
Abstract
Background
Multi-cancer early detection tests (MCEDs) have the potential to identify over 50 types of cancer from a blood sample, possibly transforming cancer screening paradigms. Studies on the safety and effectiveness of MCEDs are underway, but there is a paucity of research exploring public views on MCEDs. We sought to explore public perspectives and understanding on the use of MCEDs in patient care.
Methods
We conducted a cross-sectional, qualitative study using one-on-one, semi-structured interviews. Residents of the United States aged 45–70 years old were recruited through a survey panel and purposively sampled to maximize racial diversity. Interviews explored understanding of MCEDs and perspectives on their use. Interviews were analyzed using thematic analysis with deductive coding and semi-quantification.
Results
Among 27 participants, mean age was 62 years (range 48-70) and most (63%) were non-white. Most participants had completed at least one cancer screening (89%). Participants had a positive impression of MCEDs (85%) and found the concept easy to understand (88%). They were enthusiastic about the convenience of MCEDs (30%) and thought they would improve “cancer outcomes” by looking for multiple cancers (70%) and facilitating early detection (33%). Participants emphasized the need to balance these benefits against potential harms, including inaccuracy (96%), cost (92%), test-related anxiety (56%), and lack of evidence of effectiveness (22%). Participants favored that MCEDs be delivered in primary care (93%). Participants worried that the potential benefits of MCEDs might not be equitably distributed (44%).
Conclusions
Members of the US public in this study expressed an interest in using MCEDs but had concerns regarding cost, accuracy, and potential inequitable access to the tests. Findings suggest that MCEDs that are found to be safe and effective will be acceptable to patients as a part of primary care, and underscore public interest in improving this technology.
Introduction
Multi-cancer early detection tests (MCEDs) are being developed to identify cancer at early stages and offer a potentially transformative approach to population-based cancer screening.1-3 MCEDs use liquid biopsy technologies and artificial intelligence/machine learning to look for a variety of genetic and molecular markers of malignancy. 4 Numerous MCEDs are in research and development, and these vary in features including the biomarkers used to identify cancers (eg, tumor cell-free DNA, proteins, tumor RNA, circulating tumor cells) and the number and types of cancers targeted for detection.5,6 Large-scale studies evaluating MCEDs by the National Cancer Institute, UK National Health Service, Centers for Medicare and Medicaid, and industry are underway, but will take several years to produce robust evidence of these tests’ accuracy.7-9
Even amidst a paucity of data supporting the use of MCEDs, tests are available to United States (US) patients with a prescription. 10 Members of the public are key stakeholders whose perspectives should be elicited to inform the development and evaluation of emerging technologies such as MCEDs. Engaging members of the public is crucial for designing technologies that address unmet needs through effective and user-friendly solutions.11,12 Members of the public can provide input on a variety of topics that inform the design and evaluation of novel technologies, ranging from identification of ideal product features to selection of appropriate outcome measures for their evaluation.13,14
Few studies have focused on public attitudes toward MCEDs. A recent scoping review of liquid biopsies identified only one study wherein patients were asked about their interest in using a test that looked for multiple cancers through a stool-based sample, finding general receptivity to its use.15,16 Two survey studies separately found that 70%-80% of participants would use an MCED if offered to them.17,18 At the same time, economic evaluation research has demonstrated that suboptimal outcomes from cancer screening programs like MCEDs, such as false positive findings and the need for additional diagnostic follow-up, create disutility for patients. 19 A focus-group study in the UK observed enthusiasm for MCEDs but indicated this was moderated by an individual’s beliefs about their cancer risk, personal preferences, and perceived integration into the UK’s National Health Services public health care system. 20 Research has yet to qualitatively explore the US general public’s perspectives on MCED test characteristics or to identify patient-centered pathways for their integration into routine care.
We sought to explore public perspectives and understanding of MCEDs and their role in clinical care. This information may be useful to diverse audiences including developers seeking to understand which factors related to MCEDs matter most to patients, as well as to clinical care providers considering how MCEDs may be perceived by patients and what resources are needed to support their use in routine care.
