
Abstract
Pediatric solid tumors are heterogeneous and comprise various histological subtypes. TP53, a tumor suppressor, orchestrates the transcriptional activation of anti-cancer genes. The gene coding for this protein is highly polymorphic, and its mutations are associated with cancer development. The Arg72Pro polymorphism in TP53 has been associated with susceptibility to various types of cancer. Here, in this hospital-based study, we evaluated the association of this polymorphism with susceptibility toward malignant abdominal solid tumors in children in the Hunan province of China. We enrolled 162 patients with neuroblastoma, 60 patients with Wilms’ tumor, and 28 patients with hepatoblastoma as well as 270 controls. Genotypes were determined using a TaqMan assay, and the strength of the association was assessed using an odds ratio, within a 95% confidence interval identified using logistic regression models. Our results showed that the Arg72Pro polymorphism did not exhibit significant association with susceptibility toward pediatric malignant abdominal solid tumors. Stratification analysis revealed that this polymorphism exerts weak sex- and age-specific effects on Wilms’ tumor and hepatoblastoma susceptibility, respectively. Overall, our results indicate that the Arg72Pro polymorphism may have a marginal effect on susceptibility toward pediatric malignant abdominal solid tumors in Hunan, and this finding warrants further confirmation.
Introduction
Malignant tumors are detrimental to people’s lives and health. In recent years, pediatric cancers have emerged as the leading cause of disease-related morbidity and mortality in children, second only to accidents in developed countries. 1 In contrast to most adult cancers—the majority of which are of epithelial origin and usually develop over time due to cancer risk factor exposure—most pediatric solid tumors are considered to have an embryonic or developmental origin as alterations in organogenesis or normal growth can result in the generation of these tumors from any of the 3 germ cell lineages. 2,3 Given the advances in multimodal therapy for pediatric oncology patients, cure rates or the 5-year survival rates for pediatric cancers have increased to approximately 80% in recent decades. 4,5 However, the prognosis of many pediatric high-risk solid tumors remains poor. 6
Pediatric solid tumors are typically heterogeneous and are characterized by occult onset, high malignancy, and complex and diverse clinical manifestations. Most malignant abdominal solid tumors are found in children aged 1 to 5 years, with neuroblastoma being the most common, followed by Wilms’ tumor, hepatoblastoma and rhabdomyosarcoma. 7 Neuroblastoma is the most common malignant tumor in infancy and the most prevalent extracranial solid malignancy in childhood. 8 Neuroblastoma mainly originates from neural crest progenitor cells in the sympathetic nervous system and primarily occurs in the adrenal gland, followed by the mediastinum, neck, lower extremities, and other nerve tissues. 9,10 The prognosis of neuroblastoma patients varies greatly from spontaneous regression without treatment to rapid malignant progression—in spite of aggressive multimodal therapy. 11 Wilms’ tumor, usually derived from the embryonal nephric mesenchyme, is the fourth most frequently diagnosed pediatric malignant tumor worldwide and account for 7%-8% of the tumors in childhood. 12 This tumor is widely believed to arise as a result of erratic and disordered kidney development, in which posterior renal blastocysts fail to differentiate into glomeruli and renal tubules. 13 Hepatoblastoma, a typical embryonic tumor, accounts for nearly 80% of the pediatric liver malignancies and 1% of all childhood tumors. 14,15 Given that the exact etiology and mechanisms underlying the development of these malignant abdominal solid tumors remain unknown, elucidation of the pathogenesis and identification of more susceptible genes is imperative.
