
Abstract
Background:
Weber B (supination external rotation) ankle fractures with complete deltoid ligament rupture (SER4b) are typically considered unstable and treated with plate fixation of the fibula. Recent studies have suggested a significant ankle-stabilizing role of the deep posterior tibiotalar ligament (dPTTL), which questions current practice. To our knowledge, there are few studies on the biomechanical effects of plate fixation and none on dPTTL repair. Therefore, this study aims to evaluate the effects of fibular plate fixation and dPTTL repair on ankle stability in a Weber B fracture model with complete deltoid ligament sectioning.
Methods:
We robotically tested 15 cadaveric ankle specimens in 5 states: native joint, SER4b injury models, SER4b injury models with plate fixation of the fibula, SER4b injury models with dPTTL repair, and SER4b injury models with combined plate fixation and dPTTL repair. The robot measured ankle stability in lateral translation, valgus, and internal and external rotation. Talar shift and talar tilt were measured on mortise view radiographs. The primary outcome was differences in talar shift in neutral ankle position.
Results:
When comparing SER4b injury models with plate fixation to native ankles, we found a mean difference in talar shift of 1.18 mm (95% CI 0.88-1.48, P ≤ .001), talar tilt of 14.47 degrees (95% CI 12.90-16.05, P ≤ .001), and external rotation of 11.44 degrees (95% CI 9.00-13.87, P ≤ .001). When comparing SER4b injury models with combined plate fixation and dPTTL repair to native ankles, we found a mean difference in talar shift of 0.23 mm (95% CI −0.07 to 0.54, P = .132), talar tilt of 1.65 degrees (95% CI 0.07-3.22, P = .040), and external rotation of 5.26 degrees (95% CI 2.82-7.70, P ≤ .001).
Conclusion:
This study's main finding was that plate fixation of the fibula alone did not considerably enhance ankle stability in SER4b injury models. However, ankle stability was substantially improved when plate fixation and dPTTL repair were combined.
Clinical Relevance:
Our study showed that dPTTL repair, in addition to plate fixation, improved ankle stability in Weber B SER4b fracture models. This information should be considered in future clinical research and treatment strategies for these fractures.
This is a visual representation of the abstract.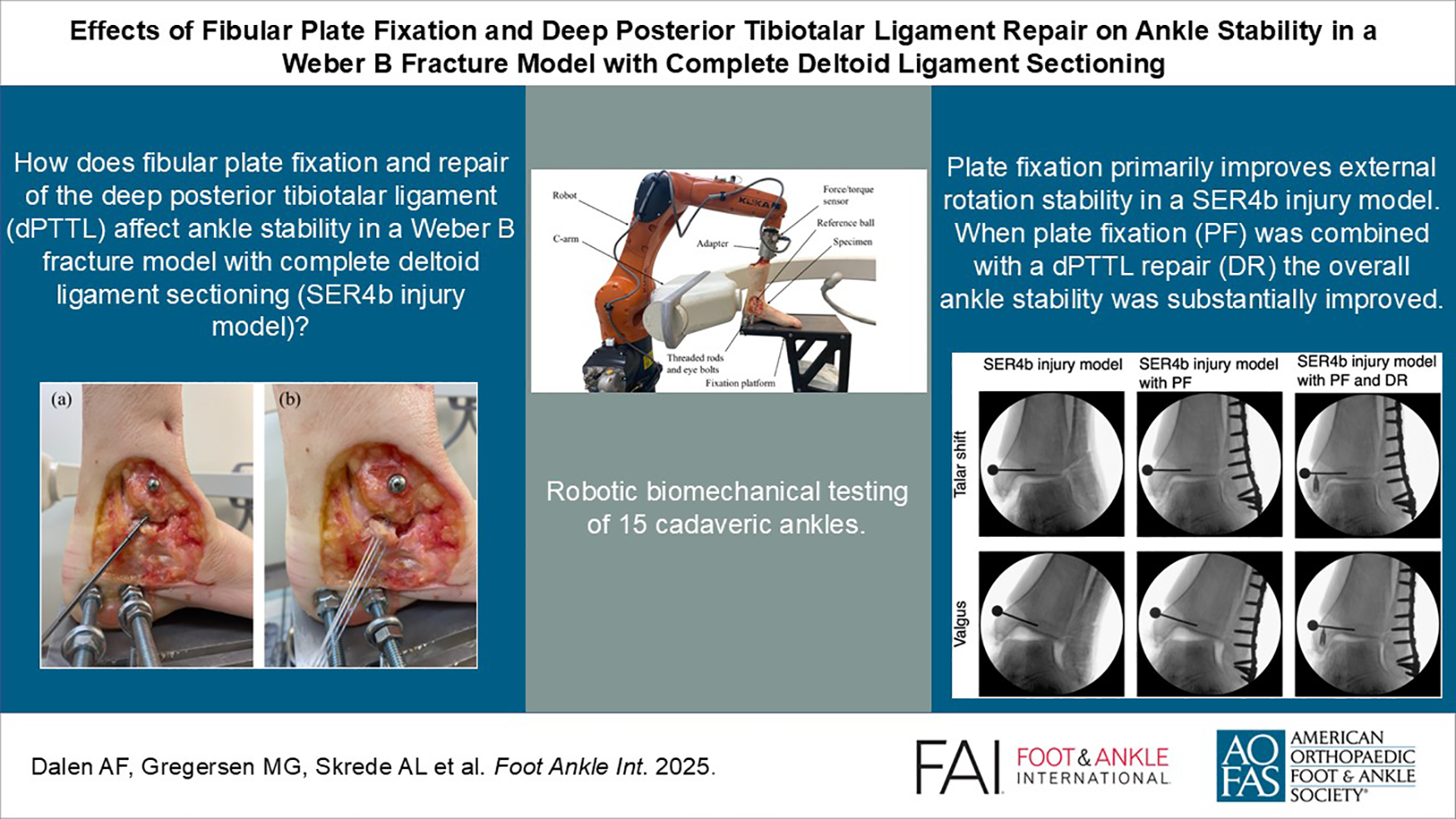
Introduction
Recent classifications of Weber B/supination external rotation (SER) ankle fractures provide more precise diagnostics criteria based on the state of the deltoid ligament as intact (SER2), partially injured but with the deep posterior tibiotalar ligament (dPTTL) intact (SER4a), or completely ruptured (SER4b).4,7,8 Differentiating between partial and complete deltoid ruptures seems critical, as it may represent the watershed for when surgery is warranted.2,10 Ankle fractures with partial deltoid ruptures (SER4a) are traditionally managed surgically. However, several clinical and biomechanical studies indicate that SER4a fractures are stable enough to be treated conservatively with excellent outcomes.2,7,8,10,12 Clinical data on fractures with complete deltoid ruptures (SER4b) are limited, but biomechanical studies suggest that SER4b injuries are considerably more unstable compared with SER4a.2,10
