
Abstract
Purpose:
Today, cancers have become a major cause of mortality in developed and developing countries. Among various cancers, gastric cancer imposes a huge economic burden on patients, their families, and on the health-care system. This study aimed to determine the economic burden of gastric cancer in Kohgiluyeh and Boyer Ahmad province of Iran in 2016.
Methods:
This was a cross-sectional cost of illness study conducted in Kohgiluyeh and Boyer Ahmad province of Iran in 2016, using a prevalence-based approach. All patients were studied using the census method (N = 110). The required data on direct medical, direct nonmedical, and indirect costs were collected using a data collection form from the patients’ medical records, tariffs of diagnostic, and therapeutic services approved by the Ministry of Health and Medical Education in 2016.
Results:
The total cost and burden of gastric cancer in Kohgiluyeh and Boyer Ahmad province of Iran in 2016 were $US436 237, among which the majority were direct medical costs (59%). The highest costs among direct medical costs, direct nonmedical costs, and indirect costs were, respectively, related to the costs of medications used by the patients (35%), transportation (31%), and absence of patients’ families from work and daily activities caused by patient care (56%).
Conclusion:
Our study has revealed for the first time high costs of gastric cancer in Iran. To decrease the total costs and burden, the following suggestions can be made: increasing insurance coverage and government subsidies for purchasing necessary medications, providing the required specialized care and services related to cancer diseases such as gastric cancer in other provincial cities rather than just in capital cities, and so on.
Introduction
Cancer is the second cause of death globally, 1 and the number of people with cancer is increasing. 2 Historically, gastric cancer has been one of the major causes of deaths due to cancer in the world. 3 Gastric cancer is the fifth most common cancer in the world, and more than a million new cases are detected every year. The incidence of gastric cancer is particularly high in East Asia, followed by Central and Eastern Europe, and South America. 4 Gastric cancer is one of the main causes of death due to cancer in the 21st century. It is anticipated that by 2030, gastric cancer will be one of the main causes of mortality in the world, and by 2050, there will be 2.5 million new cases and 1.9 million deaths. The prognosis of this disease is poor, and its 5-year survival rate in most countries ranges from 10% to 40% and is around 20% in most developing countries, while in Japan it is 40% to 60%. In Iran, the 5-year survival is relatively low at 28%. 5 ,6 Gastric cancer has remained a major public health issue worldwide, despite a steady reduction in its incidence and mortality rate in the past 30 years. Annually, more than 870 000 new cases of this disease are reported in the world, and more than 650 000 people in the world die due to this cancer. The estimated incidence rate in Iran is about 7300 cases per year and is the first cause of cancer deaths in both genders. 7 In Iran, according to the Iran Cancer Research Center, gastric cancer is the most common cancer in men and the third most common cancer in women after breast and colon cancers. 8 Furthermore, based on the official statistics of the Ministry of Health and Medical Education, over the past few years, especially since the beginning of the 2010s, cancer and, more commonly, gastric cancer in the province of Kohgiluyeh and Boyer Ahmad have been widespread. According to the data registered in the Iran Cancer Registration System affiliated to the Health Deputy of Yasuj University of Medical Sciences in 2016, the total number of patients with cancer in this province was 446, of which 155 people, that is, about one-third of all cancers, had been diagnosed with gastric cancer. The number of patients with gastric cancer registered in this province over the past few years has shown an increasing trend. 3 Gastric cancer is a multifactorial disorder, with aging, male sex, lifestyle, environmental and genetic factors, and Helicobacter pylori infection among its known risk factors. 9 Gastric cancer is characterized by nonspecific symptoms such as dyspepsia, weight loss, and anemia, making its early detection and diagnosis difficult. Therefore, when the disease is diagnosed it is usually advanced, and treatments become more complex and costly. 10 The results of a study showed that the burden of gastric cancer and the number of disability-adjusted life-years in the province of Kohgiluyeh and Boyer Ahmad in 2015 was 754.03 years, indicating a high burden of disease. 11 On the other hand, cancer, especially gastric cancer, in addition to their high burden of disease which leads to a reduction in production and productivity in the economy, imposes heavy costs on households and the health system. These costs are also very important from the societal perspective and account for 5% to 10% of the total health-care costs in most developed countries. 12 Among various cancers, gastric cancer imposes a huge economic burden on the affected person and the health-care system. Gastric cancer is considered as a serious illness in terms of control and treatment, and its medical costs are almost 10 times higher than other noncancerous diseases. Also, the medical costs of patients with advanced gastric cancer are higher than those of patients with gastric cancer whose stage of the disease is unclear. 13
