
Abstract
Human papillomavirus (HPV) is identified as the leading cause of cervical cancer which is the second most common cancer of females in the world. This study aimed to evaluate the effects of a community-based intervention on knowledge and practice of HPV prevention among married females aged 15 to 49 in rural areas, Vietnam. This study used a quasi-experimental design with serial cross-sectional surveys at one intervention commune (Chi Linh, Hai Duong) and one control commune at other province (Thanh Thuy, Phu Tho). Number of participants in these surveys were respectively 317 and 320 in Chi Linh and 334 and 335 in Thanh Thuy at pre- and postintervention period. The time of intervention was 15 months from April 2015 to June 2016. The study used behavior models to build up a logical framework for identifying related factors of knowledge and practice among females and developing intervention strategies. A difference-in-differences analysis approach was used to evaluate the effects of this intervention program. The study identified that the intervention had a significant change of knowledge of HPV prevention among married females after the intervention (odds ratio = 3.16, 95% confidence interval: 1.3-7.66) after adjusting for other confounders but no any significant change of practice of HPV prevention (eg, condom use, numbers of sexual partner, HPV vaccination, and screening test for cervical cancer). This might be caused by a short intervention program that did not lead to changes of practice but only change of knowledge.
Introduction
Cervical cancer has been among the most common types of cancer worldwide in women, just second to breast cancer. 1 –3 In Vietnam, a study conducted at Ho Chi Minh City in 2003 indicated that cervical cancer was the most popular cancer in women around menopause. 4 In 2018, statistics of Global Cancer Observatory (Globalcan 2018) taken data from Hochiminh City Cancer Registry identified that cervical cancer was at the 10th rank—in terms of both new cases and death—of all cancers for both sexes and was outside of the top 5 most frequent cancers for female in Vietnam. 2 However, a newest study of Thi Nguyen DN et al noted that there is no national cervical screening program in Vietnam, and data on cervical cancer are limited because Vietnam has 2 cancer registries covering urban population have only counted for about 20% of the national population. 5 Basing on the current available data, Diep NTD et al also indicated a significant increase of new cases of cervical cancer in Vietnam over the period 2013 to 2049.
Infection of human papillomavirus (HPV) has being seen a cause of cervical cancer. The HPV consists of unidentified, low-risk and high-risk strains. In most cases, HPV infections can be resolved on their own over time, but some HPV strains survive longer in human body and can cause cervical cancer, nasopharyngeal cancer, genital warts, and skin warts in both males and females. 6 –9 Women with HPV infection of high-risk type, for example, type 16 and 18 for Vietnamese women, have a high proclivity to have lesions develop in cervical tissues. 10 If not early detected and treated, these lesions can develop into invasive cervical cancer. 1 Therefore, HPV prevention plays an important role in cervical cancer prevention for women.
In Vietnam, cervical cancer prevention has been one of the national priorities of reproductive health care, since 2016. A national action plan on cervical cancer prevention and control aiming to improve health status and reduce the burden of morbidity and mortality in women in the coming decades was issued by Ministry of Health (MOH). 11 In this plan, knowledge of women about HPV infection and HPV vaccination was recommended to be one of important strategies for preventing HPV infections and reducing cervical cancer rate in Vietnam later on. 11
In fact, evidences worldwide have proved the safety and effects of HPV vaccines in HPV prevention. 12 However, the implementation of HPV vaccination for cervical cancer prevention in Vietnam has encountered many difficulties because of high price of vaccines and insufficient perception of community for HPV infection and HPV vaccination. 10,11 This has become more serious for females in rural areas because they are not often to get regular gynecological examination. 10 Therefore, improving knowledge, attitude, and behaviors of the HPV prevention for women, especially those of reproductive ages, has been needed as a crucial intervention to prevent cervical cancer in rural Vietnam. This study was conducted to evaluate a Behavioral Change Communication (BCC) program on HPV prevention among married women aged 15 to 49 in some rural communes in Vietnam.
Methodology
Settings and Participants
The participants were married females aged 15 to 49 years old in An Lac and Ben Tam commune, Chí Linh district, Hải Dương province (intervention group) and Tuvu and Thanh Thủy commune, Thanh Thủy district, and Phú Thọ province (untreated control group). The intervention site belongs to the Demographic Surveillance System named Chililab of the Hanoi University of Public Health. The control site has socioeconomic characteristics relatively similar to the intervention site and is far from the intervention site about 200 km. This distance could ensure the reduction of information contamination between 2 areas. Both these study sites have no previous intervention program of either reproductive health or cervical cancer or HPV prevention. All participants in the pre- and postintervention period did not have any history of HPV or cervical cancer.
