
Abstract
Purpose
This cross-sectional study explored associations of BMI with renal cell carcinoma (RCC) pathological grade and stage, and how these associations vary by BMI-related factors, to better understand the obesity paradox.
Method
Data was obtained from 2 academic institutions for this cross-sectional study of RCC patients who underwent surgical treatment. Logistic regression models were used to identify BMI-related factors and to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for diagnosis with high grade or advanced stage.
Results
A total of 1949 cases, 1526 from Roswell Park Comprehensive Cancer Center (Roswell Park) and 423 from University of Arizona Baner-University Medical Center Tucson (BUMCT), were included. In both datasets, obesity was significantly associated with lower odds of high grade compared with non-obese (OR 0.69, 95% CI 0.54-0.88 in Roswell Park, OR 0.62, 95% CI 0.41-0.94 in BUMCT). In Roswell Park, unintentional weight loss at the time of surgery was associated with higher odds of high grade (OR 3.81, 95% CI 2.38-6.09) and advanced stage (OR 4.12, 95% CI 2.74-6.20). In both datasets, older age was associated with reduced odds of obesity and higher odds of high grade, and heterogeneous associations between obesity and high grade by age group were observed (PInteraction = 0.001) in Roswell Park. Former smokers had increased odds of obesity in BUMCT and increased odds of high grade in both datasets. In BUMCT, obesity was significantly associated with reduced odds of high grade in patients who never smoked, not in patients who have smoked, but heterogeneity by smoking status was not significant.
Conclusion
Higher BMI was linked to a lower likelihood of high-risk RCC pathological characteristics consistent with the obesity paradox. However, BMI-related factors, including older age and smoking, were associated with higher odds of RCC severity, potentially modifying the associations between BMI and severity.
Plain Language Summary
Although obesity increases kidney cancer risk, obese patients often have better kidney cancer survival. This phenomenon is known as the obesity paradox. This study explored the relationships between BMI and kidney cancer pathological grade and stage and how these relationships vary by BMI-related factors to better understand the obesity paradox. Data was obtained from Roswell Park Comprehensive Cancer Center (Roswell Park) and University of Arizona Baner-University Medical Center Tucson (BUMCT) for this study among patients who underwent surgical treatment. A total of 1949 patients, 1526 from Roswell Park and 423 from BUMCT, were included. In both datasets, obesity was significantly associated with lower likelihood of diagnosis with high grade compared with non-obese. In Roswell Park, unintentional weight loss at the time of surgery was more likely to have high grade and advanced stage kidney cancer. In both datasets, older age was associated with reduced likelihood of obesity and higher likelihood of high grade, and a different pattern of associations between obesity and high grade by age group were observed in Roswell Park. Former smokers were more likely to be obese in BUMCT and were more likely to have high grade kidney cancer in both datasets. In BUMCT, obesity was significantly associated with a reduced likelihood of diagnosis with high grade in patients who never smoked, not in patients who have smoked, but the differences by smoking status were not significant. In conclusion, higher BMI was linked to a lower likelihood of high-risk kidney cancer pathological characteristics consistent with the obesity paradox. However, BMI-related factors, including older age and smoking, were associated with higher likelihood of kidney cancer severity and influenced the associations between BMI and severity.