Only a few studies have been conducted on the economic burden of gastric cancer, such as studies conducted by Haga et al 14 in Japan and Kim et al 15 in South Korea, which have reported its economic burden at $US11 billion and $US2.8 billion, respectively. Moreover, Mariotto et al 16 in their study have estimated the direct costs of gastric cancer in the United States at $US1.82 billion. Also, Khorasani et al in their study have reported the total cost of productivity loss caused by premature deaths due to gastric cancer in Iran in 2012 as US$209 920 163, 17 and Karami-Matin et al in their study have reported that in Iran during 2006 to 2010, the costs increased from US$45 850 250 in 2006 to $US51 273 537 in 2010. 6
Despite the high prevalence of gastric cancer in Iran, there are no comprehensive studies investigating the economic burden of this disease. Therefore, faced with increasing numbers of gastric cancer in Kohgiluyeh and Boyer Ahmad province in Iran, we conducted a study to determine the economic burden of gastric cancer in this province in 2016.
Materials and Methods
This was a cross-sectional cost of illness study conducted to determine the economic burden of gastric cancer in Kohgiluyeh and Boyer Ahmad province in Iran in 2016. Kohgiluyeh and Boyer Ahmad is 1 of the 31 provinces of Iran located in the southwest of the country and its capital is Yasuj. In general, there are 2 approaches for calculating the economic burden of diseases, including incidence-based and prevalence-based approaches. 18 In the present study, the prevalence-based approach was used, and the economic burden of gastric cancer was estimated from the patients’ perspective. In the prevalence-based approach, the costs of a disease associated with a time period (often 1 year) due to the prevalence during the same period, irrespective of the onset time of the disease, are estimated. 18 Therefore, in this study, the costs of all patients with gastric cancer, including patients whose illness started in 2016 or before, was calculated for 2016. The study population consisted of all patients with a definitive diagnosis of gastric cancer in Kohgiluyeh and Boyer Ahmad province registered in the Iran Cancer Registration System affiliated to the Health Deputy of Yasuj University of Medical Sciences in 2016. Of 155 patients registered in this system, 45 patients were excluded from the study due to missing key data, and the rest were studied using census method. Inclusion criteria were patients diagnosed with gastric cancer based on the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (C16) in 2016 in Kohgiluyeh and Boyer Ahmad province and the patients and their families’ willingness to participate in the study. Exclusion criteria included patients and their families’ unwillingness to participate in the study, incomplete patients’ medical records, and having other diseases and cancers as comorbidities. The present study was approved by the ethics committee of Shiraz University of Medical Sciences (Project No. 95-01-07-11299). Informed consent was obtained from all patients participating in the study.
In this study, the required data were collected using a data collection form consisting of 2 parts. The first part was related to patients’ demographic characteristics, and the second part was included items related to the costs. Costs were divided into 2 main categories: direct and indirect costs. Direct costs were divided into medical and nonmedical costs. Direct medical costs included costs related to physicians and oncologists’ visits, emergency department visits, chemotherapy, surgical services, laboratory tests, ultrasonography, magnetic resonance imaging, computed tomography scan, radiology, radiotherapy, endoscopy, colonoscopy, transfer by ambulance, patient hospitalization, and medications used by patients. These costs were calculated using the patients’ medical records available in the Health Deputy of Yasuj University of Medical Sciences and hospitals to which patients were admitted in 2016 as well as tariffs of diagnostic and therapeutic services approved by the Ministry of Health and Medical Education in 2016 available in the Treatment Deputy of Yasuj University of Medical Sciences. Direct nonmedical costs included the costs of transportation, accommodation, meals for the patient and relatives, patient consumables, and the costs of accommodation for people who visit the patient at his or her home, which were calculated by asking patients and their families. Indirect costs were calculated from productivity losses of patients and their families due to absence from work and daily activities caused by illness or patient care, calculated using the human capital approach. 19 For collecting and calculating the required data on indirect costs, 2 methods were used simultaneously because of the need to obtain 1-year-old data from the studied patients and in order to minimize the possible recall bias. First, indirect costs were calculated using data obtained directly from the patients and their families. Second, indirect costs were calculated by the researchers based on the patients and their relatives’ employment status, the patients’ physical condition, the minimum wage determined by the Ministry of Labor and Social Welfare, and the amount of income lost by the patients’ relatives. Finally, the mean of these 2 numbers, obtained directly from the patients and their families and from other sources by researchers, was considered as indirect costs. In order to make international comparisons, all costs were converted into the US dollar using the exchange rate of each US dollar equaling to 30 221 Rials in 2016. 20 The collected data were analyzed using Excel 2013.