Unstable fractures are typically treated with plate fixation of the fibula fracture. Although the condition of the deltoid ligament is pivotal in determining the need for surgery, clinical studies, including a randomized controlled trial, have not shown a clear benefit from adding deltoid ligament repair.11,14 However, as the understanding of the deltoid ligament and the mechanics of ankle fractures has advanced, it may be time to reassess the potential advantages of supplementing standard plate fixation with dPTTL repair in selected patient groups. We have previously demonstrated that plate fixation may be redundant in SER4a models. 5 This study addresses stabilizing surgical treatment options for SER4b models.
This study aimed to explore the following questions:
What is the stabilizing effect of plate fixation in an SER4b injury model
What is the additional effect of combining dPTTL repair and plate fixation
What is the stabilizing effect of isolated dPTTL repair in an SER4b injury model
Materials and Methods
Ethical approval for the study was given by the Regional Committee for Medical and Health Research Ethics (ref. 178067). All donors had provided consent for their bodies to be used in research. The biomechanical tests were conducted at Ålesund Biomechanics Lab, Ålesund, Norway. The methodologies for specimen preparation, testing, and statistical analysis have been thoroughly described in prior studies.2,5
Specimen Preparation
We used 18 fresh-frozen human cadaveric foot and ankle specimens (Science Care, Phoenix, AZ) that had no known medical history or visible signs of previous injury, surgery, or osteoarthritis in the ankle/hindfoot. The specimens were stored at −23 °C and thawed for minimum 12 hours before preparation and testing.
The medial side of the ankle was carefully dissected to expose the deltoid ligament, with each individual band identified and marked for subsequent sectioning.
The tibial shaft was cut 22 cm proximal to the distal tip of the medial malleolus. A metal cylinder was molded to the proximal tibia using a 3-component casting resin (Rencast FC 52/53 Isocyanate, Polyol FC 53, Filler DT 082; Huntsman Corp, The Woodlands, TX). The calcaneus was exposed from the lateral aspect and reinforced with casting resin. Two threaded rods (M8, stainless steel) were drilled through the calcaneus from medial to lateral. An 8-mm radiographic reference ball was attached to the medial malleolus.
Test Setup
The specimens were fixed to a floor-mounted platform, using eye bolts that pulled the threaded rods and the calcaneus toward the platform plate. The cylinder on the proximal tibia was attached to a custom-made adapter distal on the robot arm (Figure 1).
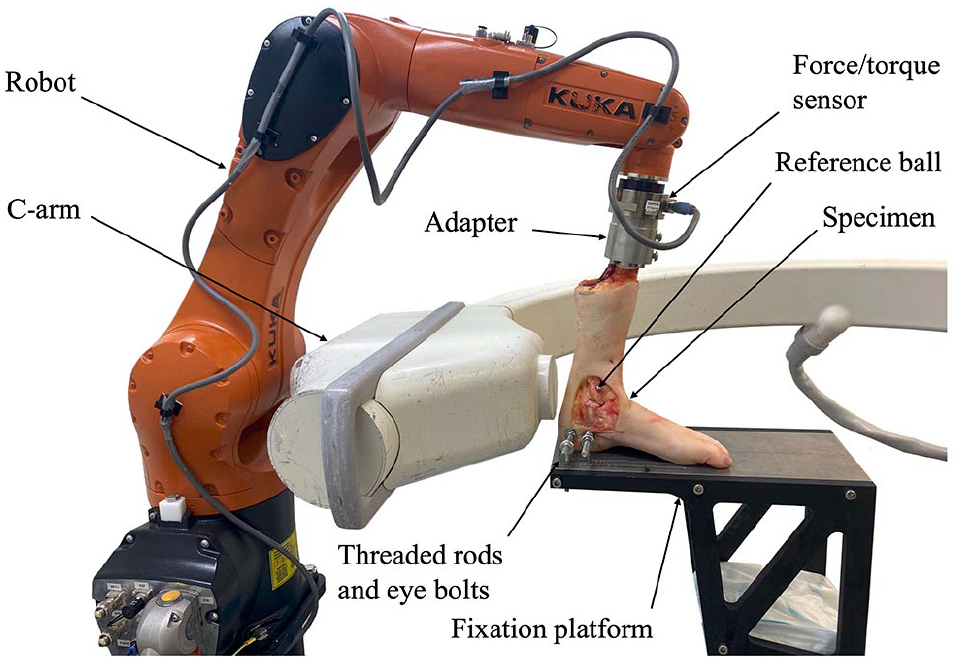
The figure shows an overview of the experimental setup for ankle stability testing.
