
Abstract
Keywords
Introduction
In the US, Hispanic women have the highest incidence of cervical cancer and are 70% more likely to die from it than non-Hispanic White women. 1 Cervical cancer mortality rates are higher for Hispanic women on the US-Mexico border compared to non-border areas. 2 The primary causal factor for development of cervical cancer is persistent infection with a high-risk or oncogenic type of human papillomavirus (HPV). 3 The factors affecting HPV infection persistence are not well understood. There are more than 200 genotypes of HPV identified of which about 40 affect the genital tissues and these are divided into high-risk or low risk types based on their risk of carcinogenesis. The high-risk genotypes (HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68) cause cervical cancer (squamous cell carcinoma or adenocarcinoma) while other genotypes cause genital warts. About 70% of cervical cancer cases worldwide are associated with HPV 16 and 18. 4
Vaccines to prevent HPV-associated cancers have been developed as a preventive strategy. The bivalent vaccine became available in 2006 and since then new quadrivalent and 9-valent HPV vaccines have become available for preventing HPV. Since 2018 only the nonavalent vaccine has been available in the USA, it provides coverage for 2 low risk types (6 and 11) and 7 high risk types (16, 18, 31, 33, 45, 52, and 58). 5 Current HPV vaccine recommendations state that HPV vaccine should be given routinely to all males and females at 11 or 12 years of age. National HPV vaccination completion rates among adolescents are suboptimal at about 51.1% 6 and fall far short of the Healthy People 2020 target of 80%. 7 Uptake of the HPV vaccine among Hispanic adolescents is higher nationally at about 56%. 8
The effectiveness of this population-based preventive strategy not only depends on vaccine uptake but also on the relative prevalence of vaccine preventable genotypes in the community at risk. International and national data suggests that the HPV genotype distribution may vary by age, race/ethnicity or geography. 9,10 A better understanding of genotype prevalence among Hispanic women in the USA is needed, especially for those living on the US-Mexico border who suffer high cervical cancer health disparities. In this study, we investigated the distribution and prevalence of genital HPV genotypes in a population-based sample of Mexican American women living along the US-Mexico border. We believe that the findings of this study will help in understanding the HPV prevalence profile in this group of women and will help to inform future prevention efforts in the group with the highest cervical cancer incidence and mortality in the US.
Methods
Study Design
A cross-sectional study was conducted between 2015 and 2016 in order to characterize HPV subtypes. Women participating in a population-based cervical cancer screening program (De Casa en Casa) were approached for participation in the study when they attended for their Pap test. The De Casa program is a comprehensive screening program that provides no-cost screening, diagnostic testing and education to eligible women in a 2 county area (El Paso and Hudspeth County). These counties have a high proportion of Hispanic residents (78% and 81%). 11 Prior ethical approval for the study was obtained from the Texas Tech University Health Sciences Center, El Paso Institutional Review Board (IRB Protocol # E14129).
Eligibility
Eligibility criteria for entry into the program were age 21 to 65 years, due for cervical cancer screening (last Pap smear more than 3 years ago) uninsured, a self-reported Texas address, no history of cervical cancer, or hysterectomy, or unable to be enrolled in the Texas Department of State Health Services Breast and Cervical Cancer Services (BCCS) program (income greater than 200% of the federal poverty level or unable to provide proof of income). Individuals were enrolled from community sites including food pantries, community centers, fitness classes, and churches. Women were provided education and a Pap test appointment was made. Transportation was provided if needed.
Recruitment Procedure
Women were invited to be in the study when they attended their Pap test appointment at the designated Pap clinic at Texas Tech University Health Sciences Center El Paso (TTUHSC El Paso). Those expressing an interest were approached by study personnel who described the study and obtained written informed consent in a private room.