Results
The results showed that most of the studied patients were male (77%), in the age-group of 55 to 65 years (39%), married (99%), illiterate or with elementary education level (77%), had rural health insurance coverage (48%) and no supplementary insurance coverage (81%), had monthly income between US$193.53 and 303.89 (43%), and had malignant tumors (60%; Table 1).
Demographic Characteristics of the Studied Patients.

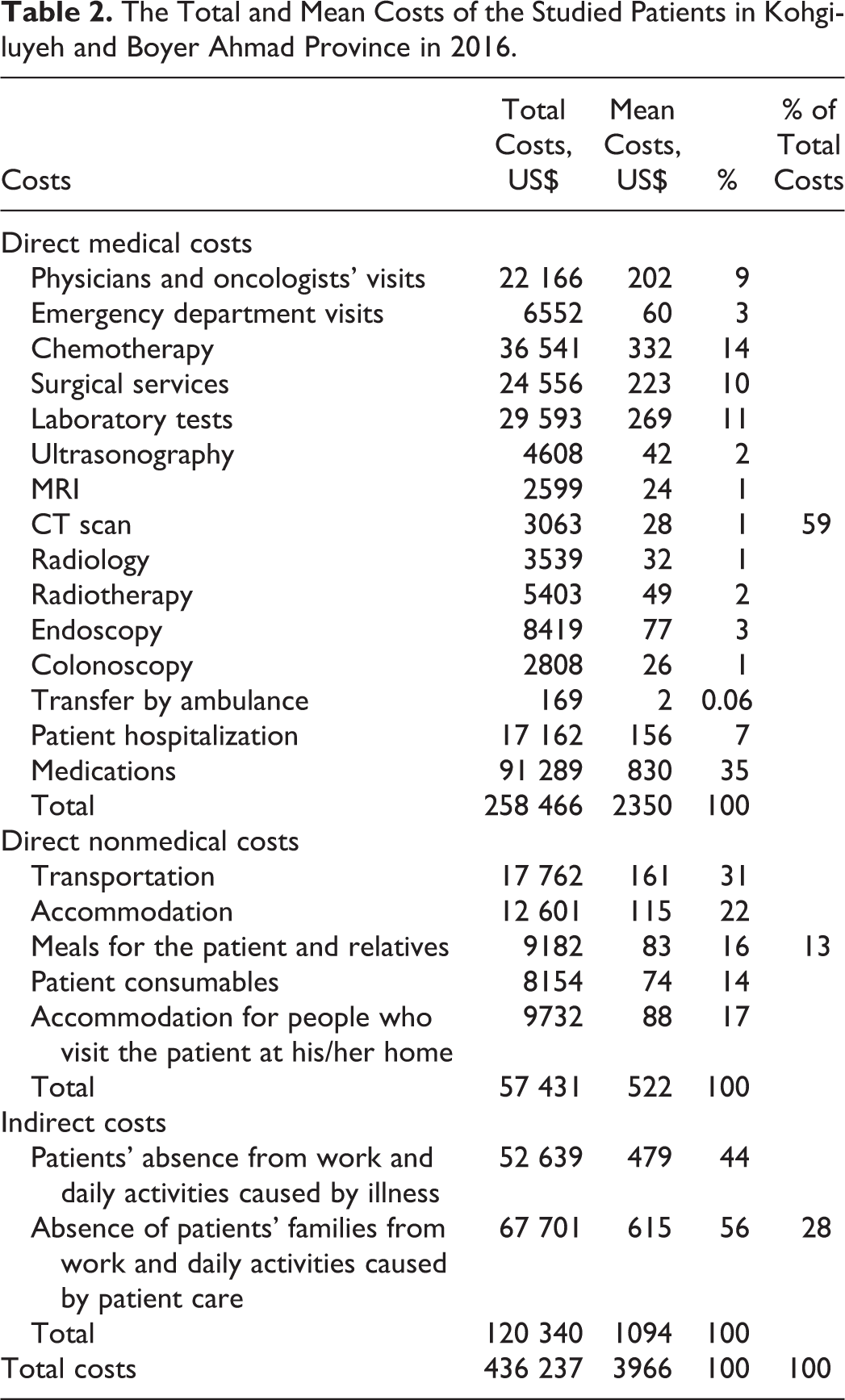
Furthermore, the results showed that the total costs of gastric cancer in Kohgiluyeh and Boyer Ahmad province in 2016 were US$436 237, in which the direct medical costs were 59%, indirect costs were 28%, and direct nonmedical costs were 13% of total costs. Mean costs per patient were US$3966. The total and mean direct medical costs in 2016 were US$258 466 and US$2350, respectively, in which the major costs were related to the costs of medications used (35.32% of total direct medical costs), chemotherapy (14% of total direct medical costs), and laboratory tests (11% of total direct medical costs), respectively. Moreover, the total and mean direct nonmedical costs in 2016 were US$57 431 and US$522, respectively, in which the major costs were related to the costs of transportation (31% of total direct nonmedical costs), accommodation (22% of total direct nonmedical costs), and accommodation for people who visit the patient at his or her home (17% of total direct nonmedical costs). Also, the total and mean indirect costs in 2016 were US$120 340 and US$2, in which the major costs were related to the absence of patients’ families from work and daily activities caused by patient care (56% of total indirect costs; Table 2).
The Total and Mean Costs of the Studied Patients in Kohgiluyeh and Boyer Ahmad Province in 2016.
Discussion
This study was conducted to determine the economic burden of gastric cancer in Kohgiluyeh and Boyer Ahmad province of Iran in 2016. The results showed that most of the studied patients with gastric cancer diagnosis were male, in the age-group of 55 to 65 years, married, illiterate or with elementary education level, had rural health insurance coverage and no supplementary insurance coverage, and had monthly income between US$199 and US$331, consistent with studies from other countries. 21 -24 Based on the results of the present study, the total costs and economic burden of gastric cancer in Kohgiluyeh and Boyer Ahmad province of Iran in 2016 were estimated to be US$436 237, in which the highest were related to the direct medical costs indicating that the decreases in the direct medical costs for patients with gastric cancer could significantly reduce the economic burden of gastric cancer in Kohgiluyeh and Boyer Ahmad. Kim et al 15 in their study found that the economic burden of gastric cancer in South Korea was estimated to be US$2.8 billion, in which the lowest costs were related to the direct nonmedical costs. Hong et al 4 in their study estimated the economic burden of advanced gastric cancer in Taiwan at US$423 million, the lowest of which were related to direct nonmedical costs. The results of these 2 studies are in line with those of the current study. In the studies conducted by Kim et al and Hong et al, the highest costs were related to indirect costs, which are not consistent with the results