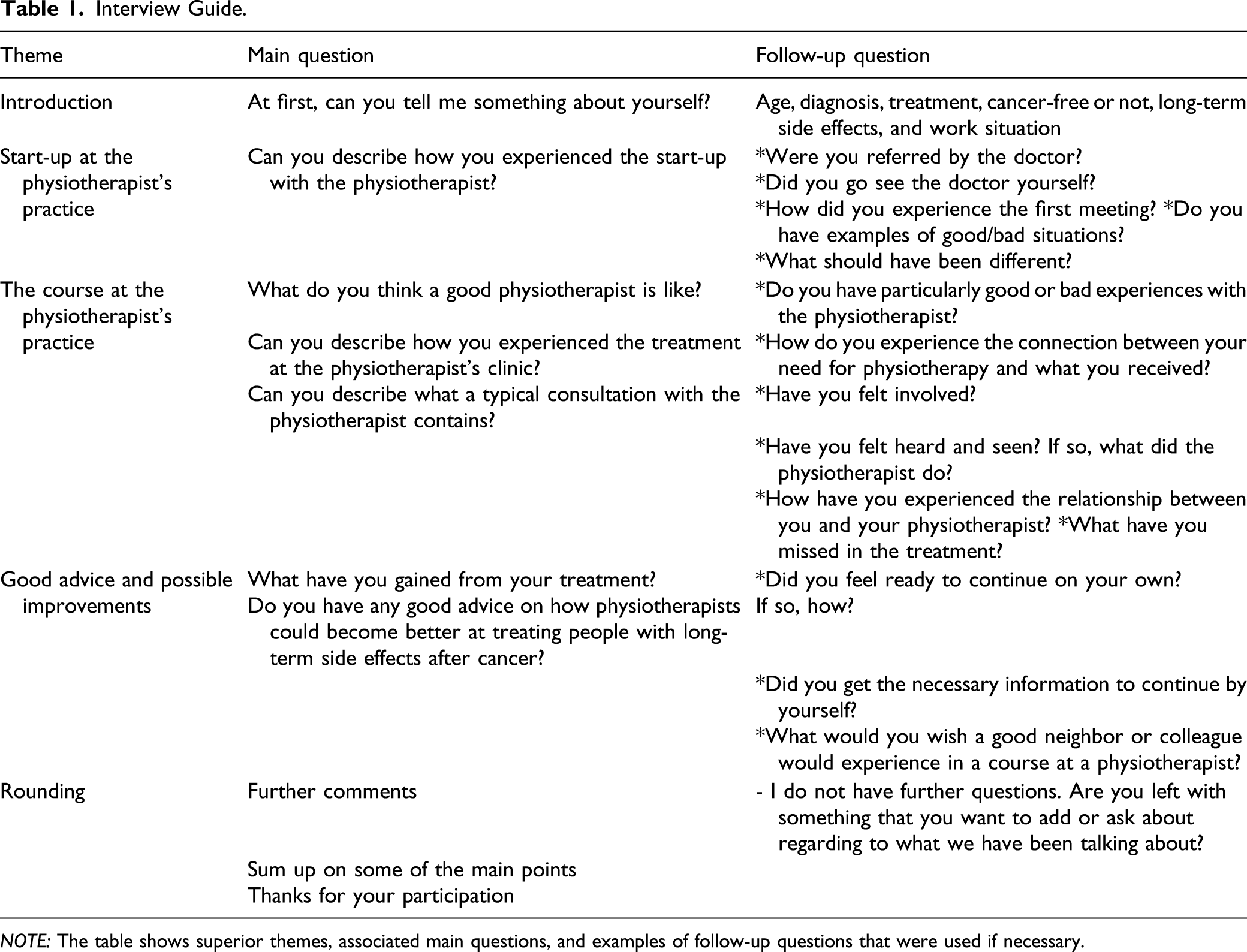
NOTE: The table shows superior themes, associated main questions, and examples of follow-up questions that were used if necessary.
The interview guide contained 3 topics and a few open-ended questions that the interviewer used as a start, after which follow-up questions were asked if necessary (Table 1). No field notes were made. The interview guide was pilot tested with SJ as an interviewer and MK as a respondent with RKJ, SVG, MFA, and AR present.