Background
Kidney cancer (KCa) is one of the 10 most common cancers in the United States (U.S.) with 90% being attributed to renal cell carcinoma (RCC). 1 Risk factors of RCC include advanced age, a family history of KCa, smoking, hypertension and obesity. 2 Increasing evidence suggests that excess body weight defined as body mass index (BMI) ≥ 25.0 kg/m2 plays an important role in the initiation and progression of various cancers, including RCC.3,4 Speculated mechanisms through which larger body size increases the risk of RCC include chronic tissue hypoxia and dysregulated inflammatory response. 5 These processes are known to both initiate and promote carcinogenesis, which would suggest that a higher BMI should be an adverse prognostic factor. However, many studies have reported that overweight and obese patients experienced significantly longer survival compared to normal weight patients.6,7 This phenomenon is referred to as the “obesity paradox.”8-10
Several hypotheses have been proposed to explain the obesity paradox.11-13 Many patients lose weight before diagnosis and treatment due to RCC-related conditions, and patients with aggressive type of tumor may lose considerable amount of weight (reverse causation). 14 Collider stratification bias and confounding may also explain the protective effect of higher BMI. Patients with lower BMI may have an unmeasured risk factor associated with disease aggressiveness and poor survival. It is also possible that patients with low BMI have a different and more aggressive type of RCC compared to obese patients (disease heterogeneity). 8 Finally, BMI is a poor proxy of adiposity, particularly in patients from racial and ethnic minority backgrounds.13,15,16
Various factors cause obesity, and some obesity-related factors may also influence RCC aggressiveness and outcomes. Obesity is often more prevalent in neighborhoods with high socioeconomic challenges or social vulnerability due to factors, such as food desert where people have limited access to healthy food or a safe place for physical exercise. 17 Patients from minoritized racial and ethnic groups often live in neighborhoods with high socioeconomic challenges, and patients from low socioeconomic backgrounds may have increased risk of poor cancer outcomes (grade or advanced-stage cancers), which could be influenced by both their limited access to healthcare and the high prevalence of obesity. 18 The impacts of living in disadvantaged neighborhoods are especially strong when it comes to delays in RCC surgery, 19 and neighborhood socioeconomic factors modify associations between obesity and perioperative surgical outcomes. 20 In addition to socioeconomic challenges and race and ethnicity, other factors, such as age and smoking that are closely related to obesity, may also influence cancer outcomes. Age contributes to obesity as metabolic rates decline and hormonal changes promote fat accumulation over time. 21 Smoking is linked to obesity through its effects on appetite, metabolism, and post-cessation weight gain 22 and is associated with RCC stage and survival.23,24 However, previous studies on obesity and RCC in the U.S. have rarely utilized measurements of neighborhood socioeconomic characteristics or did not examine modifying effects of obesity-related factors on RCC pathological characteristics including diverse patients.
To better understand the obesity paradox in RCC, this study first examined factors associated with obesity in RCC patients. Then, we examined the associations between BMI and RCC pathological characteristics (grade and stage) and how these associations vary based on obesity-related factors, such as neighborhood social vulnerability, race and ethnicity, age, and smoking status. Our study leveraged data from 2 academic institutions, Roswell Park Comprehensive Cancer Center (Roswell Park) and University of Arizona Baner-University Medical Center Tucson (BUMCT), comprehensive cancer centers in 2 different states. We included data from these 2 sites with very different patient demographic and clinical characteristics and healthcare settings to enhance the generalizability and robustness of our findings by replicating them in 2 independent datasets.
Materials and Methods
Materials
Our study is a cross-sectional analysis involving RCC patients who had nephrectomy for treatment of RCC. Roswell Park data includes patients who were treated between 2004 and 2022 and had surgical treatment, including partial and radical nephrectomy, simple or total nephrectomy, and nephroureterectomy at Roswell Park as well as other facilities. Patients at BUMCT had a partial or radical nephrectomy at BUMCT between 2010 and 2022. At Roswell Park, patients’ demographic information (age at surgery, gender, and race and ethnicity), zip code, insurance coverage, pathology (histological subtype, stage, grade at diagnosis), and treatment information was obtained from Roswell Park Cancer Registry. We obtained weight, height, medical history, and detailed treatment information from electronic medical records. Unintended weight loss information was extracted from urologists’ notes. At BUMCT, electronic medical records were retrospectively reviewed to extract all the data as described previously.20,25 The zip code of patient’s residents was used to link Social Vulnerability Index (SVI) and Rural-Urban Commuting Area (RUCA) codes. This study included adult patients (≥18 years old at diagnosis) with a renal cell carcinoma primary tumor living in the state of New York or Arizona. After removing patients from other states and without BMI, SVI, pathological grade and stage data, there were 1949 patients, 1526 at Roswell Park and 423 at BUMCT. This study was approved by the Institutional Review Board at both sites, and the reporting of this study confirms to the STROBE guidelines. 26
This study evaluated the associations of obesity with 2 outcomes: (1) high grade RCC (grade 1 and 2 vs grade 3 and 4) and (2) advanced stage RCC (Stage I and II vs Stage III and IV). BMI was categorized into 4 groups: <25.0 kg/m2 (normal/underweight), 25.0-29.9 kg/m2 (overweight), 30.0-34.9 kg/m2 (obesity class I), and ≥35.0 kg/m2 (obesity class II/III), based on the World Health Organization (WHO) criteria. Because there were only 6 patients who were underweight (5 in Roswell Park and 1 in BUMCT), these patients were grouped together with normal weight patients. SVI was used to measure neighborhood-level socioeconomic challenges. 27 SVI scores range from 0 (less vulnerable) to 1 (most vulnerable) with increasing social and economic challenges in the neighborhoods. The SVI has 4 major themes within: (1) socioeconomic status, (2) household composition and disability, (3) minority status and language, and (4) housing and transportation. We have categorized SVI into 4 groups as<25, 25-50, 50-75, and >75. RUCA codes, which range from 1 (metropolitan) to 10 (isolated rural), were categorized into (1) metropolitan/urban (1-3), (2) large rural (4-6), and (3) small/isolated rural areas (7-10).