Specimen Collection and Processing
The Pap test samples were obtained and preserved in PreservCyt® liquid provided in the test kit, which allows for storage up to 6 weeks at 15 oC-30 oC. Following collection, Pap samples were sent to the lab to undergo routine clinical processing. Upon completion of the clinical testing, Pap samples were transferred to the research lab, de-identified and given a numerical tag and stored at at -20 o C. Tissue samples then were removed, defrosted and underwent DNA extraction using QIAmp DNA Mini Kit from QIAGEN®, a silica-membrane DNA binding method, according to the manufacture’s protocol. Following DNA extraction, the samples were genotyped using the Linear Assay from Roche® Diagnostics, a PCR-hybridization colorimetric method, according to the manufacture’s protocol. This LINEAR ARRAY® HPV genotyping test identified single and multiple infections from 37 various HPV types including 14 high-risk types
Sample size and Statistical Analysis
Assuming a 10% prevalence of high-risk HPV, a total of 554 participants were required to produce a 2-sided 95% confidence interval (CI) using asymptotic normal distribution with a width equal to 5%. Thus, this study aimed to recruit 600 participants. Descriptive statistics were used to summarize the study sample characteristics. The prevalence of HPV infection and high-risk HPV type was estimated using binomial proportion and reported along with the 95% confidence interval (CI). The distribution of each specific HPV type according to low and high-risk was also described. The subjects’ characteristics were compared by any HPV type or high-risk HPV type using either an unpaired t-test or Fisher’s exact test. The prevalence of any HPV type and high-risk HPV type and the 95% confidence intervals according to age-groups were plotted using a cluster bar diagram to demonstrate the age-pattern associated with HPV positivity. The 95% confidence interval (CI) for any HPV and HPV-high risk in each age-group was estimated using a binomial distribution. Data analyses were conducted using Stata 15 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
Data Statement
The data that support the findings of this study are available from the corresponding author, [NKS] upon reasonable request.
Results
Samples from 585 participants underwent the HPV genotyping test and 251 (43%) of these individuals provided consent for access to their screening medical record. With the exception of one individual, the entire cohort was Hispanic and all 251 women in the medical record sample were Hispanic. The distribution of sample characteristics are shown in Table 1. The average age of the subjects was 47 years old (range 22-65 years) and mean years in the US was 17 years (range 1-62 years). The majority of participants were Spanish speakers (93%), born in Mexico (90%), married (62%), had less than a high school education (70%), were unemployed (56%), and had low income (mean of $180 per month). Most women had a Pap smear 3 or more years ago (98%), had normal prior pap findings (98%), reported no prior history of HPV (99%), no regular doctor (95%), self-reported good to excellent health (67%), had heard about cervical cancer (88%), and had received a doctor recommendation for a Pap test (53%). These characteristics were not found to be different among subjects who were HPV positive versus those that were negative except for a slightly higher number of pregnancies in HPV negative subjects (p = 0.019).
Summary of Baseline Characteristics According to HPV Status in Subsample.

* All women in the sample were Hispanic.
Table 2 displays the prevalence of HPV infection and genotype distribution in this population. The population prevalence of HPV infection was 53.2% (n = 311, 95% CI: 49-57.3). The population prevalence of high-risk genotypes was 15.6% (95% CI:18.3%-25.1%). Among those who tested positive for HPV, 29.3% had a high-risk genotype. Overall there were 652 occurrences of a HPV genotype of which 169 (26%) were a high-risk genotype. Overall, 27.5% of women had a single strain HPV infection and a similar proportion (25.6%) had multiple strains of HPV infection. The mean number of genotypes among the women that tested positive was 2.1. Of cases with multiple infections, approximately 12% had 2 types of HPV followed by 3 types and 4 types; fourteen women had 6-8 types.
The Prevalence of Genital HPV Among Women (N = 585).

HPV: Human papillomavirus; CI: confidence interval
Figures 1 and 2 display the individual genotypes of HPV infection classified into high and low-risk types separately in our study population. The most common high-risk types were genotypes 35 (4.27%) 33 (3.76%) 16 and 39 (both 3.08%); there were only 2 occurrences of HPV genotype 18 (0.3%). We report type 52-33-35-58 (3.42%) because further typing required a second step that was not conducted. Overall 41% (69/169) of the high-risk genotype occurrences types were of a non-vaccine genotype (types 35, 39, 51, 56, 59, 68). The most common overall genotype was HPV 84 (40%), a low-risk genotype, other common low-risk genotypes were genotypes 82 followed 62, 67, and cp6108.