A force-guided industrial robot (KR6 R900 Sixx, KUKA, Germany) was used for the biomechanical testing. The robot was equipped with a 6–degrees of freedom force/torque sensor (ATI Industrial Automation, Inc, Apex, NC). The robot has a pose repeatability of 0.03 mm (ISO 9283), and the force/torque sensor has a resolution of 1/20 N and 1/800 Nm (SI-130-10 ATI).
A C-arm (FlexiView 8800; GE Healthcare, Chicago, IL) was used to capture radiographs. The robot measured the total movement between the tibia and the calcaneus, including both the talocrural and subtalar joints. Radiographs were used to measure movement in the talocrural joint.
Biomechanical Testing Protocol
The robot moved the tibia of the specimen relative to the fixed calcaneus, guided by measurements from the force/torque sensor. Four stability tests were conducted: external rotation, internal rotation, valgus, and lateral translation. All 4 stability tests were performed in 3 different positions of the ankle joint: 10 degrees dorsiflexion, neutral position, and 20 degrees plantarflexion. All joint positions were validated using radiographs prior to testing. Internal rotation, external rotation and valgus tests were performed until 2 Nm torque was achieved. Lateral translation test was performed by linearly moving the tibia until 30 N was achieved. A constant 45-N axial force was applied to the tibia in all positions during all tests. The robot test methodology is thoroughly described in a previous study. 13
All specimens were tested sequentially as follows:
Native joint
SER4b injury models with plate fixation of the fibula
SER4b injury models with combined plate fixation and deep posterior tibiotalar ligament (dPTTL) repair
SER4b injury models with dPTTL repair
SER4b injury models
Specimen Injury Model and Surgical Procedures
The SER4b injury models were made according to the Lauge-Hansen SER classification 9 and consisted of a Weber B fracture model osteotomy of the fibula, dissection of the syndesmosis ligament (anterior and posterior tibiofibular ligaments) and a total sectioning of the medial deltoid ligament complex (both superficial and deep layer). The method of making the SER4b injury models have been thoroughly described in prior studies.2,5
