
Abstract
Introduction
Individuals diagnosed with cancer are living longer due to improved screenings and treatments, 1 leading to many cancer survivors with unique cancer-related needs which must be cared for alongside other comorbidities. 2 Oncology has largely assumed responsibility for providing survivorship care through survivorship clinics and programs within cancer centers. 3 However, for nearly 20 years, governmental and professional organizations have called for increased integration and engagement of primary care in cancer survivorship,4,5 with the aging population of cancer survivors further exacerbating this need. 6 Primary care plays a unique role in the longitudinal care of individuals, providing whole-person care and taking responsibility for most health needs. 7 Prior research has found only a minority of oncologists agree primary care has the necessary skills to provide follow-up for individuals with a history of cancer.8,9 Still, most oncologists acknowledge a significant proportion of their patients could be transferred to primary care, and primary care is better suited to addressing non-cancer comorbidities. 8
Despite calls for increased primary care involvement in survivorship, significant challenges remain and there has been limited research on the perspectives of oncologists about the challenges of engaging primary care in survivorship. 10 In this study we sought to understand the perspectives of oncologists practicing at NCI-designated comprehensive cancer centers (NCI-CCCs) on the role of primary care in adult cancer survivorship. These NCI-CCCs are leaders in cancer research innovation, recognized for excellence in research, education, and clinical care as well as cancer prevention, diagnosis, and treatment; 11 however, their role in cancer survivorship is still emerging and perspectives of practitioners within these institutions is unknown.
Methods
As part of a larger NCI-funded study, we conducted qualitative in-depth interviews with medical oncologists regarding their perspectives on the role of primary care in cancer survivorship. Participants were nominated by the grant's national advisory committee or a cancer survivorship proponent because of their reputation for interest in cancer survivorship and contacted via email by a researcher on the study team. Interviews were conducted by one of the authors (JH) between December 2021 and June 2022 via Zoom. Interviews were between 30 and 60 minutes and were conducted using an open-ended semi-structured interview guide asking questions about cancer survivorship care at the participants institution and their perspective on role of primary care. Questions from the interview guide are included in Figure 1. Interviews were transcribed verbatim. This study was approved by the institutional review board of Rutgers University (#2021000838) on 06/09/2021 and all participants provided verbal consent. Participants received a $30 incentive for participation. We adhered to the Standards for Reporting Qualitative Research (SRQR) reporting guidelines.
12
Open-ended semi-structure interview questions.
Analysis
Data analysis used a collaborative, interpretative process called “immersion/crystallization.” This was an inductive process in which four of the authors, three of whom were PhDs experienced in qualitative research, went through iterative cycles of repeated readings through transcripts and summaries of each interview until salient themes emerged. 13
Each transcript was reviewed separately as an individual case and read by the authors together in multiple passes during debriefing sessions. Interview summaries of approximately 3–5 pages highlighting approaches to cancer survivorship and primary care were written collaboratively to organize the data and highlight themes. When all interviews had been discussed and summarized, summaries were used to identify cross-case comparisons. Themes that emerged from individual interviews were discussed and compared in the context of themes from other interviews by the authors until consensus was achieved. Immersion/crystallization does not require a formal coding structure, but rather allows for dynamic interaction throughout the interpretation process through these multiple collaborative, iterative cycles of analysis.13,14 We have reported these methods consistent with the COREQ Qualitative Checklist.
Results
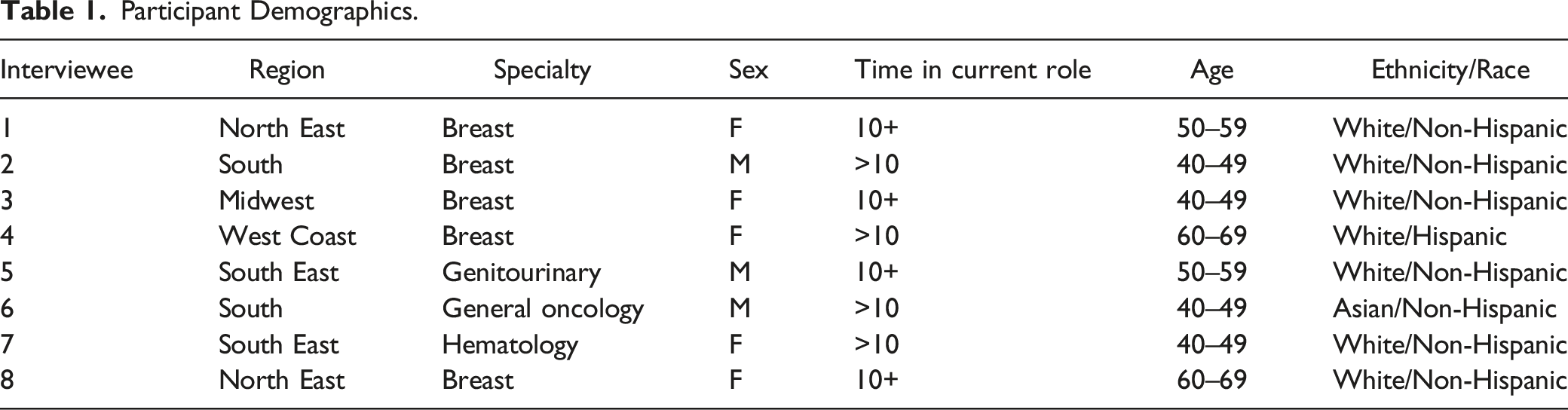
Participant Demographics.
