
Abstract
Background:
This study investigates the effect of body mass index (BMI) on complications and satisfaction in patients who underwent thyroidectomy and lateral neck dissection.
Methods:
We retrospectively reviewed 386 patients with papillary thyroid cancer who underwent total thyroidectomy and lateral neck dissection between January 2013 and December 2016. We compared variables including population characteristics, subjective satisfaction, and complications in nonobese (BMI < 28.0 kg/m2) and obese (BMI ≥ 28.0 kg/m2) patients.
Results:
Obesity was associated with an increased risk of postoperative hemorrhage (POH) (P = .014), accessory nerve injury (P < .001), operative time (P < .001) and infection (P = .013). However, obese patients had higher subjective satisfaction and Vancouver Scar Scale (VSS) scores (P < .05).
Conclusions:
Obesity was associated with increased risk of POH, injury of the SAN, and infection. Interestingly, we found that obese patients had higher subjective satisfaction and VSS scores.
Introduction
Papillary thyroid cancer (PTC) has increased rapidly in recent decades, especially among women. 1,2 Even so, its prognosis is favorable after surgical therapy, and the 10-year survival rate in the past few decades has exceeded 90%. 3 Lateral neck metastases (LNM) occur in up to 40% of all cases, severely affecting postoperative quality of life and constituting a known independent risk factor for local recurrence. 4 Lateral neck dissection (LND) and total thyroidectomy (TT) are performed in patients with clinically positive neck lymph nodes.
Obesity has been recognized as a risk factor for endocrine cancer, esophageal adenocarcinoma, colon cancer, renal cancer, and thyroid cancer. A 5 kg/m2 increase in body mass index (BMI) has been strongly connected with PTC. 5 –7 An increasing rate of obesity is not only driving up medical costs but is also increasing the incidence of complications. Presently, more patients with obesity are undergoing surgical procedures, and there is growing interest in the effect of BMI on surgical outcomes. Previous research shows that obese patients appear to require surgeries of longer duration and they sustain more complications after cervical endocrine procedures than do nonobese patients. Nevertheless, substantial controversy exists regarding the effect of BMI on clinical outcome in numerous surgical fields. 8 –11
No study has assessed the surgical safety for obese patients with PTC having LNM. The aim of the present retrospective study is to further investigate this topic.
Method
Our study was approved by the ethics committee of the Affiliated Cancer Hospital of Zhengzhou University (approval no. 2018136). All patients provided written informed consent prior to enrollment in the study. All related procedures were consistent with the ethics committee regulations. The study was performed in accordance with the Declaration of Helsinki. This retrospective study involved 386 patients between January 2013 and December 2016 from the Affiliated Cancer Hospital of Zhengzhou University. All patients underwent TT and LND for PTC and had evidence of LNM by preoperative imaging or fine-needle aspiration cytology. The thresholds proposed by the Working Group on Obesity in China in 2003 for categorizing Chinese adults as overweight or obese were used in this study. Thus, patients were divided into 2 groups: nonobese (BMI < 28.0 kg/m2) and obese (BMI ≥ 28.0 kg/m2). 12
Neck length is defined as the vertical distance from the midpoint of the inferior border of the mandible to the ipsilateral clavicle when the neck is fully extended in the supine position (Figure 1). Neck circumference is the circumference of the upper edge of the cyclic cartilage when standing upright (Figure 2). Measurements of the neck circumference, incision length, and neck length were performed by 2 endocrinologists specializing in endocrinology of the neck with a combined work experience of more than 15 years. The data recorded were the average of 2 measurements, and all measurements were obtained in the upright position.

Measurement of neck length.

Measurement of neck circumference.