Anatomic reduction and plate fixation of the fibula osteotomy was done using an EVOS lateral distal fibula 3.5 mm, 7-hole locking plate (Smith & Nephew, Watford, United Kingdom) (Figure 2). All screw holes were used in every case.

The figure shows fixation of the Weber B fibula fracture model with a 7-hole locking plate.
In the SER4b injury model, the dPTTL was sectioned proximally, close to its tibial attachment. To repair the ligament, a Twinfix Ti 3.5-mm suture anchor with 2 No. 2 Ultrabraid sutures (Smith & Nephew) was inserted centrally in the footprint of the origin of the dPTTL (Figure 3A), anatomically described as the distal center of the intercollicular groove in the medial malleolus of the tibia.1,3,6 Both sutures were sewn into the remaining distal part of the dPTTL (Figure 3B) and the ligament was tightened against the medial malleolus with slip knots and finally secured with a running suture to adapt the superficial part of the ligament.
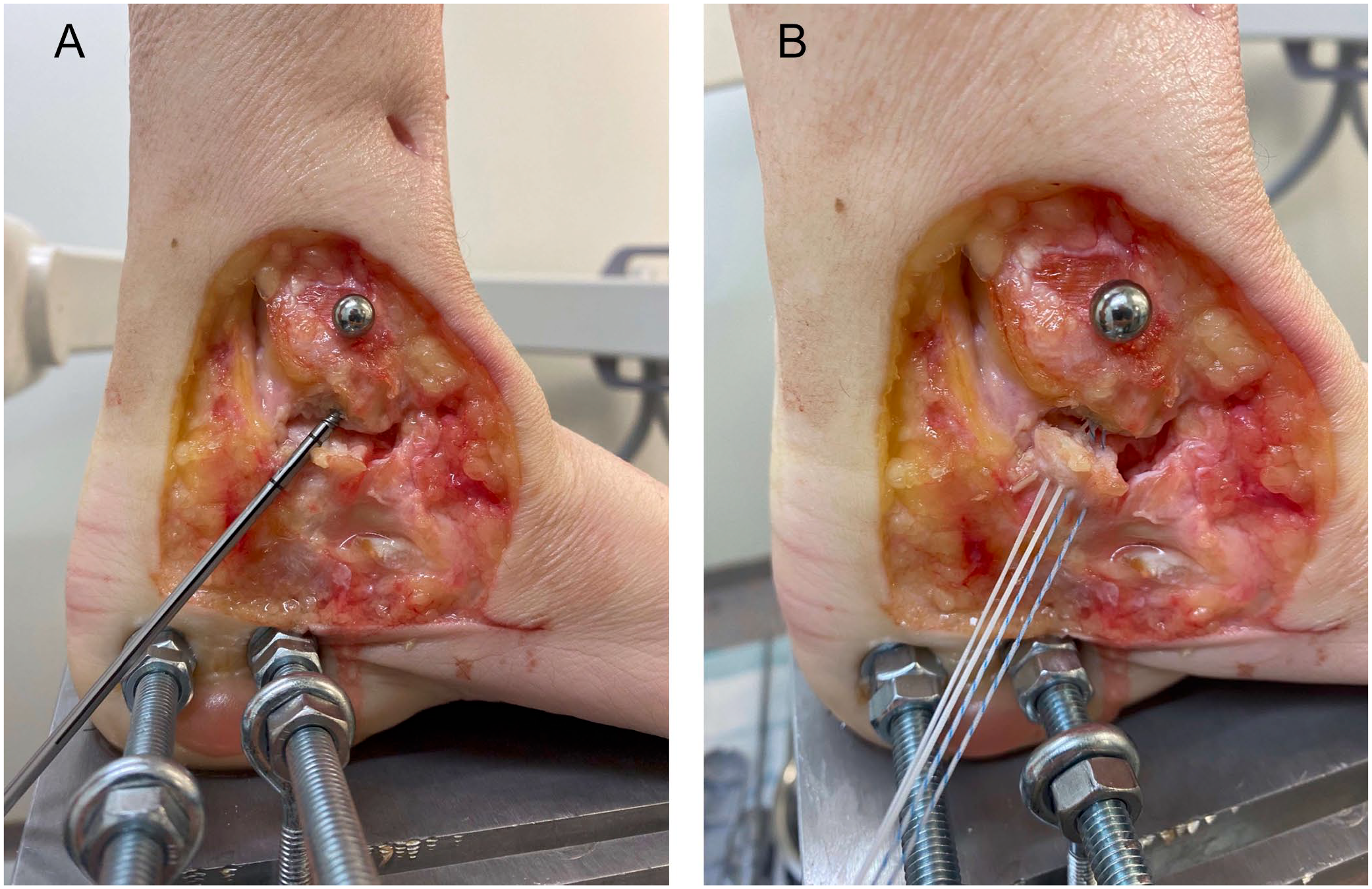
The figure shows the repair of the deep posterior tibiotalar ligament (dPTTL) with (A) the insertion of a 3.5-mm suture anchor centrally in the footprint in the medial malleolus of the tibia and (B) both sutures sewn into the remaining part of the dPTTL.
All injuries and repairs were done with the specimen securely fixed to the platform and robot, with the ankle joint in neutral position. The specimens were not detached from the robot or the fixation platform between the subsequent tests or interventions, keeping the specimen placement consistent.
Outcomes
The primary outcome of the study was the difference in radiographic talar shift for SER4b injury models with plate fixation compared to native ankles, at a neutral ankle position (Figure 4). Talar shift was quantified in millimeters as the medial clear space (MCS) on ankle mortise view radiographs. The MCS was defined as the distance between the medial border of the talus and the lateral border of the medial malleolus, measured along a line parallel to and 5.0 mm below the talar dome.
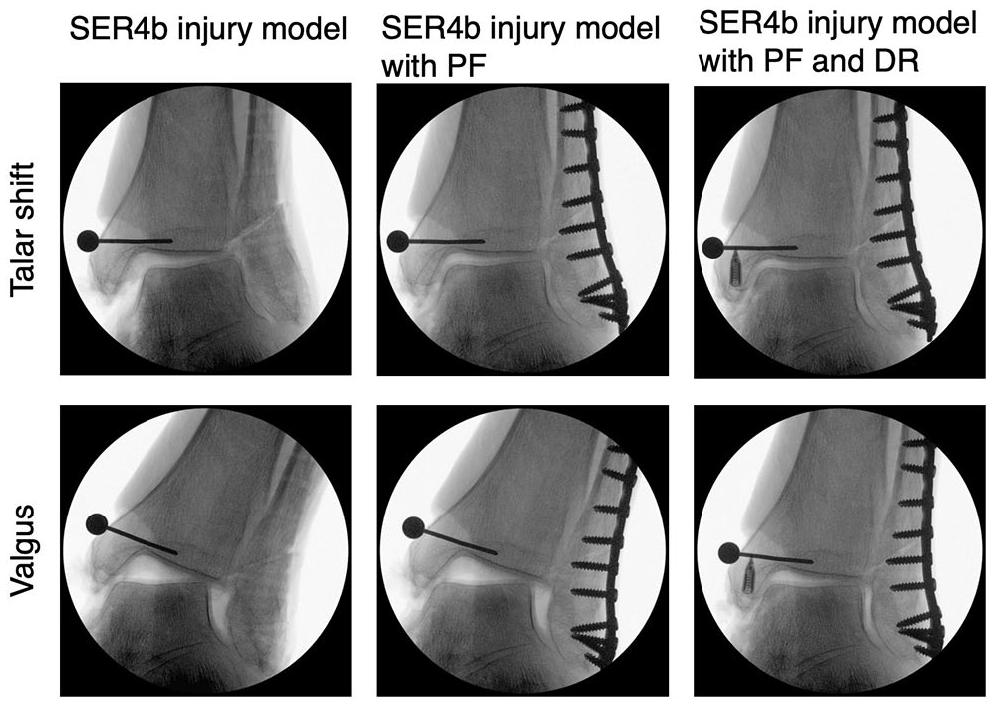
The figure shows radiographs of talar shift and valgus testing of an ankle with SER4b injury model, SER4b injury model with plate fixation of the fibula and SER4b injury model with combined plate fixation and deep posterior tibiotalar ligament repair. DR, deep posterior tibiotalar ligament repair; PF, plate fixation.