Study Design, Sample Size, and Sampling
This is a quasi-experimental study with serial cross-sectional surveys (ie, independent surveys of pre- and postintervention period) for both untreated control and treated/intervention group. Sample size was calculated to compare the percentage of having knowledge of HPV prevention before and after intervention of intervention group with 5% of significance level and 80% of study power. A reference of Le Dinh Roanh et al stated that the percentage of having knowledge of HPV prevention in some communities without any intervention program was about 16%. Our intervention proposed to increase this percentage 10% after intervention, so the required sample size would be 315 married women at each group. In the fact, number of participants in the study is 317 in Chí Linh (intervention group) and 334 in Thanh Thủy (control group) at preintervention period; 320 in Chí Linh and 335 in Thanh Thủy at postintervention period (Figure 1).

Sampling procedures of the study. Note: Grey box is sampling procedure of pre-intervention stage. Note: Grey box is sampling procedure of pre-intervention stage
The study included 3 phases. The first phase was a baseline cross-sectional survey to investigate the background knowledge and practice of HPV prevention among married females at study sites and identify factors related to their knowledge and practice. This provided crucial information for developing intervention strategies. Phase 2 was an intervention program that conducted for all women in the intervention sites. In control sites, all regular health-care services and communication program were also implements as usual. Finally, phase 3 was another cross-sectional survey with participant samples independent from samples of the first phase.
A systematic random sampling was used to select participants (ie, sampling units) in this study. The sample frame was all married women from study sites, listed by commune health units. In the preintervention period, sample frame of intervention and control group consisted of 1586 and 1348 females, respectively. In the postintervention period, sample frame of intervention and control group consisted of 1975 and 1334 females, respectively. Basing on needed sample size, the sampling interval (SI) was calculated. In preintervention period, SI of intervention and control groups respectively was 1586/317 = 5 and 1348/334 = 4. In postintervention period, SI of intervention and control groups respectively was 1975/320 = 6 and 1334/335 = 4.
From the beginning random numbers, individuals would be recruited by repeatedly adding SI. Note that, in postintervention period, selected participants those were recruited in the preintervention periods would be excluded to ensure the independence of pre- and postintervention samples.
Intervention Strategies
Before developing intervention strategies, qualitative data collection methods (eg, in-depth interview and focus group discussion) were used to assess current availability of reproductive care programs and HPV prevention at study sites, possible supports and commitment of stakeholders, and potential barriers of this intervention study. Key informants included married females and their husbands, local health practitioners, representatives of women union, people committee, and youth union.
In addition, data from stage 1 were also analyzed to identify knowledge and practice of target intervention group and factors related to their knowledge and practice. Together with expert opinions—including 1 doctor specialized in HPV prevention and cervical cancer and 3 public health specialists with experiences of implementing interventions in community—intervention strategies for a BCC program were determined.
The intervention team at study site included health staffs of commune health stations (the leader of the team) and other stakeholders such as women union, people committee, and youth union. They were trained by doctors specialized in HPV prevention and public health specialists in health education and communication. They were also provided handbags decorating with logo and key message of this program “
Methods of Assessing the Effectiveness of the Intervention Program
Outcomes of Interest
The main outcomes of interest in this study were knowledge and practice of HPV prevention. In order to develop a questionnaire for assessing knowledge and practice of HPV prevention, we used on the logical framework built up from 3 logical models, namely the Health Belief Model, the theory of reasoned action and planned behavior, and the PRECEDE-PROCEED.
Knowledge questions were developed through different themes according to main components of the Health Believe Model, including the awareness of sensitivity to HPV (knowledge of subjects with high risk, risk behaviors, transmission routes, and ways of transmission prevention), the awareness of the severity of HPV (knowledge of symptoms, consequences, and treatment of HPV infection), and the awareness about benefits of prevention (knowledge of HPV vaccination) and the awareness about barriers of implementing preventive practice (access to and prices of HPV vaccines). These questions were scored 0 for wrong answers and 0.5 or 1 for right answers (weighting by the importance of the answers). As a result, knowledge variable was counted by all these questions. Participants with higher score mean better knowledge of HPV prevention.
Practice of HPV prevention was evaluated through condom use, numbers of sexual partners in 1 year, and HPV vaccination. This study also evaluated the practice of cervical cancer through screening examination of cervical cancer—including tests of HPV infection. All outcomes were self-reported by participants (see Appendix).