The Vancouver Scar Scale (VSS) was used to investigate healing of the incision in patients after surgery. The VSS observes 4 physical characteristics of scars: vascularity, pigmentation, pliability, and height. The maximum score is 13, which represents the worst outcome in terms of appearance of the scar. The higher the score of each item is, the worse the patient’s satisfaction would be. In addition, all patients were invited to fill out their own questionnaires on their satisfaction with the incision using a 10-point Likert scale (with 1 being very unsatisfied and 10 being very satisfied) 6 months after surgery. Similar scales have been used successfully in previous trials assessing satisfaction.
13,14
Observations and records of the postoperative complications including hypocalcemia, recurrent laryngeal nerve (RLN) palsy, accessory nerve injury, chyle leakage, and infection were collected. After thyroidectomy, all patients were received TSH suppression therapy with levothyroxine and radioactive iodine (RAI) ablation. They were followed up for at least 12 months. Patient follow-up examinations consisted of neck ultrasound and monitoring of serum Tg and TgAb levels every 6 months during suppressive
Statistical Analysis
Data were analyzed using descriptive statistical methods with SPSS software (version 20.0 for Windows; IBM Corp, Armonk, New York). Chi-square tests supplemented with Fisher exact tests were used. Continuous variables were analyzed using Student t test and were expressed as the mean ± standard deviation. We analyzed predictive factors for accessory nerve injury including age, gender, BMI, tumor size, neck circumference, neck length, and LND. Logistic regression analysis was performed for multivariate analysis in order to determine predictive factors associated with accessory nerve injury. The results were considered statistically significant if P values were ≤.05.
Results
In total, 294 (76.2%) patients were in the nonobese group and 92 (23.8%) patients were in the obese group; 27.2% (n = 105) and 72.8% (n = 281) of the patients were males and females, respectively (Table 1). Body mass indexes for the nonobese and obese groups were 23.57 ± 7.78 and 30.46 ± 6.27, respectively. The mean ages of nonobese and obese groups were 41.62 ± 15.4 and 50.73 ± 12.9 years, respectively. The mean age was significantly lower in nonobese patients than in obese patients, reflecting the higher prevalence of obesity in middle-aged adults versus young adults (P < .001). The mean incision lengths were significantly different, with a mean of 11.35 ± 1.62 cm in the nonobese group and 13.93 ± 2.71 cm in the obese group (P < .001). People who were obese had a larger neck circumference (39.89 ± 3.13 cm vs 32.64 ± 1.73 cm, P < .001) and shorter neck length (9.35 ± 1.62 cm vs 13.17 ± 2.15 cm, P < .001). Furthermore, the obese group had longer operation times (175.16 ± 24.91 minutes vs 154.61 ± 38.79 minutes, P < .001). However, there was no significant difference in blood loss (74.68 ± 12.5 mL vs 83.16 ± 9.81 mL, P = .463) or drainage (173.28 ± 30.15 mL vs 181.64 ± 23.51 mL, P = .619) between the groups. Seventy-three patients underwent bilateral neck dissection (regions II-VI), and 313 patients underwent unilateral neck dissection (regions II-VI). Tumour sizes in the nonobese and obese groups were 1.58 ± 0.73 cm and 1.67 ± 0.91 cm, respectively (P < .001).