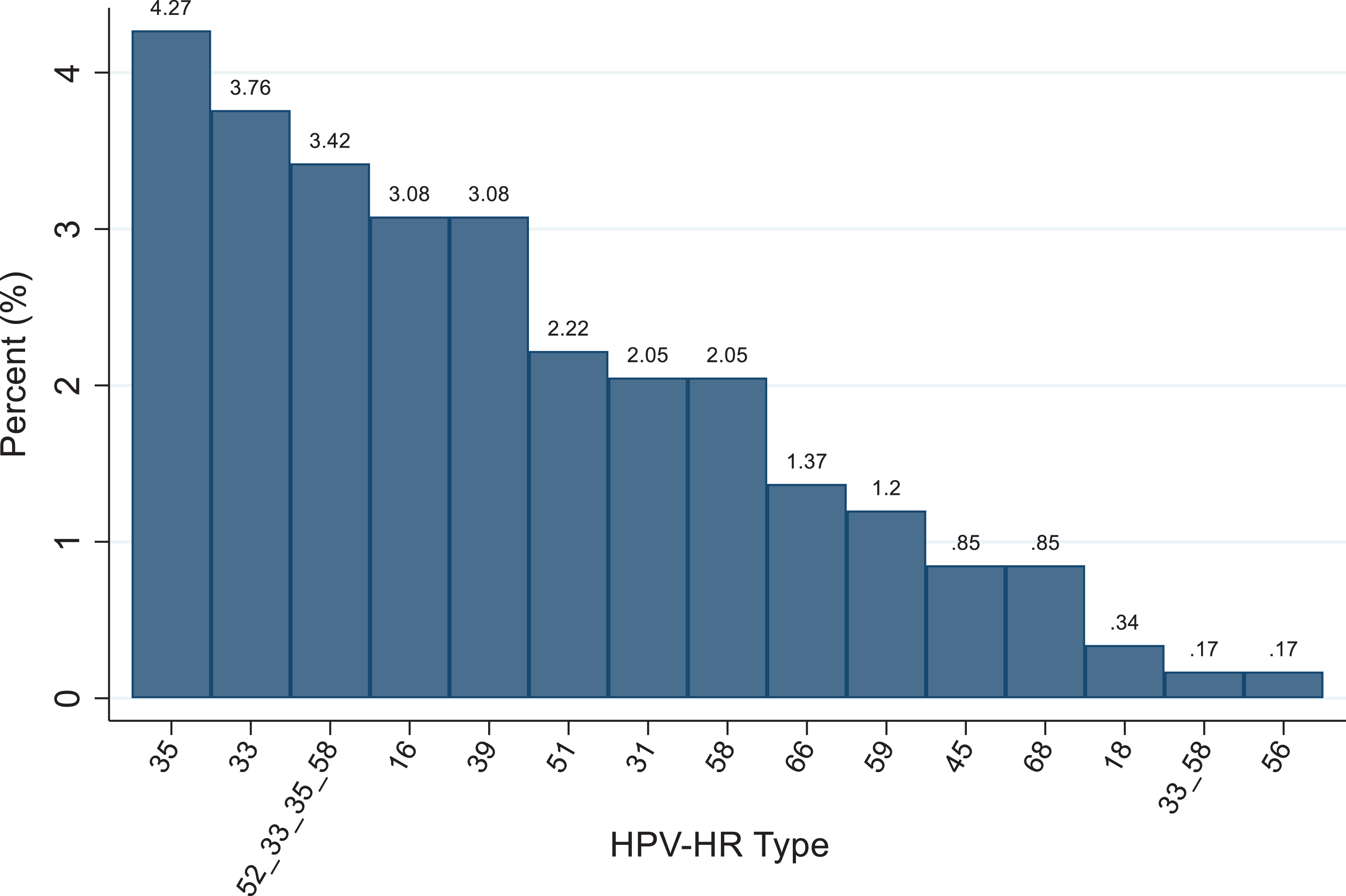
Prevalence and distribution of high risk HPV genotypes. HPV-HR: high-risk human papillomavirus.