Even survivorship-championing oncologists from NCI-CCCs lacked consensus about the role of primary medical care in cancer survivorship. Two salient themes emerged through the analysis. (1) Medical oncologists have diverse perspectives on if, how and when primary medical care should be involved in survivorship and the overarching role of primary care clinicians in survivorship.
Various opinions were presented on when primary care should be involved in survivorship. Several participants suggested primary care clinicians should be involved with oncology from diagnosis through continuous conversation about shared patients. As one interviewee noted, “So my hope would just be more continuous engagement with primary care will help that because then they’ll be part of the process instead of kind of a before and after” #7. Another participant felt primary care should be “at the table with the oncology team up front” #5. However, these attitudes contrasted with others who believed patients should remain in the care of oncology and did not mention primary medical care involvement. “But historically, we keep those patients in the survivorship clinic indefinitely. And we don’t discharge patients from that clinic” #6. Others explained individuals remain in oncology for an extended period, typically at least 5 years post-treatment, but there were plans for a hand-off back to primary medical care at some point.
These differing opinions inform the language used to discuss survivorship. Some participants stated there should be a “transition” of patients back to their primary care clinician, inferring primary medical care was not involved while the patient was receiving oncology care. Others noted the goal should be “co-management” between oncology and primary care. These attitudes inform emerging models of survivorship care in NCI-CCCs. As one participant explained, at their institution primary medical care was left out of the conversation about survivorship from the beginning of program planning. “I would tell you that when we formed our… survivorship program committee… One of the things that we are missing in that crowd is a primary care physician” #2. Another noted while their organization sponsors research conferences and lectures about survivorship they are not developed for primary care clinicians. (2) Medical oncologists lacked recognition about the expertise and value of primary care.
Throughout these interviews, participants demonstrated a lack of understanding about primary care clinician’s expertise. For example, interviewees discussed treatment summaries or care plans designed to be given to primary care clinician’s that include all preventive care needs. Preventive care is primary medical care’s domain, and treatment summaries need to provide actional information beyond the routine health maintenance primary care is already knowledgeable about. As 1 interviewee noted, “And there’s some [oncologists] who feel that no, I’m the expert in this disease and I have a relationship with patients. Why should they see anybody else?” #4. There was evidence this lack of understanding about primary care’s expertise may translate into a lack of trust that primary care is qualified to care cancer survivorship. “I actually think sometimes patients don’t have a strong primary care doctor or I’m worried that something is gonna get missed” #3.
Communication issues between oncology and primary care have been previously documented and arose in these interviews. The lack of communication between oncology and primary care may reinforce oncology’s lack of understanding about what primary care does, and in turn, may perpetuate a system where oncology does not engage primary care because they do not understand their value.
Conclusion
These interviews with practicing medical oncologists from NCI-CCCs illustrate a lack of a coherent messaging regarding primary care’s role in cancer survivorship. These NCI-CCCs were created to improve understanding in cancer diagnosis and treatment, which they have accomplished with great success. However, survivors may have different needs at various phases, and care needed during treatment may differ from care required years later when long-term effects are the primary concern. 15 Many needs of survivors are already addressed by primary care, 16 but these interviews suggest a lack of understanding about the role and expertise of primary care in this area. Solutions including survivorship care plans have been attempted, but with limited success, 17 suggesting the need for more specific instruction and other avenues of communication. It has been nearly 20 years since the first calls for primary care engagement in cancer survivorship, but little will change until primary care is involved in the conversation.
Limitations
This study has several important limitations, primarily its small sample size. Additionally, while this study involved a diverse group of oncologists from different institutions with varying experience, these individuals do not represent all individuals from their institutions and were mostly breast oncologists.
Footnotes
Acknowledgments
This research was supported through grants from the National Cancer Institute (R01 CA257197). This work also benefited from support from the Cancer Center Support Grant (P30-CA072720) to Rutgers Cancer Institute of New Jersey, Dr. Hudson’s time was in part supported by the National Center for Advancing Translational Sciences (NCATS) a component of the under award number UL1TR003017. Ms. Barry’s time was supported by the Summer Student Research Training Program at the Rutgers, RBHS-Robert Wood Johnson Medical School.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grants from the National Cancer Institute (R01CA257197, P30CA072720).
Ethical Approval
This study was approved by the Rutgers University Institutional Review Board (#2021000838).
Informed Consent
Informed consent was not sought from patients included in this article. No patient participation was required, and all relevant patient information was de-identified.