Demographic and Clinical Characteristics of Patients.a
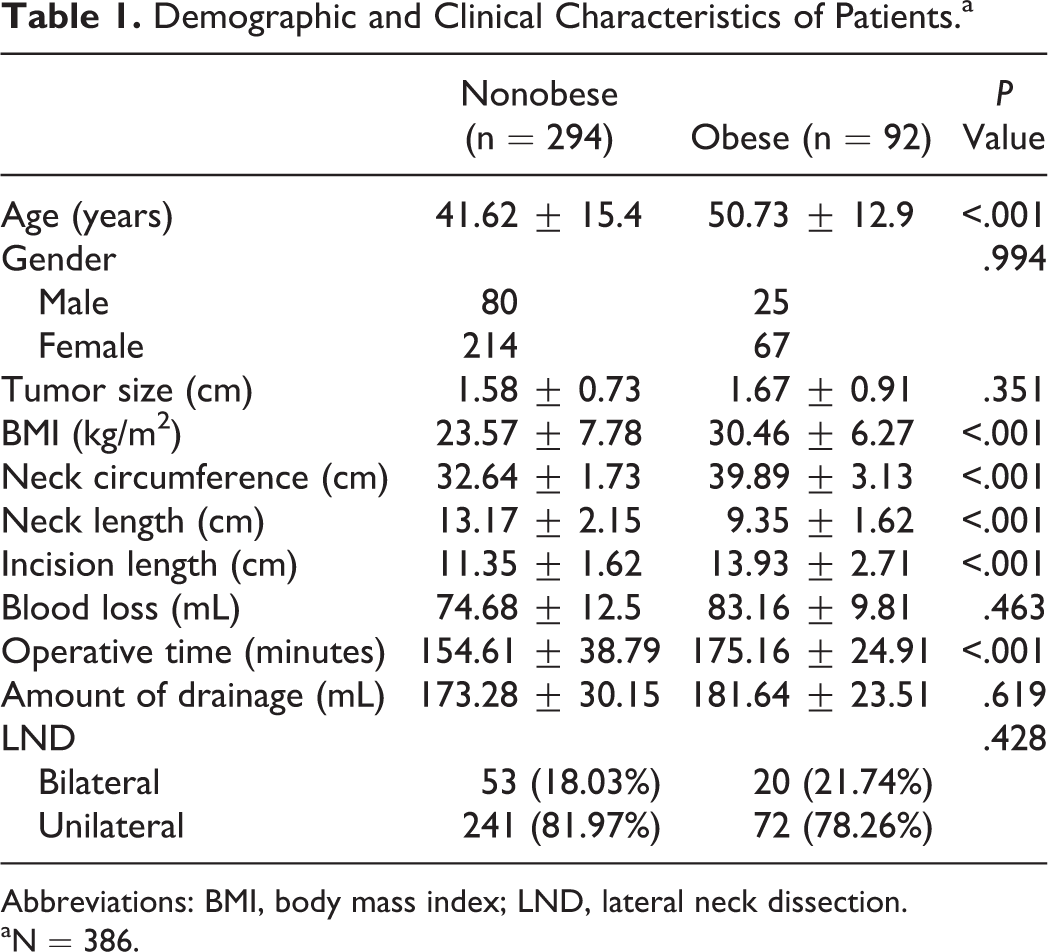
Abbreviations: BMI, body mass index; LND, lateral neck dissection.
aN = 386.
A total of 120 (31.01%) patients had postoperative complications, of whom 85 were obese patients and 35 were nonobese (P = .099; Table 2). The most frequent complication was transient hypocalcemia in 101 (26.17%) patients. At 6-month follow-up, 99 patients did not need oral calcium tablets or vitamin D analogue therapy. However, 2 patients still needed medication to reduce spasms. Neither transient hypocalcaemia (P = .107) nor permanent hypocalcaemia (P = .428) were significantly different between groups. Three (0.08%) patients had bilateral paresis of the RLN, and 18 (4.66%) patients had unilateral paresis of the RLN; however, all patients had normal vocal cord function after 6 months. Bilateral (P = .698) or unilateral (P = .125) paresis of the RLN showed insignificant differences between the groups. Nineteen (4.92%) patients suffered postoperative hemorrhage (POH), and there was a significantly positive correlation between POH and BMI (P = .014). Two (0.52%) patients, one from each group, suffered chyle leakage; both resolved after 1 week of local pressurization. The increase in BMI did not increase the incidence of chyle leakage (P = .389). Infection was found in 2 (0.68%) out of 294 patients in the nonobese group and in 4 (4.35%) out of 92 patients in the obese group (P = .013). The rate of SAN injury (XI nerve) was 21.24%. Thirty-seven obese patients had shoulder weakness compared to 45 patients in the nonobese group (P < .001).