Growing evidence from genome-wide association studies (GWASs) has highlighted the importance of germline variations in disease susceptibility. As a result, considerable advances have been made in our understanding of the genetic underpinnings of pediatric malignant solid tumors. TP53, a well-known tumor suppressor gene located on chromosome 17p13.1, comprise 11 exons and 10 introns. 16 This gene encodes a 393 amino-acid–long protein that is critical for regulating the cell cycle and executing tumor suppressing functions by orchestrating of the transcriptional activation of tumor-associated genes involved in apoptosis, maintenance of genetic stability, and angiogenesis. 17 -19 Alterations in this gene have been extensively studied in a variety of human malignancies, including pediatric malignant solid tumors. 20 The fact that the Single Nucleotide Polymorphism Database hosts information regarding >1000 TP53 single nucleotide polymorphisms (SNPs) supports the highly polymorphic nature of this gene. 21 Among those polymorphisms, Arg72Pro (rs1042522 C>G) in exon 4 is the most important and extensively investigated. 22 Genetic variations may alter the expression levels and structures of the tumor suppressor genes, consequently affecting their tumor suppressive function. In addition, TP53 genotyping is considered a useful inexpensive tool for predicting the risk of developing cancers, such as lung cancer, thereby contributing to earlier detection and management of the disease. 23 However, few studies have explored the association between this polymorphism and susceptibility to simultaneously acquiring more than 2 pediatric malignant solid tumors risk simultaneously. The main objective of the present study was to investigate the association between the Arg72Pro polymorphism and the comprehensive risk of developing 3 malignant abdominal solid tumors, i.e. neuroblastoma, Wilms’ tumor, and hepatoblastoma.
Materials and Methods
Study Subjects
This case-control study was approved by the Institutional Review Board of Hunan Children’s Hospital, Changsha, China (IRB number: HCHLL-2020-80), and informed consent was obtained from the guardians of all participants. All patients at our hospital who were histopathologically diagnosed with neuroblastoma, Wilms’ tumor, or hepatoblastoma were included in this study. Importantly, all patients were younger than 18 years of age, and none of them had a history of any other tumors. Information regarding the major clinical characteristics of the patients, including age, sex, tumor sites, and tumor stage, was collected. In total, 250 patients with abdominal solid tumor and 270 controls were separately recruited from Hunan Children’s Hospital. The abdominal solid tumor patients comprised those with neuroblastoma (n = 162), Wilms’ tumor (n = 60), and hepatoblastoma (n = 28). The healthy controls were randomly chosen among age- and sex-matched children living in the same area as the abdominal solid tumor patients, with match age and sex. The demographic and clinical characteristics of all participants are provided in Supplemental Table 1.
SNP Selection and Genotyping
Based on previous publications, the Arg72Pro polymorphism of TP53 gene was chosen for this study. 24,25 Genomic DNA was isolated from venous blood samples using a TIANamp Blood DNA Kit (TianGen Biotech Co. Ltd., Beijing, China). The TaqMan SNP Genotyping Assay from Applied Biosystems (Foster City, CA, USA) was used for genotyping TP53 rs1042522 C>G. 26 -28 For quality control, negative controls (with water) and duplicate test samples (10% of all the samples) were included in each 384-well plate.
Statistical Analysis
The chi-square test was performed to test for deviations from the Hardy-Weinberg equilibrium in the genotype frequencies of the polymorphism in control participants along with differences in demographic variables between the case and control subjects. The association between the Arg72Pro polymorphism of TP53 gene and pediatric malignant abdominal solid tumor risk was determined as an odds ratio (OR) within a 95% confidence interval (CI) based on multivariate logistic regression analyses. All statistical analyses were performed using SAS release 9.1 software (SAS Institute, Cary, NC, USA). Statistical significance was set at P < 0.05.
Results
Patient Characteristics
This study included 250 patients with pediatric solid abdominal tumors and 270 cancer-free controls. The overall clinical characteristics of all participants are presented in Supplemental Table 1. For patients with neuroblastoma or Wilms’ tumor, no significant difference in age (P = 0.322 and P = 0.872, respectively), or sex (P = 0.842 and P = 0.697, respectively) was observed between the patients and controls. However, for hepatoblastoma, a significant difference in age (P = 0.018) but not sex (P = 0.620) was observed between the patients and controls. On employing the International Neuroblastoma Staging System criteria, 48 (29.63%), 22 (13.58%), 54 (33.33%), 37 (22.84%), and only 1 (0.62) neuroblastoma samples were classified the diseases into stages I, II, III, V, and 4 S neuroblastomas, respectively. Upon employing the National Wilms’ Tumor Study-5 criteria, 14 (23.33%), 16 (26.67%), 21 (35.00%), and 9 (15.00%) patients were defined as having clinical stage I, II, III, and IV Wilms’ tumor, respectively. In case of hepatoblastoma, most of the patients had stage III disease (46.43%), followed by stage II (28.57%), stage IV (17.86%), and stage I (7.14%).