Secondary outcomes included difference in radiographic talar valgus tilt (degrees, Figure 4), robotic measurements of lateral translation (millimeters), valgus tilt (degrees), and internal/external rotation (degrees). Radiographic talar valgus tilt was measured as the angle between the distal articular surface of the tibia and the superior articular surface of the talus. 5 All radiographic measurements were performed using Sectra IDS7, version 23.2 (Sectra AB, Sweden). The robotic system was used to measure the combined motion of the ankle joint, including both the talocrural and subtalar joints. Radiographs were used to measure the isolated motion of the talocrural joint during lateral translation and valgus tests (Figure 4). All robotic and radiographic measurements were done in neutral ankle position, 10 degrees dorsiflexion, and 20 degrees plantarflexion.
Four different comparisons were made:
- SER4b injury models with plate fixation compared to native
- SER4b injury models with dPTTL repair compared to native
- SER4b injury models with combined plate fixation and dPTTL repair compared to native
- SER4b injury models with combined plate fixation and dPTTL repair compared to SER4b injury models with plate fixation.
Statistical Analysis
Continuous variables were summarized using means and corresponding SDs. Mixed models with random intercepts for study specimens were estimated and used for comparing pairwise differences in means across groups. Normality was assessed through visual inspection of distributions. No formal a priori power analysis was done as this was considered to be a descriptive pilot study. All analyses were done using Stata, version 17.0 (StataCorp, College Station, TX).
Results
Specimens
Three ankle specimens were excluded because of significant ankle osteoarthritis (n = 2) and arthrofibrosis indicating previous substantial ankle trauma (n = 1). Fifteen ankle specimens were included in the final analyses. The average age at death was 71.3 years (range 55-87 years), 7 were female (46.7%), and 7 were right ankles (46.7%).
Biomechanics
Test results of native ankles, in neutral position, showed a mean talar shift of 2.97 mm (SD 0.51), talar valgus tilt of 1.48 degrees (SD 0.87), and external rotation of 13.47 degrees (SD 4.25).