Statistical Analysis
RCC patients were stratified by study datasets and characterized using proportions for categorical variables and median with interquartile range (IQR) for continuous variables. Differences between datasets were tested using the chi-square test. The relationships between BMI and RCC pathological characteristics were assessed through three-stage analyses for each dataset. First, multivariable logistic regression was performed to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for assessment of BMI-related factors. The final model for each dataset was built by including age, sex, race and ethnicity, SVI, and variables that were significantly associated with obesity in unadjusted models (P < 0.10 in any category). Then, multivariable logistic regression models were used to test associations of BMI with pathological characteristics (high grade and advanced stage RCC) adjusting for potential confounders including age, sex, race and ethnicity, SVI, and other variables that were associated with outcome variables in unadjusted models (Model 1 for both sites). For analysis of Roswell Park data, weight loss variable was added to variables included in Model 1 to assess the influence of unintentional weight loss on the relationship between BMI and pathological characteristics (Model 2). BMI was modeled as a continuous variable and separately as categorical variables. We report BMI as a categorical variable because the relationship between BMI and RCC pathological characteristic outcomes was not linear. Sensitivity analyses were performed after excluding patients with a prior diagnosis of cancer and/or unintentional weight loss in Roswell Park. Finally, stratified analysis was performed to test effect modifications based on SVI categories (<50 and ≥50), for major race and ethnic groups: Non-Hispanic White (NHW) and Non-Hispanic Black (NHB) patients in the Roswell Park dataset, and NHW and Hispanic patients in the BUMCT dataset, age groups (≤60 years and >60 years), and smoking status (have smoked and never smoked). Statistical analysis was performed separately for 2 datasets because of differences in healthcare settings, data collection, and patient backgrounds resulting in very different demographic and clinical characteristics of patients who were treated at 2 sites and included in this study. Although the study approach was slightly different in 2 sites, we also aimed to validate the findings in 2 independent datasets.
Results
Characteristics of Patients
Characteristics of RCC Patients at Roswell Park and BUMCT

aP-values from Chi-square test. NA when Chi-square test was not performed because data was missing in BUMCT dataset or differences in data collection methods resulted in missing data in a category.
Factors Associated With Obesity
BMI was higher in patients from neighborhoods with higher SVI compared with patients from low SVI neighborhoods in both the datasets (Figure 1, Table S1). We performed multivariable logistic regression analyses to identify factors associated with obesity (Table S2). In both datasets, older age was generally associated with a reduced likelihood of obesity. Specifically, at Roswell Park, patients aged 70 and above had lower odds of obesity (OR 0.64, 95% CI 0.41-1.02) compared with those aged <50 years, while patients aged 50-59 years were associated with a higher likelihood of obesity (OR 1.53, 95% CI 1.04-2.24). In BUMCT, only patients aged 60-69 had a significant reduction in obesity odds compared with younger patients (OR 0.46, 95% CI 0.25-0.84). In Roswell Park, patients with a history of unintentional weight loss had significantly reduced odds of obesity (OR 0.30, 95% CI 0.20-0.45), and patients with non-clear cell subtypes were less likely obese. In BUMCT, American Indian patients had more than 3-fold increased odds of obesity compared with NHW patients, and former smokers had a 1.7-fold increase in odds of obesity compared with patients who never smoked. Increasing BMI with overall SVI in Rosell Park (A) and BUMCT (B) patients.