Methods
Study Design
We conducted a cross-sectional, qualitative interview study to explore and document current public perspectives and understanding on the use of MCEDs. The study protocol including informed consent of participants and was approved by the Ohio State University College of Medicine IRB (2023C0176, October 29, 2023, Columbus, Ohio, US). The study followed Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Appendix 1). 21
Recruitment and Data Collection
Participants were identified through the American Population Panel, a survey panel which comprises more than 55,000 US residents 18 years and older from all 50 states and Washington DC. 22 Eligible participants were aged 45–70 (consistent with other ongoing MCED research 7 ), US residents, and English-speaking. Members of the panel who met these criteria were emailed information about the study, and interested individuals completed a screener survey to ensure eligibility and gather demographic information for purposive sampling across race/ethnicity. A total of 1287 individuals completed this screener survey. Individuals were invited for interviews on a rolling basis based on their confirmed eligibility, order of sign-up, and race/ethnicity.
We used saturation of major ideas as the criterion for discontinuing data collection. Saturation is the gold-standard for sample size determinations in qualitative health services research. 23 While saturation varies depending on the research questions and participating sample, saturation in qualitative research can be reached at relatively low sample sizes, with most studies achieving saturation following 9–17 interviews. 24 Data collection in the current study continued until we had verified data validity through reaching saturation of major themes.
Interviews were conducted from November 2023 – February 2024 via Zoom. Participants were verbally consented. Each interview was led by a primary moderator (either NLC, a white, female health services researcher with training in qualitative and mixed methods research, or RN, a mixed-race, female researcher who received training to conduct interviews). An additional team member (NBC, a white, Hispanic female) took field notes. Members of the interview team briefly introduced themselves, their background, and interest in the research topic at the beginning of each interview. Participants were offered a $50 gift card for compensation, consistent with current practices. 25
Participants watched a three-minute educational video at the beginning of the interview. The study team developed the video to parallel the content and scope of what a provider might tell a patient about an MCED. The video is included in Appendix 2 and describes in simple language what an MCED is and its potential benefits and harms.
A semi-structured interview guide was informed by a literature review. The interview guide was structured to elicit awareness and understanding about MCEDs, perceptions of MCED characteristics including their benefits and drawbacks, and preferences for MCED use in clinical care. Adaptations to the interview guide were made throughout interviews as new topics emerged from participants. 26 Demographic information, health history, and health attitudes were collected using a closed-ended form at the end of each interview.
Data Analysis
Data were analyzed following Braun and Clark’s method for thematic analysis 27 and included a deductive coding approach based on the interview guide. 28 Members of our research team (NLC, NBC, RN) jointly reviewed a sub-set of 3 transcripts half-way through data collection to explore the content and identify preliminary themes. Preliminary themes were cleaned, condensed and applied to remaining transcripts. Themes were modified throughout the review of the remaining transcripts.
Results were triangulated through debriefing with members of the interview team and the larger study team. Direct quotes from the transcripts were selected to represent each theme. We used a semi-quantification approach to describe the salience of phenomena. Closed-ended questions regarding patient background were descriptively analyzed. Data were managed in Microsoft Excel.
Results
Participant Characteristics
Participant Demographic Characteristics (N = 27).

*Missing for n = 2.
Comprehension and Initial Impressions
No participants reported having heard of MCEDs prior to engagement with the study team (100%). After viewing the video, most participants (88%) were able to accurately describe the concept of MCEDs. Participants routinely highlighted that the test looked for the presence of cancer through a blood sample but did not predict cancer risk. Participants also noted that the video demonstrated to them that the tests had both potential benefits and drawbacks. Despite this, participants generally had a positive impression of the tests (85%).
Thematic Analysis
Illustrative Quotes.