Data Analysis
NVivo software (NVivo 12) was used to code the meaningful units. Themes were thereby derived from data by use of Malterud’s principles of systematic text condensation were used to analyze data in rounds after 4, 8, and 10 transcriptions. 20
The total impression—from chaos to themes First, a data overview was established. RKJ, SJ. SVG individually read all the transcriptions to get a general impression of the content and then come up with preliminary themes. The data were considered with an open mind and an awareness of the participants’ own voices. The themes were discussed on multiple occasions until a consensus was reached on common themes.
Identifying and sorting meaningful units—from themes to codes RKJ, SJ, and SVG individually read the transcriptions line by line to identify and code meaningful units. The coding included identifying, classifying, and sorting meaningful units potentially related to the previously negotiated themes. The meaningful units were marked with a code. In this way, the related meaningful units were connected through code groups. The names of the code groups were elaborated from the preliminary themes in step 1.
Condensing—from code to meaning RKJ, SJ, and SVG individually went through one code group at a time to sort the meaningful units of the actual code group into a few subgroups. Afterward, these were discussed, and common subgroups were found for each code group. Then meaningful units were coded into subgroups. The procedure was then repeated with the remaining transcriptions in round 2 and 3. At last, a condensed form and headline for each code group and subgroup were created. For each condensed form, a quotation was picked out. This sought, as far as possible, to maintain the original terminology applied by the participant.
Synthesizing—from the condensed form to descriptions and concepts From the condensates and artificial quotations, analytic texts presenting the most salient content and meaning was written in third-person format, as RKJ, SJ, and SVG were in the roles of re-narrators responsible for interpretations. The analytic text for each of the code groups was reconceptualized, returning to the full transcript, where RKJ, SJ, and SVG validated whether the synthesis and the illustrative quotation still reflected the original context appropriately. Finally, a category heading to each analytic text was developed and also reconceptualized according to the full transcription. The category headings show the most significant interpretations and represent the final results of the analysis. In the result paragraph, these category headings are called themes and subthemes listed with the belonging analytic text. Following the analysis, an external person, not member of the author group, but experienced with qualitative research, read the transcriptions, and validated the result section, including the themes and subthemes.
Results
Characteristics of the Sample.

Note: N = 10. Sampling was aimed for maximum variation on type of long-term side effects.
Example of Coding.

Note: Overview of code- and subgroups, meaningful units, themes, and subthemes.
Theme 1. The Importance of the Physiotherapist´s Approach
Most of the participants experienced having met an empathetic, welcoming, and grateful physiotherapist. One participant expressed the importance of the physiotherapist being honest and direct in their communication. Besides, good collaboration involving the patient in a dialogue about goals and expectations was mentioned to be important. Further, it depends on getting to know each other. “I hope for a lovely and warm-hearted physiotherapist […] Of course, it’s fine to keep a certain distance, but it’s also nice to be close to your physiotherapist” (participant 2)
Subtheme 1a; Empathy and Acknowledgment
Several participants stated the importance of being seen and heard by an empathic physiotherapist with a perfect mix of personal and professional interests. Additionally, mutual respect is important regarding the feeling of being acknowledged and taken care of without being treated as a victim. Some prefer a physiotherapist who dares to address the psychological aspect and several expressed that honesty and direct communication in layman´s terms increase the patient’s confidence in the therapist. “Someone who understands what your problems are. I just felt that I was in safe hands with the physiotherapist. They listened and understood the problem” (participant 5)
Subtheme 1b; Involvement of Patients
Some participants did not receive the treatment they had expected. A participant stated that informing the physiotherapist about expectations might have positively changed the situation. Moreover, several expressed a desire of being involved in decisions and receiving information regarding treatment. Getting to know each other was mentioned to give the feeling of collaboration with the physiotherapist while also helping the physiotherapist to understand the individual. In connection with an experience of having to ask for new exercises, one of the participants considered it fair to take the initiative. “I’d probably expected that some massage might help but that wasn’t the case. I got some exercises, then, I was able to go home and do them. […] I’ve heard several acquaintances saying ‘but, he didn´t even touch me’” (participant 4)
Subtheme 1c; Individual Adjustment
For the participants, the ideal course is individually tailored. One participant had a physiotherapist who was able to vary the training, while others were annoyed by the idea of “one size fits all” and feeling incorrectly assigned to a team. Another participant had experienced that very few physiotherapists were giving a diagnosis and starting treatment based on a thorough examination. “In general, I might think that people are taking the easiest path. I don’t think it’s because people don´t want to listen, but I believe it’s easier to classify people more rigidly” (participant 6)
Theme 2. Meeting Like-Minded People and Being Understood
The participants described the social and enjoyable aspects of exercising with others, especially if the patient was feeling alone or having a hard time training alone. Several participants felt connected to other patients. Furthermore, they felt it was possible to share experiences and be understood when they were with other cancer patients. “We didn’t talk that much, but just a little. It was actually fine having a subconscious connection to a group that you know are going through the same as you” (participant 6)
Subtheme 2a; Social Cohesion