Test results of SER4b injury models, in neutral ankle position, showed a mean talar shift of 7.01 mm (SD 2.42), talar valgus tilt of 18.83 degrees (SD 3.92), and external rotation of 35.02 degrees (SD 6.01).
Test results of SER4b injury models with plate fixation, in neutral ankle position, showed a mean talar shift of 4.15 mm (SD 0.85), talar valgus tilt of 15.95 degrees (SD 4.33), and external rotation of 24.91 degrees (SD 6.44).
Test results of SER4b injury models with dPTTL repair, in neutral ankle position, showed a mean talar shift of 4.60 mm (SD 0.83), talar valgus tilt of 4.32 degrees (SD 2.30), and external rotation of 31.21 degrees (SD 7.96).
Test results for SER4b injury models with combined plate fixation and dPTTL repair, in neutral ankle position, showed a mean talar shift of 3.20 mm (SD 0.48), talar valgus tilt of 3.13 degrees (SD 1.90), and external rotation of 18.73 degrees (SD 4.79).
All stability measurements for all tested states, in neutral ankle positions, are presented in Table 1. Testing the ankles in 10 degrees dorsiflexion and 20 degrees plantarflexion showed similar results (Table S1) as in neutral ankle position.
Stability Measurements for All Tested States, in Neutral Ankle Positions (N = 15 Ankles).
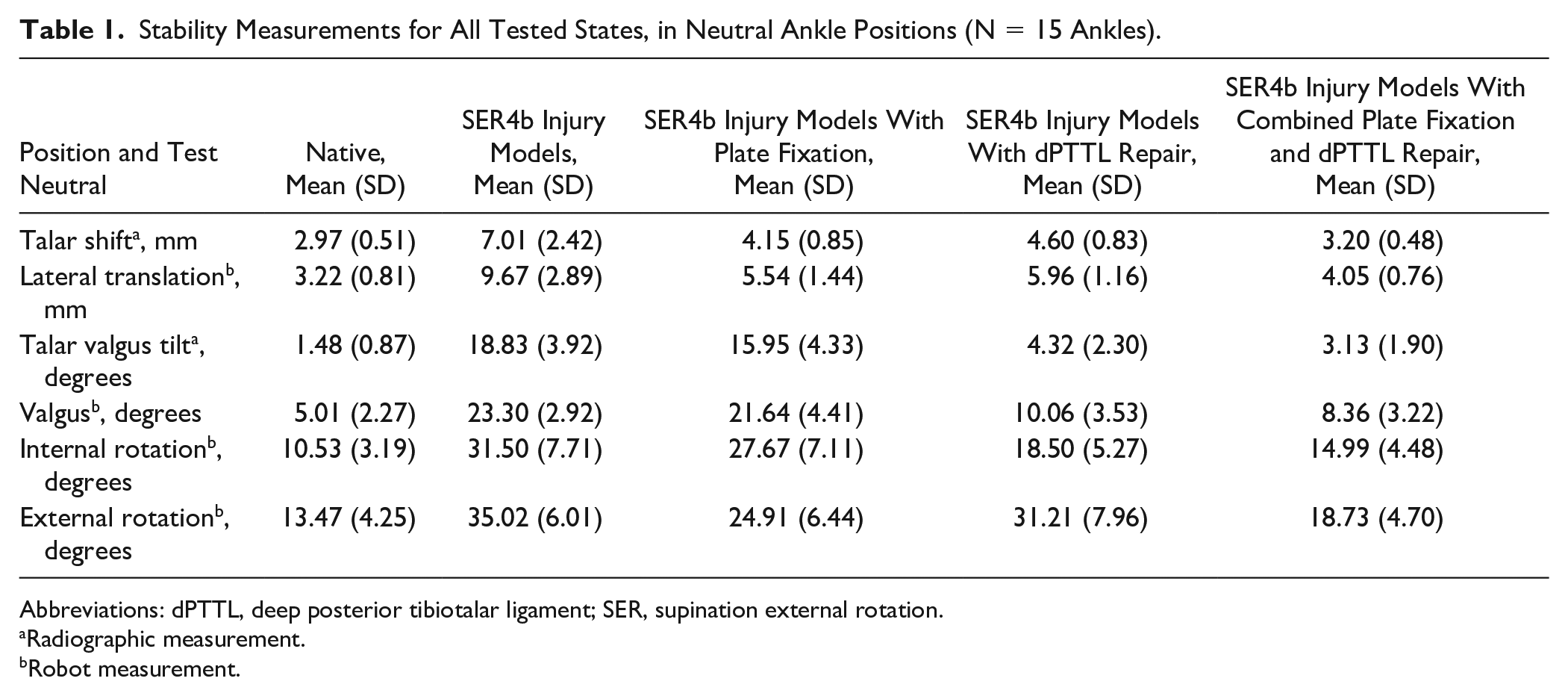
Abbreviations: dPTTL, deep posterior tibiotalar ligament; SER, supination external rotation.
Radiographic measurement.
Robot measurement.
Plate Fixation Compared With Native
When comparing SER4b injury models with plate fixation to native ankles, in neutral ankle position (Table 2), we observed a mean difference in talar shift of 1.18 mm (95% CI 0.88-1.48, P ≤ .001), talar valgus tilt of 14.47 degrees (95% CI 12.90-16.05, P ≤ .001), and external rotation of 11.44 degrees (95% CI 9.00-13.87, P ≤ .001). Similar results were also observed when testing the ankles in 10 degrees dorsiflexion and 20 degrees plantarflexion (Table S2).
Stability Differences Ankles Tested in Neutral Position Comparing SER4b Injury Models With Plate Fixation to Native (N = 15). a
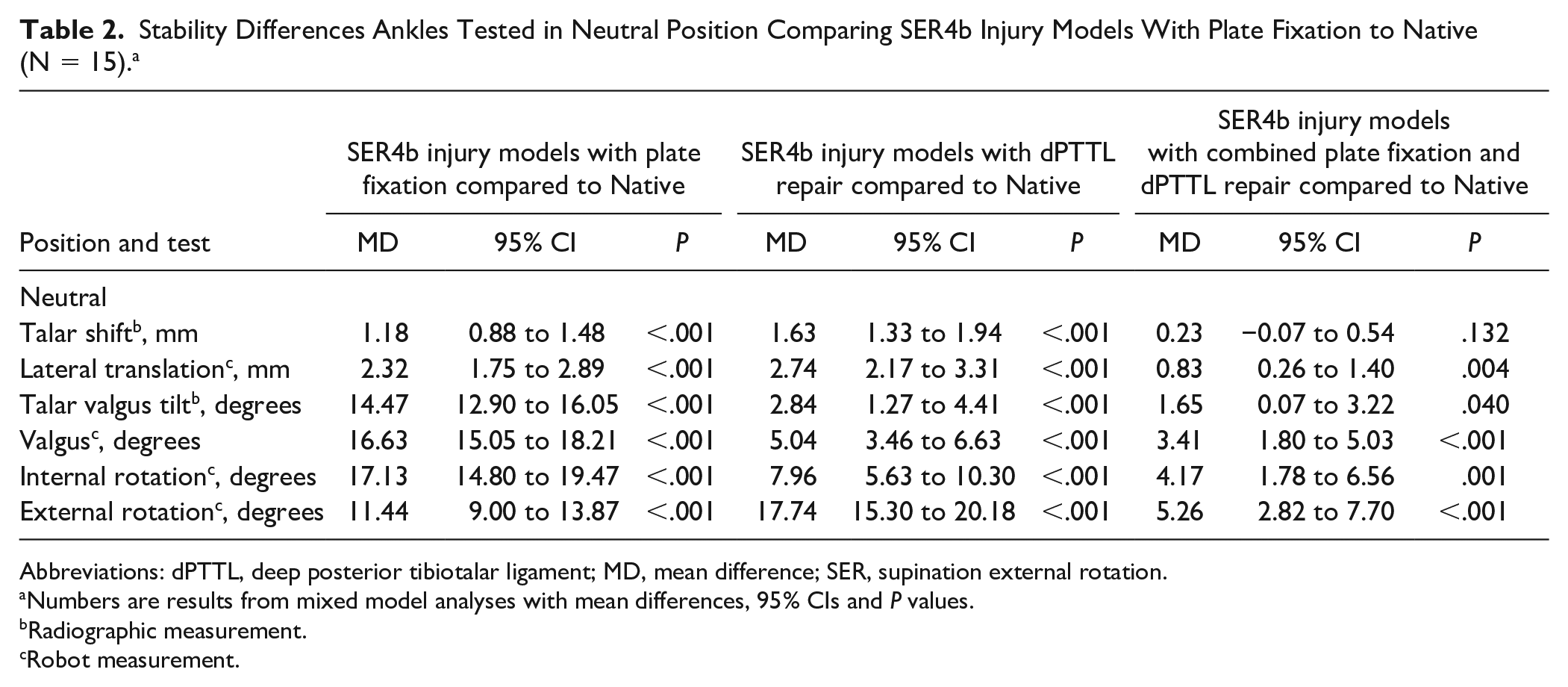
Abbreviations: dPTTL, deep posterior tibiotalar ligament; MD, mean difference; SER, supination external rotation.