Obesity and High Grade and Advanced Stage RCC
Multivariable Logistic Regression Analysis Showing Associations Between BMI and Diagnosis With High Grade RCC
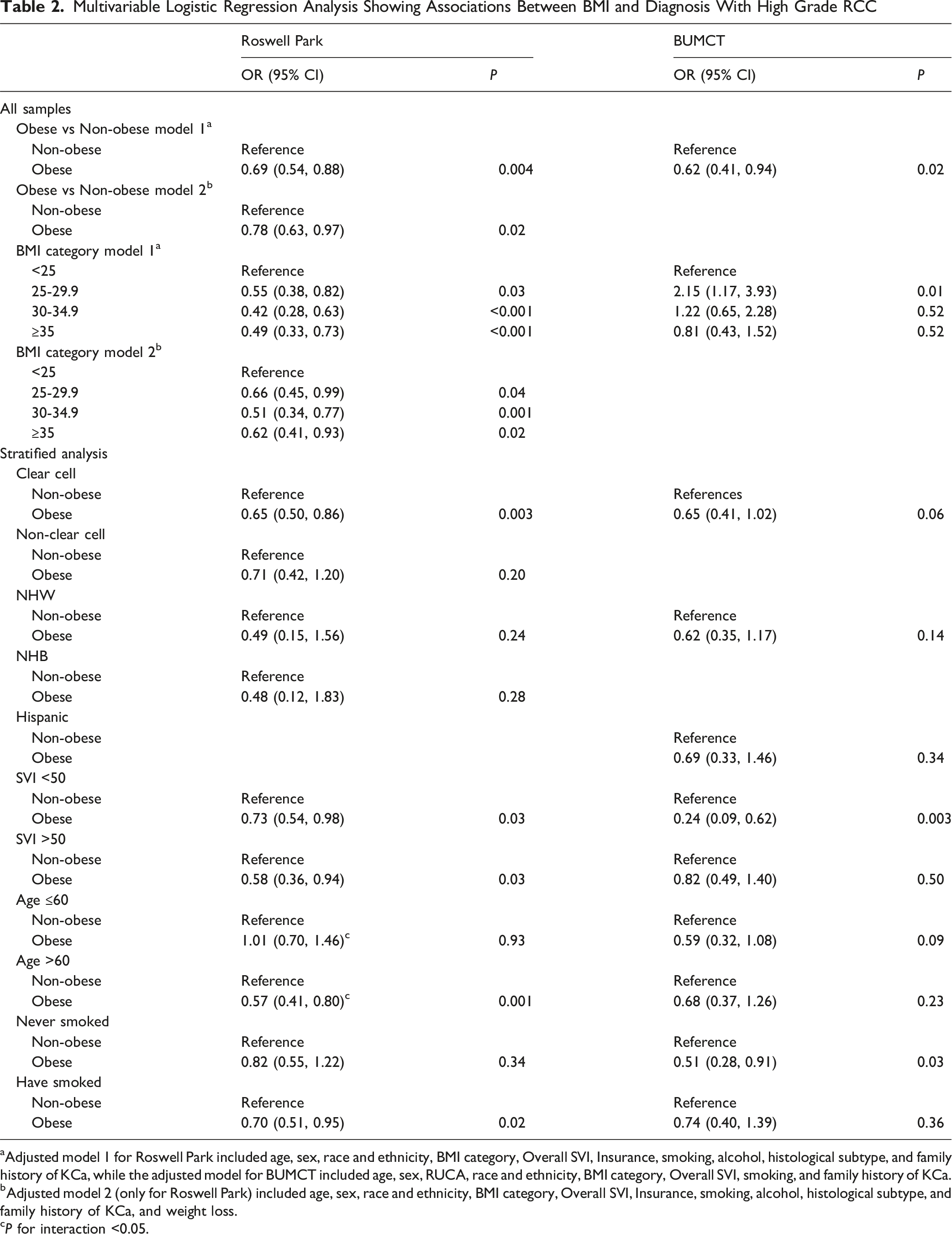
aAdjusted model 1 for Roswell Park included age, sex, race and ethnicity, BMI category, Overall SVI, Insurance, smoking, alcohol, histological subtype, and family history of KCa, while the adjusted model for BUMCT included age, sex, RUCA, race and ethnicity, BMI category, Overall SVI, smoking, and family history of KCa.
bAdjusted model 2 (only for Roswell Park) included age, sex, race and ethnicity, BMI category, Overall SVI, Insurance, smoking, alcohol, histological subtype, and family history of KCa, and weight loss.
cP for interaction <0.05.