Several participants described the social aspects of being with others. A participant considered it particularly rewarding for people who spend a lot of time alone. Furthermore, social cohesion was stated as achieving higher success when a consistent group of people participated. Another participant considered that team training was an opportunity for completing exercise and that this had more value than the social aspect. A participant attending a social cycling team experienced it as a legitimate opportunity for getting into a little conversation. “Sometimes, we meet the same people, but not always as someone will switch between teams. There is not the same social cohesion as with aqua aerobics where the same people always show up” (participant 3)
Subtheme 2b; Being in the Same Situation
More participants described the feeling of synergy and a subconscious connection when being with others in the same situation who truly understand them. People had the experience of attending a team where you could contribute to anything relating to LTSE. This was elaborated by another who felt it rewarding to hear relatable experiences and identify with others. “I think that it might have given me a sense of connection by showing up and being with someone who had endured almost the same thing as me. They understand what it’s like to have cancer that others who’ve never had it don’t always understand” (participant 6)
Theme 3. The Importance of Knowledge
Several participants experienced a lack of knowledge with LTSE. However, some had good experiences where physiotherapists made an honest attempt to treat them despite having a lack of knowledge. “I probably know more about long-term side effects than many of the people I meet in the system. [...] Some of the physiotherapists where I go don’t know about long-term side effects and they are not specialised” (participant 3)
Subtheme 3a; Knowledge as a Safety
Some participants described a feeling of being in safe and competent hands when the physiotherapist has knowledge of working with LTSE and watches to make sure everything is going well. A participant considered it rewarding and calming to receive extra information about her specific situation. Most expressed the importance of being perceived as a whole person. Furthermore, a participant had experienced a more relaxed atmosphere at the physiotherapist´s compared to at the doctor´s. Also, this participant felt a respect for the fact that patients can also have important knowledge about their health condition. “Experienced physiotherapists have had someone like me in their hands before. It just gives me a feeling of being in safe hands” (participant 1)
Subtheme 3b; Physiotherapists Not Being Familiar With LTSE
Several participants expressed that many physiotherapists are not familiar with LTSE. A participant expressed a wish to know more about LTSE from personal experience, which many healthcare professionals do not have. However, the importance of trying and being honest when not having qualifications was mentioned, as it is fair that not everyone will know everything. A participant considered it was desirable that physiotherapists should seek more information and specialize in LTSE. “I don’t think that physiotherapists are aware that cancer demands something extra. [...] Radiation does something with the body and I don’t think they have much experience in that” (participant 7)
Theme 4. Maintenance Is More Important Than Improvement
Several participants experienced the effects of attending different treatment activities. A few had experienced treatments that were insufficient, but several agreed that their current treatment is predominantly maintenance. Several participants mentioned that treating LTSE is a lifelong project, which is why they request different tools to improve this lifelong treatment. “I experience the treatment as some kind of maintenance. I’m not quite sure things will get much better than they are now because of the body’s decay” (participant 2)
Subtheme 4a; Tools for a Lifelong Project
Several participants mentioned the importance of receiving tools to use at home as the damage from the radiation treatment never disappears. Moreover, one had obtained knowledge about exercises and techniques for massaging their surgical scar, and one participant experienced that more focus on the exercises resulted in a noticeable improvement. Furthermore, a couple of the participants described the value of receiving continuous supervision from a physiotherapist. “I feel like I’m being kept on track in relation to where I want to go. I also feel exercises are a tool that helps me cope” (participant 10)
Subtheme 4b; Investment in Well-Being
Most of the participants have experienced the effects of treatment. One woman talked about a great and surprising experience in loosening up a tight surgical scar, while another experienced that the physiotherapist was able to move the lymphatic fluid away. Some participants have experienced improved mobility, physical well-being, or softening of the muscles in the axilla. One woman described the feeling of being in a slightly small wetsuit that fits better after treatment. Furthermore, one described her body getting better when doing her exercises, while another mentioned the need to remind herself that treatment and exercising are good investments. “In practical terms, the muscles are loosened. […] when I come for treatment, I simply get improved mobility in my arm,” (participant 6)
Subtheme 4c; Chronic Pain as a Condition of Life
One man has concluded that massage does not help him. Several participants perceived massage more as a symptomatic treatment than a holistic treatment when experiencing LTSE. They expressed a perception that LTSE never disappears, regardless of the amount of massage received. One woman said that if she were a millionaire, she would visit a physiotherapist once a week because it would be more effective. However, another questioned whether physiotherapy made a difference. One man considered it important in trying to resign himself to the conditions of life that chronic pain inflicts, as otherwise, this might lead to psychological problems. “I’ve been seeing the same [physiotherapist] for one year and seven months and over the last year, I’ve probably thought that there wouldn´t be any change” (participant 2)
Discussion
Principal Findings
The aim of the study was to investigate what patients expect from physiotherapeutic treatment of LTSE in physiotherapeutic clinics. Throughout the analysis the following themes emerged: (1) The importance of the physiotherapist’s approach, (2) the importance of meeting like-minded people and being understood, (3) the importance of knowledge, and (4) maintenance is more important than improvement.