Incidence of Complication.
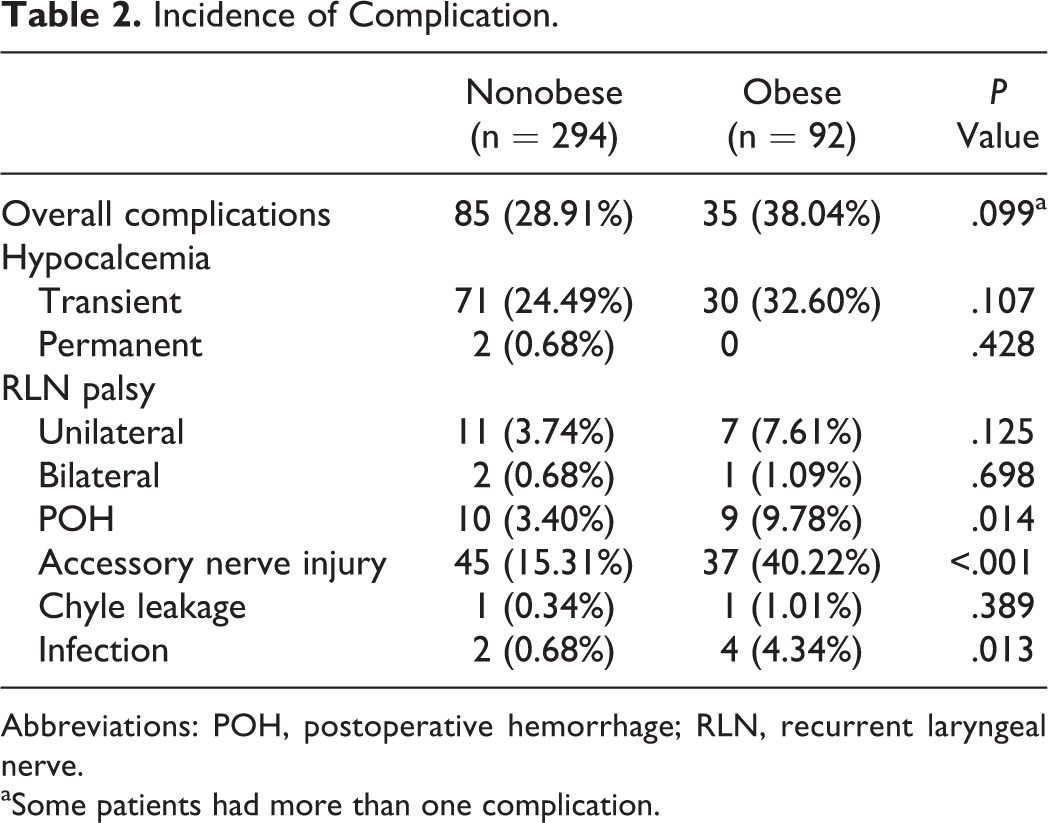
Abbreviations: POH, postoperative hemorrhage; RLN, recurrent laryngeal nerve.
aSome patients had more than one complication.
Univariate analysis revealed that accessory nerve injury was associated with BMI (P < .001), neck circumference (P = .004), and neck length (P < .001). However, age (P = .091), gender (P = .189), tumor size (P = .386), and lymph node dissection (P = .081) did not increase the risk of accessory nerve injury (Table 3). Multivariate logistic regression analysis showed that BMI (odds ratio = 1.93, 95% confidence interval [CI] = 1.57-7.16, P < .001), neck circumference (odds ratio = 2.162, 95% CI = 1.39-5.02, P < .001) and neck length (odds ratio = 0.67, 95% CI = 0.14-0.87, P < .001) were significantly correlated with an increased risk for accessory nerve injury.
Risk Factors for Accessory Nerve Injury.