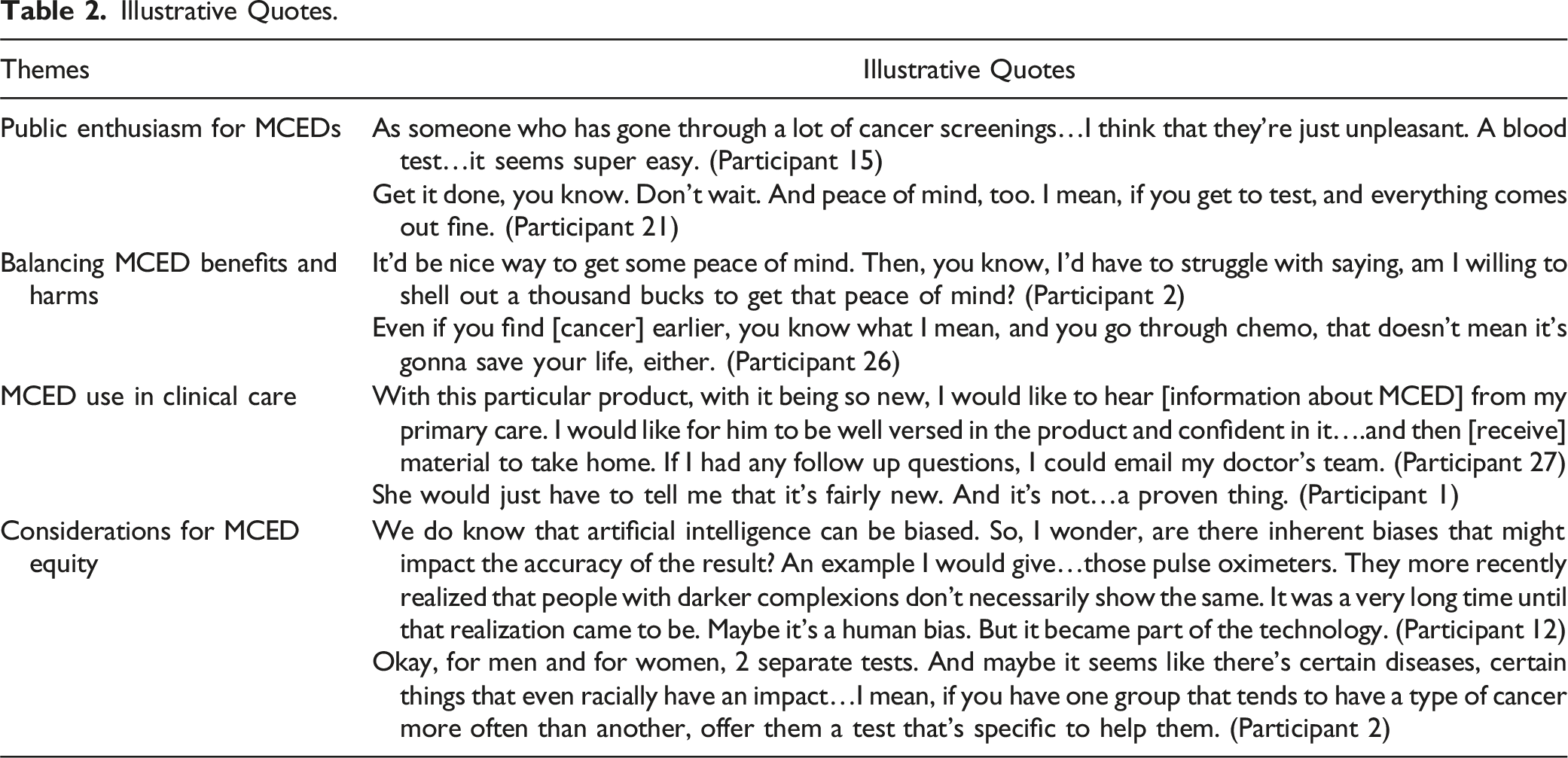
Public enthusiasm for MCEDs
Perceived Benefits and Harms of MCEDs (n = 27).

aTotal number of participants who discussed at least 1 form of convenience.
bTotal number of participants who discussed at least 1 form of inaccuracy.