Prevalence and distribution of low risk HPV genotypes. HPV-LR: low-risk human papillomavirus.
Figure 3 shows the prevalence of any HPV infection and HR HPV infection by age. Both demonstrated a U shape pattern with initial high rates that increase again starting around 45 years of age for any HPV and around the mid-fifties for high-risk HPV.

Distribution of HPV by age group. HPV-HR: High-risk human papillomavirus.
In the subsample consenting for medical record linkage (n = 251) all self-reported as Hispanic; we examined the association of demographic characteristics and cervical cancer risk factors among those with high-risk HPV vs those with no or low risk HPV genotypes. We observed that women who were younger, single, and reported better health were more likely to have high-risk HPV. Furthermore we noted that no woman aged 50 or above had type 16/18, whereas 4% (n = 10) had a non-16/18/ high-risk type. The results for the association of high-risk HPV and age at first intercourse and number of sex partners were in the expected direction but these associations were not significant. High-risk HPV was associated with age (p = 0.0007), being married/living with a partner (p < 0.001) and better health status (p = 0.04) (Table 3). In the adjusted analysis, only age (PR = 0.95, p = 0.005) and being married/living with a partner (PR = 0.28, p = 0.001) were associated with high-risk HPV.
Comparisons of Prevalence of High-Risk HPV and Low Risk HPV Compared to HPV Negative According to Baseline Characteristics in Subsample (n = 251).

SD: Standard deviation; IQR interquartile range; HPV: Human papillomavirus;
Discussion
This study is one of the few providing detailed information about the current HPV subtype prevalence in a general population of Hispanic women residing in the US. Our target population consisted of uninsured low income women living close to the US-Mexico border; a population that suffers a disparate burden of cervical cancer. We observed that the majority of women were vaccine naïve and 53.2% were positive for any HPV and 15.6% were positive for a high-risk HPV genotype. Our any HPV infection prevalence is a little higher than found in other population-based studies of women in the US 12 and higher than other studies including Hispanic women in the US: 37.9% among Hispanics in a national sample of sexually experienced females aged 14 to 59 12 and 26.8% in a Mexican born Federally Qualified Health Center in Chicago aged 30-60 years. 13 Our population prevalence of genital high-risk HPV among women (15.6%) is in the range observed by others in population-based or screening populations of Hispanics or Mexican Americans in the US (between 12.2% and 34.2%). 12 -15
Our findings are consistent with other studies that found racial/ethnic differences in HPV subtype prevalence in both low 12,14,15 and high risk populations in the US, 9,16 -18 The most common high-risk genotype we observed in our Hispanic population was HPV 35 (4.3%) followed by 33, 39, 16 and 52/33/35/58, (3-4%). We found only 2 other studies reporting a population-based high-risk HPV subtype prevalence among low risk Hispanic women in the US, one was conducted over 20 years ago 14 and the other only examined nonavalent HPV vaccine subtypes. In the former study, 14 specimens were collected between 1997 to 1998 among Mexican origin women along the border in the USA and specific high-risk HPV subtype prevalence was between 0.2% to 3.2% which compares to our observed range of between 0.17 and 4.3%. Although their observed prevalence of HPV 16 was similar to ours, we observed a greater frequency of non 16/18 high-risk HPV subtypes, especially 35, 33, and (52/33/35/58) subtypes. The most frequent oncogenic types in that study were 16 (3.2%) 39 (2.2%), 52 (2.0%) 58 (1.2%) 18 (1.1%) 56 (1.0%) and 31 (0.9%). The other study examined a national general population of US women and also found that a greater proportion of Hispanic women (as well as African American women) had a non-16/18 nonavalent vaccine high-risk HPV type (i.e. 31, 33, 45, 52, 58;): 23.6% among Hispanic women, versus 15.9% among non-Hispanic white women). 15 This pattern among Hispanic (and other minority) women is also supported by studies among high-risk women as well (i.e. those with abnormal paps, undergoing colposcopy, or with CIN 2+). 9,16 -18 They also observed that Hispanic (and/or Black women) have lower rates of HPV 16/18 and greater rates of non 16/18 types. 16,17 In particular, these studies report greater prevalence of types, 35, 58, 68, and 52.