Multivariable Logistic Regression Analysis Showing Associations Between BMI and Diagnosis With Advanced-Stage RCC

aAdjusted model 1 for Roswell Park included Age, Sex, race and ethnicity, BMI category, Overall SVI, Hypertension, histology, laterality, while adjusted model for BUMCT included age, sex, race and ethnicity, BMI category, Overall, SVI, histological subtype, and insurance.
bAdjusted model 2 (only for Roswell Park) includes: age, sex, race and ethnicity, BMI category, Overall SVI, hypertension, histological subtype, laterality, and weight loss.
cP for interaction <0.10.
Sensitivity and Stratified Analysis
We also assessed the robustness of associations after excluding patients with a prior diagnosis of cancer and/or unintentional weight loss in Roswell Park (Table S5). The associations between BMI categories and RCC pathological characteristics remained largely consistent. In analysis stratified by histologic subtype, obesity in patients with clear cell RCC had lower odds of high grade in a similar strength in both datasets (OR 0.65, 95% CI 0.50-0.86 in Roswell Park and OR 0.65, 95% CI 0.41-1.02 in BUMCT). The association in patients with non-clear cell subtypes was similar in Roswell Park. We also explored heterogeneous associations between BMI and RCC pathological characteristics based on potential factors associated with obesity and RCC grade and stage. In the stratified analysis for Roswell Park dataset, older age and smoking showed a modifying effect on the association between obesity and high grade, with significantly reduced odds for older age group (OR 0.57, 95% CI 0.41-0.80) and patients who have ever smoked (OR 0.70, 95% CI 0.51-0.95), but not for younger age group and patients who never smoked. The interaction was statistically significant for age (PInteraction = 0.001). For advanced stage, the modifying effect was observed based only on age in a lesser extent. In the BUMCT dataset, evidence of heterogenous association between obesity and high grade was observed for SVI and smoking status with significantly reduced odds in SVI <50 group (OR 0.24, 95% CI 0.09-0.62) and those who never smoked (OR 0.51, 95% CI 0.28-0.91). A similar pattern of association was observed for SVI in the analysis for advanced stage. Interaction was not significant in BUMCT.
Discussion
This study examined the associations of BMI and obesity with RCC pathological characteristics (high grade and advanced stage) as well as heterogeneous associations by age, smoking status, race and ethnicity, and neighborhood-level characteristics as measured by the SVI. BMI was inversely associated with high grade and advanced stage in Roswell Park, while associations in BUMCT were less consistent. The associations varied based on age, smoking status, and SVI. Specifically, in Roswell Park, obesity was associated with lower odds of high grade and advanced stage among older patients (>60 years) and lower odds of high grade in current and past smokers. In BUMCT, obesity was associated with lower odds of high grade and advanced stage in patients from low SVI (<50) neighborhoods and lower odds of high grade in non-smokers.
Our overall findings on the associations between BMI and RCC pathological characteristics align with the obesity paradox observed in prior research, which suggests that higher BMI may provide survival benefits in RCC patients. 11 This study evaluated pathological grade and stage, not survival, to assess whether BMI and associated clinical factors could be utilized to understand their impact on the pathological characteristics. By focusing on high grade and advanced stage tumors, we aimed to explore how BMI influences disease severity, given its established role in RCC progression and its potential implications for clinical outcomes. 28 This study found that higher BMI was associated with low grade and early stage at the time of diagnosis. Two sites showed different patterns of association between BMI and RCC pathology, but both sites consistently showed significantly reduced odds high grade in obese patients which is consistent with obesity paradox and the hypothesis suggesting that obese patients have less aggressive tumor. 8 Roswell Park had more patients grade 4 and stage IV tumor compared with BUMCT. This difference along with differences in demographic and behavioral characteristics may have caused different patterns of associations in 2 sites. However, prospective cohort studies have challenged the obesity paradox by showing that obesity based on BMI measured before RCC diagnosis and pronged exposure to excess weight prior to diagnosis are positively associated with RCC specific mortality.12,29 Another study found that higher BMI was also associated pathological upstaging. 30 In the current study, overweight category was associated with diagnosis with high grade and advanced stage RCC at BUMCT. In our previous study, we also showed that being overweight before diagnosis increased risk of diagnosis of aggressive and fetal RCC. 4 Accordingly, there is ongoing discrepancy in the literature regarding the advantageous vs disadvantageous prognostic impact of BMI in RCC patients.4,6,31