The potential to identify multiple cancers from a single test was described as a benefit of MCEDs. Some participants hoped tests would include cancers that did have current screening tests, as those screening tests were often perceived as burdensome or uncomfortable. More participants perceived multiple cancer detection would be best used to look for cancers without established screenings. Participants also liked the idea that MCEDs might find cancer sooner, which was typically thought to lead to improved survival. Upon probing, several participants indicated that earlier detection of cancer was an important outcome irrespective of its ability to improve survival; “It’s better to know,” (Participant 17) remarked one participant.
The perceived convenience of MCEDs was typically attributed to the minimally invasive nature of the blood-based test. Several participants expressed that they hoped a test like this could one day lead to a need for fewer individual cancer screenings. Some participants described MCEDs to be “simple tests,” (Participants 18 & 22) particularly as compared to other cancer screenings which may require uncomfortable prep and procedures.
Balancing MCED benefits and harms
Despite enthusiasm for MCEDs, participants also recognized potential harms associated with their use and described the decision to use an MCED as requiring a tradeoff between benefit, risk, and uncertainty. Participants cited several potential drawbacks of MCEDs, including inaccuracies (96%), cost (85%), test-related anxiety (56%), and lack of evidence of effectiveness (22%).
Both the perception of MCEDs’ accuracy and the acceptability of that accuracy were widely variable. Participants raised concerns about various forms of inaccuracy including false positives, false negatives, and unknown signals of cancer origin. Some described accuracy as the most important characteristic of the test. Others made comparative judgements about MCED accuracy, highlighting that no tests are perfect and referencing examples of inaccuracy among established screenings.
MCEDs were seen to potentially reduce cancer anxiety by providing “peace of mind” that one does not have cancer. However, the potential for false positives and need for follow-up testing were seen as potentially canceling out this benefit. Multiple participants expressed concern that MCEDs could create more anxiety than they might alleviate.
Participants also weighed the value of the test in relation to its nearly $1000 out-of-pocket price. As one participant said: “It'd be a nice way to get some peace of mind…[but] am I willing to shell out a thousand bucks to get that peace of mind?” (Participant 2). While price was a drawback for most, several participants (11%) highlighted that MCEDs could be cost saving if they resulted in patients needing fewer separate cancer screenings or led to the earlier detection of cancer and averted the need for more advanced and costly treatments. Additionally, participants struggled with how to value MCEDs given their novelty and uncertain evidence of benefit. Participants largely understood that there was a lack of evidence, but how to weigh this lack of evidence against their enthusiasm gave many participants pause.
MCED use in clinical care
Participants had clear and relatively consistent preferences for how MCEDs might be integrated into clinical care, often favoring inclusion through primary care (44%). The prototypical pathway described by participants largely followed existing care pathways for cancer screening tests, including that the primary care provider would be the one to prescribe the test after a conversation with the patient, that the test would be done at a medical facility, and that the primary care provider (PCP) would read, interpret, and return results (Figure 1). Participants suggested that specialists such as oncologists should be engaged if MCED results were abnormal, and some indicated that there might be a role for new types of specialists with expertise in reading and interpreting MCED tests. Idealized pathway for MCED delivery. PCP = Primary care provider
Participants valued having the opportunity to discuss the test with their PCP prior to its ordering. They indicated that they would want this conversation to include a description of benefits and risks of taking the test, why it was being presented to the patient, and the PCP’s professional opinion on using the test. Several participants suggested that they should be provided with informational materials about MCEDs to inform their decision making. Additionally, most participants described wanting to know upfront about the process of getting an MCED, how they would get their results returned, and what the “game plan” (Respondents 2, 10, 17) would be to follow up on any concerning findings. Many participants emphasized the need for established care pathways upon the receipt of a positive test result. This included referrals to specialists and consulting with experts who might better understand how to interpret or follow-up after the tests.
A smaller group of participants (15%) preferred a process wherein PCPs were less engaged in the MCED process. One participant with this preference explained that they anticipated it might be cheaper to get the test direct-to-consumer. Another expressed that they did not have confidence that their PCP would be able to interpret the test, and instead would prefer to work directly with specialists.