Association Between the Arg72Pro Polymorphism and Pediatric Abdominal Solid Tumor Risk
We successfully genotyped the 250 samples and 270 controls. The genotype frequencies of the Arg72Pro polymorphism and its associations with pediatric abdominal solid tumor susceptibility are summarized in Table 1. The genotype frequency distribution of the polymorphisms was as follows: 1) 37.65% (CC), 41.36% (CG), and 20.99% (GG) in the patients with neuroblastoma; 2) 38.33% (CC), 33.33% (CG), and 28.33% (GG) in the patients with Wilms’ tumor; 3) 32.14% (CC), 42.86% (CG), and 25.00% (GG) in the patients with hepatoblastoma; and 4) 38.89% (CC), 42.96% (CG), and 18.15% (GG) in the controls. No significant associations were identified between Arg72Pro polymorphism and pediatric solid abdominal tumor risk, even after adjusting for age and sex.
TP53 Gene Arg72Pro Polymorphism and 3 Pediatric Solid Abdominal Tumors Susceptibility.
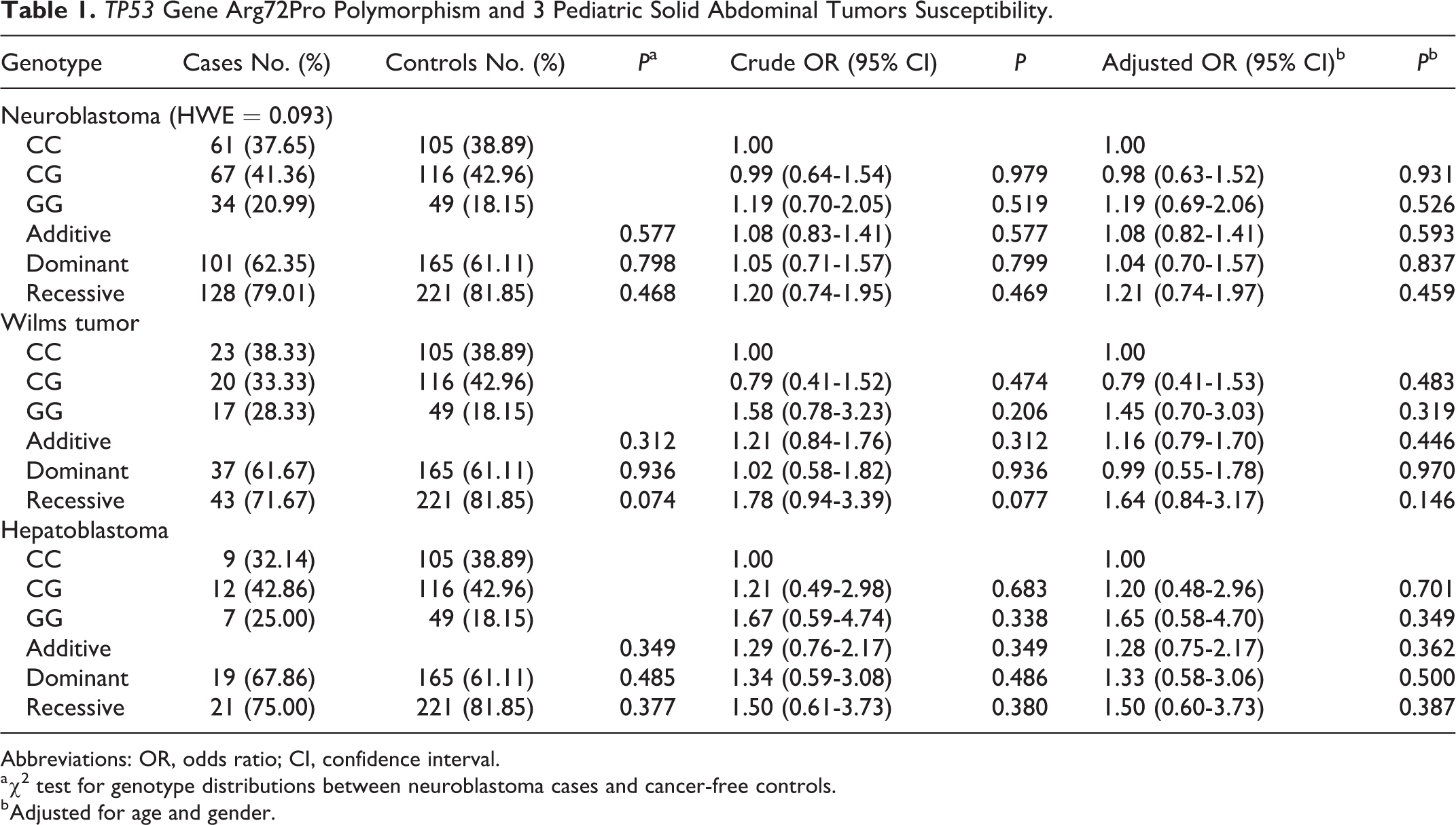
Abbreviations: OR, odds ratio; CI, confidence interval.