Discordant findings regarding the prognostic impact of BMI in RCC patients may relate to limitations in BMI measurement. In particular, the use of a single measure of weight (or BMI) at the time of diagnosis or surgery to understand disease aggressiveness and trajectories is potentially problematic. First, BMI does not measure adiposity accurately across racial and ethnic groups and are not appropriate for clinical measure. 32 Our study did not incorporate body composition measures, such as visceral or subcutaneous fat, that can further refine these associations.33,34 Second, understanding weight history is becoming increasingly important for risk stratification and clinical management of obesity related health conditions. 35 In the Roswell Park data analysis, unintentional weight loss was associated with high grade and advanced stage, and it appears to attenuate the association between BMI and RCC pathological characteristics, supporting the reverse causation hypothesis. Unintentional weight loss prior to RCC diagnosis often reflects an underlying tumor that is large and locally advanced enough to be symptomatic, reducing appetite and compromising overall performance status, the latter of which independently predicts relapse after nephrectomy.14,36,37 Consistent with this clinical observation, previous studies have highlighted that preoperative weight loss significantly affects survival outcomes, particularly in patients with a BMI < 30 kg/m2 compared to those with a BMI ≥ 30 kg/m2.38-40 Third, normal BMI group may represent heterogenous group of patients, which include patients who have maintained healthy weight throughout their lives, patients who lost weight through improving physical activities and healthier diet, and patients how experienced unintentional weight loss due to RCC, other disease conditions, or aging process. Future research of the obesity paradox in RCC should aim to account for the intentionality of weight changes and assess body composition to better understand the impact of adiposity in RCC progression, while exploring the biological mechanisms underlying the obesity paradox.
Given various factors influencing both obesity and RCC aggressiveness, we investigated whether obesity-related factors modify the associations between BMI and RCC pathological characteristics, and we found differences in the associations by smoking status, SVI, and age. Roswell Park and BUMCT data also exhibited differences in the pattern of heterogenous associations by these obesity-related factors. The different patterns of associations based on age, smoking status, and SVI in Roswell Park and BUMCT might be explained by population composition, data collection, healthcare access, behavioral factors, and underlying comorbid conditions (eg, hypertension and diabetes) and biological mechanisms. The differences in diagnosis pattern and/or body composition changes due to aging or disease process between age groups may explain the heterogeneous associations between obesity and RCC pathology by age groups in predominantly NHW patients from Roswell Park. Many younger patients regardless of obesity status may have had incidental findings of a renal mass or less aggressive RCC. On the other hand, some older patients, particularly those who are not obese, have experienced age-related body composition changes, including decreased lean muscle, which is linked to high grade RCC.21,33
We also found differences in association between obesity and grade by smoking status, but the patterns of associations were different in the 2 datasets. Obesity was significantly associated with reduced odds of high grade in current and former smokers in Roswell Park, but the association was significant in patients who never smoked in BUMCT. Smoking could have different effects on tumors by weight and had a greater negative impact in non-obese patients, but the reason for heterogenous association is uncertain. However, the difference in demography and smoking behavior may explain the different patterns that we observed in 2 study sites. Smoking prevalence is generally higher in NHW individuals, who made up a larger portion in Roswell Park. Conversely in BUMCT, Hispanic patients are well represented. Hispanic patients are often diagnosed at a younger age,25,41 and Hispanic population have lower smoking and higher obesity rates.42-44 The association between obesity and high grade was significant for ccRCC patients, not non-ccRCC patients in Roswell Park, but ORs were similar in both groups (only 6% differences). It is likely that sample size for non-ccRCC was too small to show statistical significance. Future studies are necessary to understand the influence of smoking on the relationship between obesity and RCC aggressiveness. Future studies should also investigate the obesity paradox separately within racial and ethnic groups, as the relationship between BMI and RCC outcomes may vary across populations due to behavioral, health access, and underlying genetic differences.