Considerations for MCED equity
Several participants (44%) made projections about the potential equity impacts of MCEDs. Participants raised concerns that the high out-of-pocket cost of an MCED being (nearly $1000) posed a barrier to access. On average, participants indicated that a price of $200 (range $19.99-$500) would be more accessible. There was near universal agreement that if MCEDs were effective they should be paid for by insurance (96%), and that costs for additional diagnostic workups and any treatments needed based on MCED findings should be covered.
One participant raised concern about the design of MCEDs and their ability to benefit all people. Specifically, they called out potential racial biases in artificial intelligence algorithms that underpin MCEDs, and the potential for these biases to integrate themselves into technology.
Several participants were more optimistic, hoping that MCEDs might help improve health equity through the development of precision tests with the ability to look for cancers with the highest burden specific to subgroups of the population, such as those based on factors including age, sex, genetic ancestry, those who were medically underserved, or those with behavioral risk factors.
Discussion
Participants in this study were enthusiastic about the emerging use of MCEDs for cancer screening and indicated that they would be receptive to their use as a part of routine care. Anticipated barriers to the use of MCEDs included their novelty and lack of substantiated data on accuracy, the potential for false positives and negatives, and cost. Participants indicated that the decision to use an MCED required a personal benefit-risk tradeoff.
Participants preferred an approach for integrating MCEDs into care that followed existing cancer screening paradigms, including that the test be ordered, conducted, and results returned within the primary care context. This preference for integration may be an example of status quo bias, wherein individuals favor maintaining the current approach over developing a new one. 29 Participants in the study were largely positive about medical care and expressed trust in their primary care providers. They were also more adherent to cancer screening than the general population; all participants self-reported receiveing at least one cancer screening, and 78% self-reported being up to date on colorectal cancer screening, as compared 70% nationally. 30 While introducing MCEDs in primary care may be a preferred model for already engaged primary care patients, other and more innovative approaches may be useful to facilitate MCED implementation for individuals who are not routine primary care or cancer screening users. 31
The current qualitative study was designed at the outset to support the development of a large, national survey measuring public preferences for MCEDs. Conducting formative qualitative research to support the design of preference elicitation instruments has been demonstrated to improve the quality of preference elicitation surveys, 32 and which measure concepts relevant to survey takers.33,34 Qualitative work helps researchers to understand the phenomena of interest from the perspectives of end-users. 35 It can be used to help differentiate perspectives that are prevalent from those that are atypical. Findings from the current study which may be integrated into the development of a forthcoming preference survey include questions around acceptable tradeoffs between benefits and risks/harms of MCEDs, preferences for the integration of MCEDs into care, and assessment of how these preferences vary across patient and health care system factors.
Results from this study are consistent with previous research characterizing attitudes to MCEDs. In our study, 85% of participants indicated a positive impression of, or interest in using, an MCED. This is consistent with prior research estimating that 70%–80% of individuals offered an MCED would use one.17,18 As compared to a recent qualitative study exploring perceptions of MCEDs among members of the UK public, 20 our sample was more MCED naïve. Participants in the current study also expressed greater concern for the cost of MCEDs, potentially due to differences in health care payment systems across the countries and the pervasive mindset among our US participants that insurers will deny the tests.
While the ability to reduce cancer-specific and all-cause mortality has long been the established outcome measures for cancer screening trials, participants in our study expressed that the identification of cancer alone, even without an associated improvement in health outcomes, was a meaningful achievement. Endpoint evaluation for MCEDs has been hotly contested, particularly given a push by industry groups to use stage-shift, rather than mortality reduction, as the primary endpoint for MCED clinical trials. 32 However, very recent research has demonstrated that for many cancer types, earlier detection is not associated with improved cancer-specific mortality. 33 The current study demonstrates that many for many patients, detecting cancer in-and-of-itself is a meaningful outcome.