a χ2 test for genotype distributions between neuroblastoma cases and cancer-free controls.
b Adjusted for age and gender.
Stratification Analysis
Due to the heterogeneity of pediatric solid tumors, we further conducted a stratification analysis to investigate the association between the Arg72Pro polymorphism and pediatric abdominal solid tumor susceptibility for different subtypes. As shown in Table 2, we were unable to identify any prominent associations between the polymorphism and neuroblastoma susceptibility in all strata in both single and combined analyses. However, compared to the carriers of the CC and CG genotypes, male rs1042522 GG genotype carriers were associated with a decreased risk of developing Wilms’ tumor (adjusted OR = 2.38, 95% CI = 1.01-5.58, P = 0.047). We also observed a significant protective association between the rs1042522 GG genotype and hepatoblastoma risk in children aged 18 months or younger (adjusted OR = 3.35, 95% CI = 1.004-11.15, P = 0.049). No other significant associations were identified.
Stratify Results for TP53 Gene Arg72Pro Polymorphism and 3 Pediatric Solid Abdominal Tumors Susceptibility.

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
a Adjusted for age and gender, omitting the corresponding stratify factor.
b Clinical stage 4 s and sites of origin are just for neuroblastoma.
Values are in bold if the P < 0.05 or the 95% CI excluding 1.
Discussion
Genomic alterations across multiple childhood cancer types encourage scientists to value the genetic contribution of the host more than individual susceptibilities. Approximately half of all primary pediatric cancers harbor potentially targetable genetic events. 29 Numerous genetic polymorphisms are closely related to carcinogenesis. 30 -32 To date, the association between SNPs and susceptibility to malignant solid tumors in childhood remains poorly understood. Investigating additional polymorphisms is instrumental in furthering our understanding of genetic variations and their associations with susceptibility toward pediatric solid tumor.
TP53, one of the most well-known cancer-causing genes, encodes a 53 kDa transcription factor (p53), which plays a role in several important processes, such as cell cycle control, apoptosis, induction of metabolic changes, and genome function stability. 33,34 For a long time, p53 was considered the guardian of human cells against cancer because of its tumor suppressor function, as evidenced by the high inactivation rate of p53 in human tumors. 35,36 This role is highly dependent on the integrity of its structure and function, with certain mutations resulting in the production of a dysfunctional protein with altered functions, that aids tumorigenesis. Unfortunately, mutations in TP53 are common and have a causal relationship with a variety of cancer types. 37,38 Most of these mutations are SNPs that lead to the production of dysfunctional p53 proteins, some of which develop carcinogenic properties. 39,40
Interestingly, the 2 polymorphic alleles of TP53 exhibit different biological functions based on properties, such as the capacity to induce target gene transcription, induction of cell cycle arrest, and susceptibility to degradation by the E6 protein, all of which consequentially alter the cancer susceptibility. 24,30 Specifically, TP53 with the wild-type codon 72 shows relatively stronger tumor suppressor activity.