Effectiveness of the Intervention Program
The effectiveness of the intervention program was evaluated through difference-in-differences (DID) analysis. Theoretically, DID is often used in quasi-experimental designs in which data are collected longitudinally in intervention and control groups. Difference-in-differences is often used to estimate the impact of an intervention by comparing changes in outcomes over time between the intervention and control groups. This DID approach eliminates errors in comparison in the postintervention period between the intervention and control groups; such difference could be a result of the natural difference between the 2 groups. This method also eliminates discrepancies in time-based comparisons within the intervention group that changes in the intervention group might be a result of other causes (not intervention).
Ethical Issue
This study was approved by IRB of the Vietnam University of Traditional Medicine. The decision number is 789/QĐ-HV issued on November 29, 2013. All participants were explained purposes of the study, their voluntary participation, and their rights to withdraw from the study at any time without any threats or disadvantages. They were also asked to complete a consent form before collecting data.
Results
Table 1 shows demographic characteristics of participants of the study before (stage 1) and after (stage 3) intervention program. Samples of both intervention and untreated control group before and after intervention seem to be not different in age, marital status, ethnic group, education status, and the number of children. Most married females in the study were more than 30 years old (84.9% in the preintervention and 78.9% in the postintervention period) and about 95% of participants were the Kinh. Most of participants were living with their husbands (96% and 96.5% in pre- and postintervention period) and 83.4% and 85.3% of pre- and postintervention study population had less than 2 children.
Demographic Characteristics of Women Aged 15 to 49 Participating in the Study Before and After the Intervention.a

aDifferences in characteristics of pre- and postintervention study samples were tested by χ2 test.
bDifferences between intervention and control group in pre- and postintervention period were significant at P < .001.
cDifferences between intervention and control group in postintervention period were significant at P < .05.
There were differences in occupation, education level, and economic status between intervention and control group. The percentage of farmer in control group was higher than in intervention group for both pre- and postintervention period, accounted for the highest percentage in both groups before and after the intervention. Education level of participants was similar between 2 groups in preintervention period, but this was different in the period afterward. Indeed, the percentage of participants with education level of high school and upper in intervention group was higher than in control group (51.2% and 42.1%, respectively). In addition, the percentage of participants from poor households in intervention group was smaller than in control group (4.7% and 11.4%), while the reverse was seen after the intervention (7.5% and 2.1%).
Knowledge of HPV prevention of participants was scored from 0 (the lowest) and 35 (the highest) points. As a result, knowledge score of participants before intervention period was from 0 to 26.5 in intervention group and from 0 to 21.0 in control group. Due to a significant percentage of 0 point, we used the median of knowledge scores that were more than 0 in preintervention period to divided participants into 3 groups: group of 0 point, group of score less than the median (<12.5) and group of score over the median (≥12.5). This cut-off point was also used to categorize knowledge of participants at postintervention period.
Figure 2 illustrates the percentage of participants without knowledge of HPV prevention (knowledge score of 0) before intervention period in control group was higher than in intervention group. After intervention, the percentage of no knowledge sharply decreased in intervention group (47.9%-21.9%), whereas this percentage lightly decreased in control group (60.2%-58.8%). Similarly, the percentage of knowledge score more than 12.5 increased significantly in intervention group (27.5%-54.3%), whereas the increase of this percentage in control group was a little (21%-27.2%).

Percentages of knowledge of human papillomavirus (HPV) prevention among intervention and control group before and after intervention period.
Figure 3 shows little changes of behaviors related to HPV and cervical cancer prevention, including currently using condom (yes vs no), having 1 sexual partner or less in 1 year (1 or less vs more than 1 sexual partners), and participating in screening examination of cervical cancer (yes vs no). In intervention group, all behaviors have positive changes after intervention as the proportion of using condom, having 1 sexual partner or less, and participating in screening increase in postintervention (13.9% vs 18.1%, P = .15; 92.4% vs 95%, P = .17; and 22.4% vs 31.4%, P = .01; respectively). Meanwhile, these behaviors in control group have worse trend of change, except participating in cervical cancer screening (13.8% vs 13.1%, P = .79; 97.9% vs 97.3%, P = .61; and 13.2% vs 18.9%, P = .04; respectively).

Percentages of human papillomavirus (HPV) prevention behaviors among intervention and control group before and after intervention period.
As seen in the methodology, DID analysis was used to assess the effectiveness of intervention on knowledge of HPV prevention. In this analysis, knowledge of HPV prevention was recoded into 2 groups: group of no knowledge (score of 0) and few knowledge (score less than 12.5) and group of knowledge score 12.5 and over. Multivariate logistic regression with an interaction field intervention × time was used to conduct DID analysis. Result of DID analysis presented in the Table 2 shows that the intervention brought an increase of HPV prevention knowledge to married females aged 15 to 49 in intervention sites. Indeed, married females in intervention sites were 2.21 × 1.43 = 3.16 times (95% confidence interval: 1.30-7.66) of likely to get a better score (12.5 and over) of HPV prevention knowledge compared to the control group after adjusting for age, education level, economic status, and number of their child.