While MCEDs are far from mainstream, they do represent a rapidly growing industry in cancer screening. MCEDs had a market share of nearly US$1 billion in 2022, with projected growth to US$3 billion by 2030. 34 MCEDs are increasingly being offered as part of executive health programs across the US, including at large medical institutions. 35 Some health systems have established MCED clinics which provide access to comprehensive diagnostic evaluations. 36 More broadly, both public and private payers are beginning to engage in discussions around reimbursement for MCEDs.37,38 While current approaches to evaluating MCEDs from the patient perspective have been hypothetical in nature, asking individuals to project their preferences and perspectives, research should soon be able to consider the lived-experiences of using an MCED. This information will present important complementary insight to further refine MCEDs themselves, as well as the clinical care pathways used to administer them.
Limitations
There are several limitations in the current study. First, individuals in this study were recruited from a survey panel. Concerns regarding the generalizability and reliability of data collection through panels is pervasive; however, other approaches to capture participants from national samples are limited. Members of our study team have previously found that results from a nationally-representative panel to be generalizable to community-based samples. 39 Participants in our study self-reported receiving cancer diagnoses and using cancer screening at rates higher than national averages. These experiences may reflect their propensity to using and trusting cancer screenings. It is notable that even among these individuals, however, participants still identified drawbacks and limitations for the use of MCEDs. This study largely did not capture the perspectives of individuals who are hard-to-reach or who have divergent attitudes towards cancer screening generally. Further research is needed with a larger sample size to explore the generalizability of findings observed here, as well as to test for differences in perspectives on MCED across unique subgroups of the population.
It is possible that the introductory educational materials on MCEDs may have introduced bias. Although the developed video was designed to present both benefits and potential harms from MCEDs, a lack of established data on clinical utility of MCEDs limited our ability to present clinical data such as accuracy and safety. Additionally, participants in this study limited their perspectives on the value of MCEDs as related to their own individual care rather than as a tool to achieve population health. Cancer screening tests are typically evaluated from population perspective given that their potential benefit to any given individual is low, while risks and burdens are present for all. The exception of this was when thinking about health equity, wherein participants did make projections beyond their own experiences.
Conclusion
Interview participants from the US public expressed enthusiasm for including MCEDs as a part of clinical care but had reservations related to inaccuracy, cost, uncertainty of benefit, and potential inequitable benefits. Participants indicated that the decision to use an MCED required a personal benefit-risk tradeoff. Despite the limitations of current MCEDs, their use was still appealing to participants, supporting public interest the continued development of these emerging technologies.
Supplemental Material
Supplemental Material - Public Perspectives on Multi-Cancer Early Detection (MCED): A Qualitative Study
Supplemental Material for Public Perspectives on Multi-Cancer Early Detection (MCED): A Qualitative Study by Norah L. Crossnohere, Nicola B. Campoamor, Rosa Negash, Marie Wood, Jamie L. Studts, Mohamed I. Elsaid, Macarius Donneyong, Electra D. Paskett, Daniel E. Jonas, Daniel G. Stover, Chyke Doubeni, and John F. P. Bridges in Cancer Control
Footnotes
Author Contributions
Concept and design: Crossnohere, Bridges. Acquisition, analysis, or interpretation of data: Crossnohere, Negash, Campoamor, Bridges. Drafting of the manuscript: Crossnohere, Campoamor. Critical review of the manuscript for important intellectual content: All authors. Statistical Analysis: Campoamor, Negash. Obtaining funding: Crossnohere. Administrative, technical, or material support: Crossnohere, Negash, Campoamor. Supervision: Crossnohere, Bridges. Information on author access to data: Dr Crossnohere had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Crossnohere receives funding support through a grant to the university from Pfizer. This activity is not related to this project. Dr Paskett is the PI of grants to the university from Genentech, Pfizer, Merk Foundation, Astra Zeneca, and Guardant Health. She is also on advisory boards for Merck and GSK. None of these activities are related to this project.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by an PhRMA Foundation Early Career Starter Award in Value Assessment and Outcomes Research. JFPB holds an Innovation in Regulatory Science Award from the Burroughs Wellcome Fund. Funders had no role in design and conduct of the study, collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Previous Presentation
Earlier versions of this study were presented at the ISPOR 2024 Annual Meeting.
Ethical Statement
Data Availability Statement
Data are available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.