of the present study. It should be noted that the great difference in the economic burden of gastric cancer between the present study and the Hong et al’s and Kim et al’s studies can be due to the estimation of gastric cancer only in 1 of the provinces of Iran in the present study, while in 2 other studies the burden of gastric cancer had been calculated in the whole country of Taiwan and South Korea. On the other hand, in the study of Hong et al, the burden of advanced gastric cancer had been estimated which had led to higher costs and economic burden because the studied patients were in the advanced stages of gastric cancer, and they needed more diagnostic and therapeutic measures. Undoubtedly, early diagnosis of the disease and effective treatment can significantly reduce the economic burden imposed on the patients with gastric cancer as well as the society. Also, the results of the present study showed that the total and mean direct medical costs in Kohgiluyeh and Boyer Ahmad province in 2016 were US$258 466 and US$2350, respectively, in which the highest and lowest direct medical cost was related, respectively, to the medications used by patients and transfer by ambulance. The reasons for the high costs of medications used by the studied patients were that such medications are very expensive and some of them are not covered by the health insurance organizations. On the other hand, the reason for the low costs of transferring by ambulance is that there is usually no urgent and immediate transfer of patients with gastric cancer to medical centers, and basically their required services, such as chemotherapy, laboratory tests, ultrasonography, and so on, are provided as elective services and according to a specific and determined schedule and timetable. In the study of Izadi et al, the medication costs accounted for the largest share of direct medical costs for patients with gastric cancer in Kerman, 25 which are consistent with those of the present study. Furthermore, the results represented that the total and mean direct nonmedical costs in Kohgiluyeh and Boyer Ahmad province in 2016 were estimated to be US$57 431 and US$522, respectively, in which the highest and lowest direct nonmedical costs were related to the costs of transportation and patient consumables, respectively. The shortage of public transportation vehicles needed for patients’ transportation in the town as well as for going to the capital city to receive the required services and medical treatments and more use of passenger cars and vehicles with higher costs can be a reason for high costs of transportation. Considering that consumables are often used for elderly patients and patients who have entered the final stages of the disease, and given that a small number of patients in the present study had this feature, the cost of patient consumables was the lowest cost among the direct nonmedical costs. In the study of Bazyar et al, 26 patients coming from distant areas to the specialized hospitals and medical centers in big cities for receiving medical services were faced with higher costs, which is in line with the results of the current study. The results showed that the total and mean indirect costs in the studied province in 2016 were US$120 340 and US$1094, respectively, in which the highest costs were