Abbreviations: ANI, accessory nerve injury; LND, lateral neck dissection.
aThirty-four and 12 are the mean neck circumference and neck length, respectively, for all 386 patients in this study.
Our team previously conducted a multivariate analysis of risk factors for POH which showed that BMI was an independent risk factor for POH. 15 Because infection was rare in both groups, we did not conduct further statistical analysis.
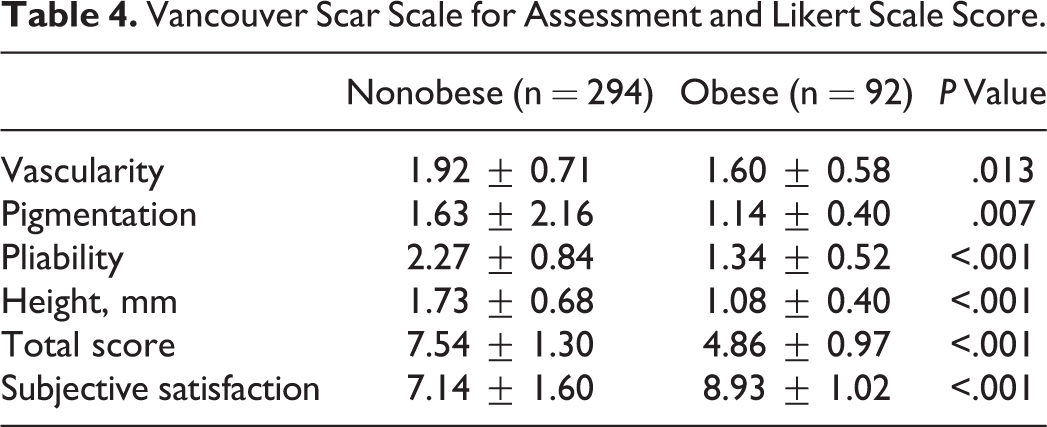
The mean VSS score of the nonobese group was higher (indicating reduced cosmetic outcome) than that of the obese group (Table 4). The 4 features of the VSS scores differed significantly (P < .05). The satisfaction scores of the patients in the obese group were higher than those of the nonobese group (8.93 ± 1.02 vs 7.14 ± 1.60, P < .001).
Vancouver Scar Scale for Assessment and Likert Scale Score.
Discussion
The key finding of our study was that there were significant differences in satisfaction scores and VSS scores between obese and nonobese patients. It appears obvious that patients would be more pleased with the cosmetic appearance of shorter thyroidectomy incisions. However, O’Connell et al 13 found that larger cervical scars created in thyroidectomy or parathyroidectomy surgery did not translate into decreased patient satisfaction with their scar result, even though they were more readily visible to naive viewers. These results are supported by a prospective study performed by Kim et al in 2013 16 that evaluated the effect of scar length on patient satisfaction in 2041 patients; this study also revealed that a shorter neck incision length during thyroid surgery did not improve satisfaction.
Satisfaction with the thyroidectomy scar is more complex than simply considering length. Other factors are also associated with patient satisfaction, including careful positioning of the incision using appropriate skin creases, pigmentation, incision symmetry, the patient’s physique, postoperative care, and suturing techniques. Previous studies did not provide evidence of the real effect of BMI on patient satisfaction after cervical endocrine operations. The present work provides deeper evidence that higher BMI is linked to higher patient satisfaction. Although the incisions in the obese group were significantly longer, obese patients have deeper skin folds; thus, scars are easier to hide after surgery. Patients with higher BMI have thicker subcutaneous tissue with less tension, which makes it easier to align the skin during subcutaneous stitching. Additionally, these patients are more concerned about the treatment of the disease rather than the scars. Furthermore, lower satisfaction may be because normal-weight patients are more active before surgery, and this provides higher expectations for the function of treatment. 11,17
As confirmed in many studies, obesity leads to an increase in operative time; however, this is especially true for neck surgery. 8,18 Our findings in the present study agrees with these previously acquired results. Obese patients have neck extension defects that lead to limited surgical site exposure and increased difficulty in surgery, which possibly resulting in longer operation times. Thyroidectomy and neck dissection often require longer times to complete.