Results of DID Analysis to Assess the Effectiveness of the Intervention on Knowledge of HPV Prevention.a

Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; DID, difference-in-differences, HPV, human papillomavirus.
aIntervention (0—control, 1—intervention), time (0—preintervention, 1—postintervention), age group (0—15 to 29 years, 1—30 to 49 years), education level (0—secondary education and lower, 1—high school education and higher), economic conditions (0—non-poor, 1—poor), and the number of children (0—>2 children, 1—≤ 2). n = 651.
Table 3 illustrates the effects of intervention on 3 behaviors of interest, including condom use when having sex (irregular use vs regular use), number of sexual partners in 1 year (more than one partner vs one partner), and screening test of cervical cancer (not screened vs screened). Results in the Table 3 show that intervention had no effect on these behavior because of the statistical insignificance of the interaction field intervention × time in the models.
Results of DID Analysis to Assess the Effectiveness of the Intervention on Behaviors of HPV Prevention.a
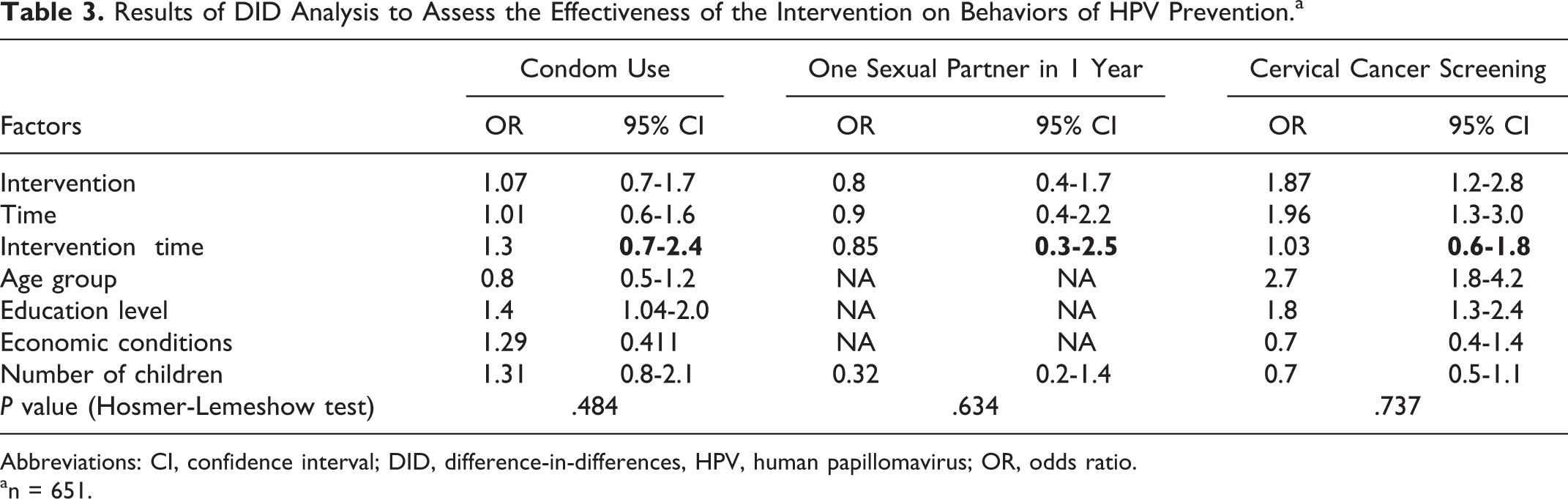
Abbreviations: CI, confidence interval; DID, difference-in-differences, HPV, human papillomavirus; OR, odds ratio.
an = 651.