related to the absence of patients’ families from work and daily activities caused by patient care. This is because most of the studied patients were elderly and in the age-group of 55 to 65 and needed to be accompanied by at least 1 of their family members at the time of going to the medical centers for receiving required services and treatment, and if they had other disabilities, including motor disabilities, the number of family members for accompanying them would increase. This had caused more and longer absence of patients’ families from work and daily activities, and therefore, its costs were the highest ones. This study had a series of limitations, including conducting a cross-sectional study as well as the defects in some of the patients’ medical records.
Conclusion
Based on the results of the present study, the total costs and economic burden of gastric cancer in Kohgiluyeh and Boyer Ahmad province of Iran in 2016 was US$436 237, in which the highest costs were, respectively, related to the direct medical costs (the costs of medications used by patients), indirect costs (absence of patients’ families from work and daily activities caused by patient care), and direct nonmedical costs (the costs of transportation). Given the high out-of-pocket costs of medications used patients with gastric cancer, health insurance coverage and government subsidies for purchasing the necessary medications by these patients should be increased. Also, it is recommended that the required specialized care and services related to gastric cancer should be provided in provincial cities as well as capital cities so that patients do not have to go to the capital cities to receive such services, and this will greatly decrease the direct nonmedical costs, including the costs of accommodation and transportation. Moreover, if there is a possibility of performing laboratory tests for Helicobacter pylori (the most important cause of gastric cancer) in all patients with gastrointestinal diseases such as gastric ulcer, gastritis, and so on by the Ministry of Health and Medical Education subsidies or medical insurance organizations, if it is cost-effective, and treating patients with positive test result, the incidence of gastric cancer will significantly decrease in Kohgiluyeh and Boyer Ahmad province. Providing training courses on the prevention of gastric cancer at an early age and before the onset of the disease and sharing required information on the disease during these training courses or in the mass media can help to raise public awareness about the ways of preventing gastric cancer.
Footnotes
Authors’ Note
The present article was extracted from the thesis written by Abed Eghdami supported by Shiraz University of Medical Sciences Project No. 95-01-07-11299. This project also was supported financially by the Social Determinants of Health Research Center and Center for Diseases Report of Yasuj University of Medical Sciences.
Acknowledgments
The researchers would like to thank the studied patients for their kind cooperation with the researchers in collecting and analyzing data, as well as the Social Determinants of Health Research Center and Center for Diseases Report of Yasuj University of Medical Sciences for their assistance in conducting the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.