Numerous studies have explored cancer susceptibility in relation to the Arg72Pro polymorphism. 40 Rosenthal et al first identified that this polymorphism dramatically affected the risk of developing cervical cancer in British women; in particular, women carrying homozygous TP53 Arg variants were inclined be at an enhanced risk of developing cervical cancer. 41 Subsequently, on performing a meta-analysis on data from 7,946 patients and 7,888 controls, Klug et al found that there was no remarkable association between the Arg72Pro polymorphism and cervical cancer risk. 42 Another meta-analysis involving a series of malignant solid tumors (e.g., breast and endometrial cancer) revealed that the association with this polymorphism was eliminated when tumor tissue was replaced by other sources as the genotyping material. 24 Additionally, this polymorphism is associated with bladder cancer risk among Asians but not Caucasians. 43 Although several studies have identified an association between solid tumors and the Arg72Pro polymorphism, the results remain inconclusive due to the limited sample size, differences in the source of genotyping material, and allele frequency differences between ethnic groups.
This polymorphism has also been well-studied in several types of childhood malignant abdominal solid tumors. Cattelani et al found that the Arg72Pro polymorphism had no effect on the risk of developing neuroblastoma by genotyping 286 patients and 288 controls. 44 This polymorphism was subsequently found to be associated with the risk of developing neuroblastoma and Wilms’ tumor but not hepatoblastoma among Chinese children. 19,21,34 However, there remains a lack of valuable evidence depicting the association between the polymorphism and the integrated risk of pediatric malignant abdominal solid tumors. To the best of our knowledge, only one study has investigated this particular association by genotyping 101 pediatric solid tumors samples and 202 controls; Borbora et al identified an SNP pair composing of TP53 rs1042522 and p21cip1 rs1059234 that had a significant impact on the risk of developing pediatric solid tumors. 45 However, the relatively small sample size undermined these findings. In the present case-control study, 250 patients with malignant abdominal solid tumors and 270 controls were genotyped. Even though the overall results indicated no significant association between this polymorphism and the comprehensive risk of abdominal malignant solid tumors among children in the Hunan province, this polymorphism was found to exert weak sex- and age-specific effect on the risk of developing Wilms’ tumor and hepatoblastoma. In contrast with existing studies, we pioneeringly performed gene association susceptibility analyses of several common abdominal malignant solid tumors in childhood simultaneously. This protocol helped to elaborate the influence of TP53 and Arg72Pro polymorphism on abdominal malignant solid tumors.
It is important to note that pediatric malignant abdominal solid tumors are heterogeneous and multi-factorial. Therefore, several limitations accompany our study. First, we only focused on the genetic factors, neglecting the environmental and genetic-environmental factors. Second, our sample size was not large enough, and we restricted the cancer types to neuroblastoma, Wilms’ tumor, and hepatoblastoma. Third, in addition to tumor tissue, other tissues should also be used as genotyping material for patients in order to reduce and eliminate significant bias in estimating the genetic effects in cancer association studies. Fourth, tumorigenesis involves variation in the expression of multiple genes, and the effect of individual gene on overall susceptibility is weak. Thus, other known polymorphisms should also be investigated, alone or in combination in the future.
Conclusion
This study demonstrated that the Arg72Pro polymorphism of TP53 gene may exert marginal effects on the susceptibility to pediatric malignant abdominal solid tumors in children in the Hunan province of China. Further molecular studies are warranted to confirm our findings.
Supplemental Material
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211004880 - Association Between Arg72Pro Polymorphism in TP53 and Malignant Abdominal Solid Tumor Risk in Hunan Children
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211004880 for Association Between Arg72Pro Polymorphism in TP53 and Malignant Abdominal Solid Tumor Risk in Hunan Children by Zan Liu, Zhenghui Xiao, Ming Li, Yaling Xiao, Xiyang Wang, Jing He and Yong Li in Cancer Control
Footnotes
Authors’ Note
The study was approved by the Institutional Review Board of Hunan Children’s Hospital, and the informed consent was obtained from all guardians of participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Natural Science Foundation Project of Hunan Province (No: 2018JJ2210) and Hunan Provincial Key Laboratory of Pediatric Emergency Medicine (No: 2018TP1028).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.