Obesity is significantly linked to decreases in plasma fibrinogen after surgery. When massive blood loss occurs intraoperatively, patients with higher BMI need to consume more plasma fibrinogen to clot. Therefore, obese patients are at risk for postoperative fibrinogen insufficiency. 19,20 Ogunsua et al 21 found that the risk of major bleeding on warfarin achieves statistical significance when obese patients are compared to nonobese patients. This risk was sufficient to warrant hospitalization in patients who had gastrointestinal and intracranial hemorrhage. Zhang et al 15 discovered that a BMI greater than 30 kg/m2 increased the risk of POH nearly 6 times after TT. In the current study, POH occurred in 9 (10%) obese and 10 (3.4%) nonobese patients, with a significant difference between the 2 groups (P = .014). Because of neck extension defects in obese patients, it is easy to injure blood vessels under conditions of poor exposure.
Obesity has been thought to be related to an increased risk of postoperative infection. Prevention of nosocomial infections has an obvious clinical impact; up to 20% of deaths due to sepsis are caused by invasive surgical infections. The association is most pronounced in orthopedics, cardiac, blood vessel and gastrointestinal surgery. This also has been shown numerous times in thyroid surgery. 22 –24 Both Buerba et al 18 and Elfenbein et al 25 found that obesity was the most significant risk factor among preoperative variables associated with postoperative infection. In the present study, the infection rate in the obese group was 5 times higher than that of the nonobese group (0.68% vs 4.35% P = .013). The prevalence of postoperative infections was higher than those of previous reports. 26 This may be because all patients underwent cervical lymph node dissection and received drainage after surgery. Larger surgical range, drainage placement, and longer operative time may increase the risk of infection. 27,28
The rate of accessory nerve injury in obese patients was higher (40.22%) in this study. This multicentre analysis demonstrated that BMI, neck circumference, and neck length were associated with a higher accessory nerve injury rate. We speculate that there may be several reasons for this result. First, the length and circumference of neck is shorter and thicker in obese patients, and these conditions are not conducive to the dissection of level IIB lymph nodes and exposure of the accessory nerve. Second, all patients underwent V-level lymph node dissection, and clearance of the posterior triangle of the neck increases shoulder morbidity. Increased morbidity is related to the cutting of the branch of the trapezius muscle of the cervical plexus. Third, obese patients need a higher dose of muscle relaxants in order to fully relax the muscles and facilitate traction exposure when cleaning the posterior lymph nodes in the II and V regions. The change in force of the surgical assistant when pulling the SAN also produces invisible damage. 29,30
Our overall complication rate was 31.01%. The incidence of complications in our study was higher than previously reported. A possible explanation for this finding might be that all patients underwent TT and LND, and a wider range of surgery tends to increase the complication risks; central and lateral cervical lymph node dissection was associated with high morbidity. 27,31
There are major limitations to this study. First, it is a retrospective, nonrandomized study that might exhibit bias. Second, only 386 patients were enrolled in the current study, and we divided patients into obese and nonobese groups. Further multicentre large sample size studies are needed to report 3 groups (normal, overweight, obese) to fully discuss the impact of BMI on complications and satisfaction in patients with PTC and LNM.
Conclusion
The results of our retrospective study confirm that obesity is associated with an increased risk of POH, accessory nerve injury, and infection. Interestingly, we found that obese patients have higher subjective satisfaction and VSS scores. When surgery is performed on obese patients, the incision and flap must be free to reveal the operative field to avoid damage to blood vessels and nerves.
Footnotes
Authors’ Note
The authors claim that none of the material in the paper has been published or is under consideration for publication elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.