Strengths and Limitations
We used a data-driven step-by-step procedure that promotes transparency and supports the identification of the participants’ experienced lifeworld, putting our preunderstanding aside. 21 The interviewers’ position as a graduating student without any relation to the participants fostered an adequate distance between the interviewer and the participants. Hence, they did not need fear insulting a trained physiotherapist or someone they knew. A study limitation might be the limited diversity of the participants’ characteristics. Only 2 men were included and most of the female participants were diagnosed with breast cancer, which limits the gender diversity in the study and is a weakness in the study. Furthermore, being a qualitative study with 10 participants, findings from this study need to be supported by quantitative research into the external validity of the findings.
Transcripts were not sent to participants for feedback, which may have improved internal validity. However, to address this limitation, an external person was used to validate the results. This led to minor adjustments to the text. However, themes and subthemes were not changed. We believe this to strengthen the study and reduce the risk of bias. Before interviewing, RKJ, SJ, and SVG stated their preunderstanding. Even though some findings are in line with their stated preunderstanding, new knowledge did arise during this study. Quotations are translated from Danish to English, however, cautions were taken in keeping the participants’ meanings. However, interviewing in one language and reporting in another is a limitation of the study.
Comparison With Previous Studies and Theories
Importance of the physiotherapist’s approach
This theme can be related to the Calgary–Cambridge Guide, an evidence-based communication model that provides the framework for professional health communication. 22 Several informants mentioned the importance of meeting a physiotherapist who is empathic, generous, and appreciative, showing personal and professional interest, which are keywords in the first phase of the Calgary–Cambridge Guide and are in line with patients' preferences for their physician.22,23 Furthermore, the Calgary–Cambridge Guide focuses on dialogue regarding goals and expectations and delivering information that allows the patient to be involved in shared decision-making. 24 Others have also found that patients with cancer prefer involvement in medical decisions. 25 This involvement in physiotherapy includes using an individualized treatment approach, offering education during all aspects of treatment and working with patient-defined goals by a physiotherapist with sufficient social skills in addition to showing specific knowledge about cancer. 26
Meeting like-minded people and being understood
Some of the participants describe team training as a way for social cohesion to arise. Furthermore, they find it essential to discuss questions and thoughts with someone in similar life situations. These findings are supported by a study where women experienced social interaction with other cancer survivors as positive and having the opportunity to discuss common issues and concerns. 16 According to the Self Determination Theory, the 3 basic psychological needs underlying intrinsic motivation are: autonomy, competencies, and relatedness. These are considered important for this patient group. 27 In this case, the feeling of relatedness is met by being able to relate to others, feeling safe, and being connected with the surroundings. This promotes an intrinsic motivation to continue training and obtain long-term exercise adherence. 28 The importance of being treated with others can also be found in a hospital setting 29 where support from other participants was a key facilitator in overcoming challenges such as fatigue and mental issues. 29
The importance of knowledge
Varied perspectives on physiotherapists’ knowledge about LTSE appeared in this study. Obtaining greater knowledge and insight could meet the participants’ basic psychological needs, autonomy, and competencies, which are described as important in the Self-Determination Theory. 27 Receiving relevant information can improve the participants’ competences for attending their treatment and making decisions that could give them the feeling of ownership of the situation and believing in their abilities. The participants’ statements regarding the importance and feeling safe with physiotherapists delivering information are supported by a qualitative study of women with breast cancer, 16 concluding that it felt safe and calming to receive relevant knowledge about the intervention. A recent review found that internet-based programs are effective in reducing LTSE. 30 Maybe physiotherapist should be more aware of advising patients to seek information online in combination with their treatment. However, it is important to recommend specific homepages, otherwise patient’s lack trust in information from the Internet. 31
Maintenance is more important than improvement