Discussion
After the intervention, the proportion of women with better knowledge of HPV prevention in the intervention site increased significantly. The proportion of women with high knowledge scores (≥12.5) nearly doubled from the preintervention figure, compared to the 6% rise in the control site. Moreover, a more noticeable result is the proportion of women with 0 knowledge scores halved after the intervention (from 47.9% down to 21.9%), while in the control site, this figure nearly remained the same (60.2% compared to 58.8%). This result is consistent with that in a study conducted by Yanikkerem in Turkey in 2014 which applied the same intervention strategies. 13
In order to confirm the effects of the intervention on knowledge of HPV prevention by dealing with confounding factors derived from the differences between the intervention and control groups, and between pre- and postintervention period, we used the DID analysis. The DID is a useful analytical technique to use when intervention studies could not perform randomization at the individual level. Thus, this technique is used in quasi-experimental designs in which data are collected vertically in the intervention and control groups. The DID is often used to estimate the impact of an intervention by comparing changes in outcomes over time between the intervention and control groups. 14 –16 Our study is a quasi-experimental design in which the intervention and control groups were measured through 2 different stages (through 2 different cross-sectional studies), so this method of analysis can be applied. The result of this analysis confirmed that the intervention had the most prominent effects on the knowledge of HPV prevention. Indeed, the knowledge of women after intervention at the intervention sites significantly increased compared to that before the intervention (P < .05). The likely of getting better HPV prevention knowledge of female in intervention site was 3.16 times higher than that in the control group after age, education level, household economic status, and the number of children adjusted.
The results of our intervention had no an obvious impact on some HPV prevention behaviors. Regular condom use when having sex has been proved to be an effective measure in reducing the risk of HPV infection; thus, it was one of the main aspects we focused on when carrying out communication activities in our intervention program. The postintervention result showed that the proportion of using regularly condoms when having sex among females in intervention site was slightly higher than that in the control site. Similarly, the proportion of having only 1 sexual partner in a year and the proportion of cervical cancer screening after intervention at intervention sites were higher than before intervention. The increase of these proportion between after and before intervention at intervention sites was also higher than at control sites, but the difference between 2 groups is not statistically significant. This univariate analysis results are the same with the DID analysis that showed there was no effectiveness of the intervention on behaviors. These results were similar to those in some other studies worldwide applying the same intervention approaches for short periods of time. 13 There should be a plan on sustaining the integration of the intervention into the existing comprehensive health-care program, as well as monitoring and supporting the intervention sites for longer periods of time in order to make expected behavioral changes.
Our DID analyses showed that there was no statistically significant effectiveness of our intervention program on females’ behavior of cervical cancer screening while the proportion of women attending cervical cancer screening increased by 1.4 times after the intervention in both intervention and control sites. This increase could be caused by other factors such as accessibility and affordability not only by our intervention. A possible explanation is that the screening may result from the plan and advocacy of different sectors and health facilities in either local areas. The data from some other surveys show that in recent years the proportions of women screened for reproductive tract infections, including HPV infection, and cervical cancer have all increased in many parts of the country. 5,10
Our study has a limitation of design and sampling. The serial cross-sectional design could be suitable for community-based intervention program, but it would be difficult to have evidences for the effectiveness of the intervention because samples at pre- and postintervention period are different. As a result, the intervention group is not comparable to control group regarding background information, especially socioeconomic status. In our study, the intervention group seems to have higher socioeconomic status than the control group, so the intervention group would be more likely make a greater change than the control one. In another word, our estimation of the effectiveness of the intervention program could be overestimated. In addition, the DID technique provided better analyses of causal inference between intervention and its outcomes for this serial cross-sectional design, but it depended on certain assumptions, especially the assumption of common trend. We did not deal well with it in this study, so our results are under this assumption.
Moreover, systematic random sampling was conducted on women aged 15 to 49 years for each stages of our study at both intervention and control sites, but the average age of participants was about 37. In other words, older women had a higher opportunity of participating in the study than younger women in our study. One explanation is that young women in these study sites often migrate to the city rather than old women who stay at their home for farm works. This should be taken into account when making the generalization of study results.
Conclusion
In summary, we have demonstrated that our intervention strategies had significant effects on knowledge of HPV prevention. But the intervention program had no effect on HPV prevention practice due to short time of intervention.
Recommendations
Intervention strategies used in this study should be considered to expand to other provinces in Vietnam with implementation strategies suitable for the context and target audience in certain settings. Time of intervention should be lengthened more (eg, 1 year) to achieve changes of HPV prevention practice. In addition, this study is a part of the research project funded by Vietnam MOH “Cost-effectiveness assessment of HPV prevention program for Vietnamese women” that used both quantitative and qualitative data collection methods to provide more detailed recommendation for HPV prevention at rural areas in Vietnam. 17 Further research on HPV prevention need to refer this research project.
Footnotes
Appendix
Authors’ Note
The protocol of this study was approved by the Scientific and Ethical Committee in Biomedical Research, Vietnam University of Traditional Medicine. The decision number is 789/QĐ-HV issued on November 29, 2013. All participants in the study were asked for their consent before collecting data, and all had complete rights to withdraw from the study at any time without any threats or disadvantages.
Acknowledgments
The authors are grateful to all people at study sites for their support and collaboration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Vietnam MOH.