Numbers are results from mixed model analyses with mean differences, 95% CIs and P values.
Radiographic measurement.
Robot measurement.
dPTTL Repair Compared to Native
When comparing SER4b injury models with dPTTL repair to native ankles, in neutral ankle position (Table 2), we observed a mean difference in talar shift of 1.63 mm (95% CI 1.33-1.94, P ≤ .001), talar valgus tilt of 2.84 degrees (95% CI 1.27-4.41, P ≤ .001) and external rotation of 17.74 degrees (95% CI 15.30-20.18, P ≤ .001). Similar results were also observed when testing the ankles in 10 degrees dorsiflexion and 20 degrees plantarflexion (Table S2).
Combined Plate Fixation and dPTTL Repair Compared to Native
When comparing SER4b injury models with combined plate fixation and dPTTL repair to native ankles, in neutral ankle position (Table 2), we observed a mean difference in talar shift of 0.23 mm (95% CI −0.07 to 0.54), P ≤ .001), talar valgus tilt of 1.65 degrees (95% CI 0.07-3.22, P ≤ .001), and external rotation of 5.26 degrees (95% CI 2.82-7.70, P ≤ .001). Similar results were also observed when testing the ankles in 10 degrees dorsiflexion and 20 degrees plantarflexion (Table S2).
Combined Plate Fixation and dPTTL Repair Compared to Plate Fixation
When comparing SER4b injury models with combined plate fixation and dPTTL repair to SER4b injury models with plate fixation, in neutral ankle position (Table 3), we observed a mean difference in talar shift of −0.95 mm (95% CI −1.22 to −0.67 mm, P ≤ .001), talar valgus tilt of −12.83 degrees (95% CI −14.87 to −10.78, P ≤ .001), and external rotation of −6.18 degrees (95% CI −7.98 to −4.37, P ≤ .001). Similar results were also observed when testing the ankles in 10 degrees dorsiflexion and 20 degrees plantarflexion (Table S3).
Stability Differences in Ankles Tested in Neutral Position Comparing SER4b Injury Models With Combined Plate Fixation and dPTTL Repair to SER4b Injury Models With Plate Fixation (N = 15). a
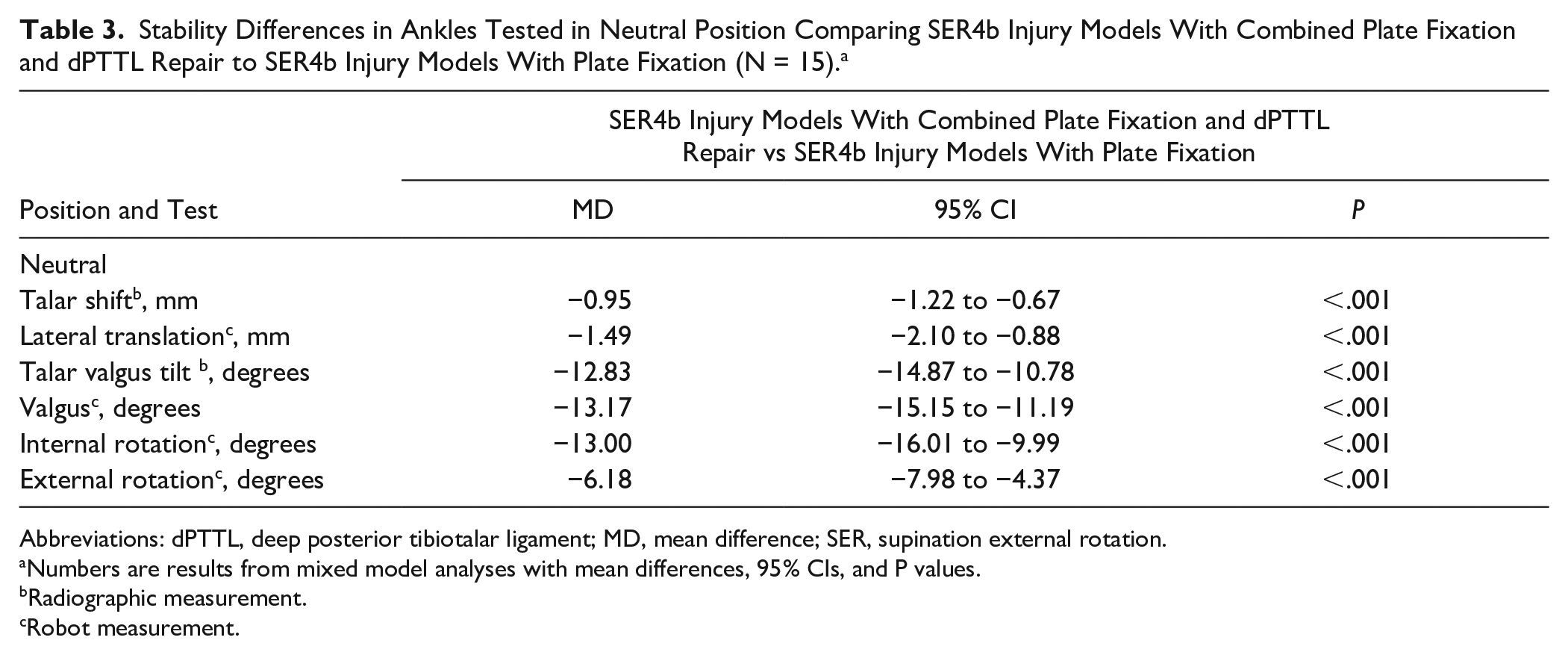
Abbreviations: dPTTL, deep posterior tibiotalar ligament; MD, mean difference; SER, supination external rotation.