Not all participants had experienced an improvement in the treatment they received. However, it was more important for them to maintain their level of health and for symptoms not to increase. Several of the participants who did not experience an improvement mentioned an awareness of things not being much better. This is in line with findings from a previous study where even patients who were highly motivated to exercise did not hold strong beliefs that exercise would decrease LTSE. 32
This highlights the importance of the recommendations in the Calgary–Cambridge Guide, emphasizing that physiotherapists need to match expectations and involve the patient to ensure common thoughts about the choice of treatment and treatment goals. 22
Implications for Practice
The findings of this study highlight various factors that could improve the experience of physiotherapeutic treatment of LTSE. First, physiotherapists should meet patients with a holistic and biopsychosocial approach. Second, patients could benefit from being involved in decisions about their treatment and treatment goals by an emphatic physiotherapist. Third, special attention is needed for the participants concerning their feelings about being abandoned by the health care system with LTSE. The participants’ experiences of the physiotherapist’s knowledge was varied. Even when physiotherapists had insufficient knowledge, several participants accepted this if the physiotherapist was honest about it. Still, most of them expressed a desire for physiotherapists specializing in LTSE. Patients’ expectations for maintaining their functional levels rather than improving their condition was not included in our preunderstanding and was a surprising finding. However, findings from this qualitative phenomenological study need to be supported in future research and call for quantitative research to quantify this belief/expectation. This is a widely spread belief that actions are needed since exercise decreases the risk of mortality and recurrence while also being associated with less severe LTSE. 33 In addition, intervention studies are generally small and rarely have long follow-up periods34,35; consequently, future studies on effects need to be large scale and report long-term follow-up.
Conclusion
Patients consulting a physiotherapy clinic with long-term side effects after cancer prefer the physiotherapist to have knowledge about cancer and to be emphatic. Furthermore, patients prefer to meet like-minded and expect support to maintain their current condition rather than necessarily improve it.
Clinical Messages
1. Patients seek information about LTSE after cancer from physiotherapists. 2. Patients aim to maintain their level of function and symptoms rather than improve these.
Footnotes
Acknowledgments
The authors thank Laura Hvidaa Hjoernholm at the Quality Unit for General Practice in the North Denmark Region for reading transcription and validating the result section.
Author Contributions
RKJ participated in the conception of the study, transcription, analyses, and interpretation of data. RKJ participated in drafting the first version of the paper and took a lead in co-ordinating rounds of corrections. RKJ drafted the last version of the manuscript and read and approved the last version of the manuscript. SJ participated in the conception of the study. SJ conducted all interviews and participated in transcription, analyses, and interpretation of data. SJ participated in drafting the first version of the paper and read and approved the last version of the manuscript. SVG participated in the conception of the study. SVG participated in the transcription, analyses, and interpretation of data. SVG participated in drafting the first version of the paper and read and approved the last version of the manuscript. MFA participated in the conception of the study. MFA participated in the interpretation of data. MFA participated in commenting on the manuscript in rounds of corrections for the paper and read and approved the last version of the manuscript. MK participated in the conception of the study. MK assisted in recruiting participants and acted as a respondent in the pilot interview. MK participated in commenting on the manuscript in rounds of corrections for the paper and read and approved the last version of the manuscript. JLT participated in the conception of the study. JLT participated in commenting on the manuscript and in rounds of corrections of the paper and read and approved the last version of the manuscript. AR participated in the conception of the study. AR participated in the interpretation of data and commenting on the manuscript in rounds of corrections for the paper. AR supervised RKJ in drafting the final version of the manuscript and reading and approving the last version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Cancer Group of Nord-KAP in the North Denmark Region. The group works to support a coherent, end-to-end treatment of patients with cancer. They had no role in conceptualizing the study, collecting, and interpreting the data. They did not participate in writing the paper and did not participate in the decision to submit the paper.