Moreover, unlike our study, prior research has lacked the integration of neighborhood-level characteristics that are potentially related to obesity and RCC pathological and oncologic outcomes. This study found differences in association by SVI in BUMCT, but not in Roswell Park. This difference may reflect neighborhood level differences in healthcare availability or environmental exposures as well as potential confounding factors that were not captured in this study.45,46 Additionally, variations in other behavioral, cultural, and socio-political factors and data collection and reporting processes between the 2 institutions may have contributed to these discrepancies. These findings highlight the complex interplay between obesity, patient demographics, and RCC pathological characteristics.
There are limitations to this study. First, the Roswell Park dataset consists predominantly of NHW patients, limiting the generalizability of our findings to more racially and ethnically diverse populations. To increase the diversity of patients in the study, we included BUMCT. Although our study incorporates data from 2 distinct sources, the number of patients from underrepresented racial and ethnic groups, such as American Indian populations, was small, preventing meaningful subgroup analysis for these high-risk populations. Secondly, there were only 6 patients who were underweight (5 in Roswell Park and 1 in BUMCT), and we were not able to investigate if the underweight patients were more likely to have high grade or advanced stage RCC. Additionally, the BUMCT data lacked recurrence and survival information, so our analysis focused on pathological characteristics rather than survival. The cross-sectional design and retrospective nature of data collection also restricted our ability to establish causality. We utilized SVI to account for socioeconomic disparities. However, individual-level socioeconomic data was not available and may yield different results. Moreover, information on unintentional weight loss may not be consistently recorded in the clinicians’ notes. Urologists may have focused on recording unintentional weight loss in patients with symptoms or more advanced RCC resulting in bias in the dataset. Finally, differences in patients treated and included in the study were very different between 2 sites. Roswell Park may include complex cases who were referred to oncology care after surgical treatment elsewhere, while BUMCT patients were treated by urologists. The differences in data collection (use of cancer registry at Roswell Park and manual chart review at BUMCT) also made harmonization of data from 2 sites difficult, requiring separate analysis for each dataset. Future studies should address these limitations by including more diverse populations, using prospective study designs with pre- and post-diagnostic assessment of weight and adiposity changes, and including additional individual-level socioeconomic and clinical data to enhance the robustness of findings, while further assessing relationships with survival outcomes.
In conclusion, this study evaluated the association of BMI and obesity with high grade and advanced stage RCC. Neighborhood level factors, age and behavioral factors such as smoking appear to impact the relationship between obesity and pathological outcome of RCC. Further exploration is necessary especially for people in vulnerable communities and underrepresented racial and ethnic groups (Hispanic and American Indian populations) who have a heavy burden of RCC but are underrepresented in clinical and epidemiologic studies.
Supplemental Material
Supplemental Material - A Cross-Sectional Study Assessing Association of Renal Cell Carcinoma Pathological Grade and Stage With Body Mass Index and Obesity Related Factors
Supplemental Material for A Cross-Sectional Study Assessing Association of Renal Cell Carcinoma Pathological Grade and Stage With Body Mass Index and Obesity Related Factors by Sakshi Shrivastava, Eric C. Kauffman, Patrick Wightman, Marilyn L. Kwan, Li Tang, Marvin E. Langston, Zhengyi Deng, Benjamin R. Lee, Juan Chipollini, Ken Batai in Cancer Control
Footnotes
Acknowledgements
Clinical Data Delivery and Honest Broker services for Roswell Park data were provided by the Biomedical Research Informatics Shared Resource, which is funded by NCI P30CA16056 and is a Roswell Park Comprehensive Cancer Center Support Grant shared resource. We also thank former students and residents at the University of Arizona who contributed to data collection for BUMCT data.
Ethical Considerations
The protocol was approved by the Institutional Review Boards at Roswell Park Comprehensive Cancer Center (STUDY00002071) and the University of Arizona (Protocol Number 191228839).
Author Contributions
Conceptualization, K. B.; methodology, S.S. and K.B.; formal analysis, S.S.; investigation, P.W.; resources, E.C.K., B.R.L and J.C.; writing—original draft preparation, S.S. and K.B.; writing—review and editing, E.C.K., P.W., M.L.K., L.T., M.E.L, Z.D., B.R.L, and J.C.; visualization, S.S. and K.B. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly supported by Roswell Park Comprehensive Cancer Center Support Grant (P30CA16056) from the US National Institute of Health and Kidney Cancer Research Program Idea Development Award (W81XWH2110811) from the US Army Medical Research and Development Command.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this project is available upon request. Fully de-identified data may be shared after establishing data use agreements with each institution.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.