These observed differences are of potential significance as many of these types are not included in the currently available nonavalent HPV vaccine. In fact, we observed that 41% of high-risk HPV occurrences were of a non-vaccine type and this is consistent with 2 other studies among high and low risk women that also concluded that a significant number of women, especially Hispanic and Black women have non-vaccine covered high-risk HPV types. 9,15
Our study was insufficiently powered to detect age-related differences in HPV prevalence, however, it does point to a possible U shaped age dependent prevalence for both any HPV and high-risk HPV with the age related decline in prevalence reversing at age 50-55 years. This uptick in older ages has been observed previously primarily in Central and South American populations 10 and has only been reported in one other US study among a Hispanic subgroup in a nationally representative sample. 12 We also observed an age-related high-risk HPV subtype pattern; with a decline in type 16/18 and an increase in non-16/18 high-risk HPV types which is consistent with the findings of others in both low and high-risk minority populations. 10,12,17,19 This may have implications for vaccine targeting and for clinical follow up, since data suggests that there is a longer development period for cancer associated with non-16/18 genotype cancers.
This study sheds light on the pattern and distribution of HPV genotypes among Mexican-origin Hispanic women residing in a region of the US with disproportionately high levels of cervical cancer incidence and mortality. Although the current strategy of HPV vaccination in the USA is expected to significantly reduce cervical cancer burden in all groups over time, there are some potential implications of our findings and those of others that should be considered. First, although the current vaccine targets 7 high risk types it does not include other prevalent types such as type 35 which appears to be observed at higher frequency among minority women this could potentially exacerbate differences in cervical cancer disease burden (due to greater prevalence of non-vaccine HR subtypes among minority women). Second, data suggests that although minority women and women of older ages are more likely to have have non 16/18 HR types, the cervical cancer screening management guidelines are predicated on presence or absence of only type 16/18. It may therefore be necessary to consider the presence or absence of more high risk types in the recommendations. Thirdly, the age-related uptick in HPV prevalence needs further attention, especially since studies suggest that older women have a greater prevalence of non-16/18 types. More work is needed to determine whether this is an effect specific to this cohort or is a phenomenon that reflects changes in sexual behavior in older age.
Strengths of our study include that a community-based sample of a large number of Hispanic women were examined and that detailed HPV subtype prevalence data was included. Second, we recruited a homogenous group consisting almost entirely oof Mexican-origin Hispanics therefore this information is generalizable to the largest Hispanic subpopulation in the US. The findings should be interpreted in the context of study limitations; first, the demographic and risk factor information could only be linked on a subsample providing consent; although we determined that those who were linked did not differ on key variables from those that were not linked. Second, the final step for typing was not performed on a subset of samples labeled 52-33-35-38, so the prevalence of those individual subtypes may be underestimated. Third, this study was cross-sectional and thus persistent infections cannot be distinguished from transient infections. Fourth, age related comparisons of HPV distribution were exploratory and underpowered so must be interpreted with caution. Finally, although participants were recruited after the licensure of the nonavalent HPV vaccine, this was a largely unvaccinated sample (mostly due to age) of uninsured women of low socio-economic status and findings must be interpreted in that context. Despite these limitations, we believe this study makes a valuable contribution to the literature on this topic.
In conclusion, we describe a detailed genital HPV genotype prevalence pattern in a general population of low income Hispanic (Mexican origin) women in the US that is known to suffer cervical cancer health disparities. We observed a different high-risk HPV subtype pattern and age distribution in this population, and this could have implications for future cervical cancer prevention efforts in the US.
Footnotes
Authors’ Note
Navkiran Shokar: conceptualization, data curation, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: N. K. Shokar; Cancer Prevention and Research Institute of Texas, Grant # PP130068 and Lizanell and Cuthbert Coldwell Foundation.