Numbers are results from mixed model analyses with mean differences, 95% CIs, and P values.
Radiographic measurement.
Robot measurement.
Discussion
The primary finding of this study was that plate fixation of the fibula osteotomy alone did not considerably enhance ankle stability in SER4b injury models when tested using a robotic system on human cadaver specimens; neither did isolated dPTTL repair. However, when plate fixation was combined with dPTTL repair, ankle stability was substantially improved, with results close to those of a native ankle.
Few studies have explored stabilizing surgery in SER4b injury models. McCormack et al 10 demonstrated residual talar valgus instability after fibula plate fixation of SER4b injury models when tested with 750-N axial load in a neutral ankle position. Our results indicate that fibula plate fixation alone does not sufficiently restore overall ankle joint stability in SER4b injury models. Our experimental protocol differed from that of McCormack in that we used a much lower axial load and tested with deforming forces in several planes. However, in addition to valgus instability, our findings also demonstrated substantial differences in talar shift and internal rotation when comparing SER4b injury models with fibula plate fixation to native ankles. Specifically, internal rotation remained markedly increased after isolated fibula fixation, indicating that this method alone is insufficient to restore rotational control, although plate fixation does appear to reduce external rotation instability to some extent. Lateral shift of the talus was not substantially improved by plate fixation alone, suggesting that the deltoid ligament plays a critical role in stabilizing the ankle in the coronal plane. These differences were reduced when combining the fibula plate fixation with a dPTTL repair, further emphasizing the importance of addressing deltoid ligament integrity to achieve optimal joint stability. These findings underscore the potential need for a more comprehensive surgical approach that includes both fibula fixation and deltoid ligament repair to effectively restore normal ankle kinematics in SER4b injury models.
Distinguishing between partial (SER4a) and total (SER4b) deltoid ligament ruptures is a relatively new concept.7,8,12 Only 2 prior biomechanical studies have addressed this distinction,2,10 both showing that ankle stability is maintained in Weber B fracture models until the dPTTL is sectioned, indicating that dPTTL rupture may be the critical factor in determining ankle stability. Interestingly, our findings of acceptable stability only after combined plate fixation and dPTTL repair do not align with previous clinical studies. In these studies, a clear benefit from augmenting fracture fixation with deltoid ligament repair could not be found. 11 However, these studies on deltoid ligament repair likely included some ankle fractures with partial deltoid ligament ruptures (SER4a), which, as recent literature suggests, could be managed nonoperatively because of their inherent stability.7,8 Moreover, the surgical techniques used in those studies did not emphasize the repair of the dPTTL, now recognized as the primary stabilizer of the fractured ankle. The only available randomized controlled trial lacks detailed descriptions of the fractures involved and the specific methods of ligament repair, 14 which limits its applicability to current clinical practice.
Finally, our findings indicate that the ankle demonstrates improved stability when evaluated in a neutral position and during dorsiflexion. Based on these findings, one could hypothesize that traditional fracture fixation of the fibula may be adequate for SER4b fractures, provided that a plaster cast is used postoperatively to maintain the ankle at a 90-degree angle until the healing of medial ligament injuries is achieved, as this position could offer additional inherent stability. Nevertheless, further research is necessary to validate this hypothesis, as healing of the medial ligaments and thus the long-term effect of cast immobilization is uncertain.
Clinical Relevance
This study's findings suggest that although traditional treatment methods with fracture fixation may restore some ankle stability, they may not be sufficient for Weber B SER4b fractures, which likely have a concomitant dPTTL injury. This study implies that incorporating ligament repair could improve ankle stability for patients with unstable Weber B/SER4b ankle fractures.
Limitations
Several limitations to this study must be considered. First, whereas cadaver studies may offer insights into Weber B injury biomechanics, they cannot fully capture the complexities of these injuries in living patients. The strict control over variables such as fracture line orientation, syndesmosis ligament injury, and the extent of deltoid injury in this study enhances scientific rigor but may reduce the clinical relevance of the findings. Additionally, the SER4b injury models in this study were modeled purely as ligamentous injuries without the involvement of the posterior and medial malleolus fractures that often accompany these injuries in vivo. The findings may not be generalized to this patient population. A limitation of our study is that we only reconstructed the dPTTL and did not assess the potential effects of repairing other portions of the deltoid ligament. Therefore, we cannot determine whether additional reconstructions, such as those addressing the superficial deltoid, would further improve ankle stability. Additionally, our method of creating dPTTL injuries by detaching the proximal attachment to the tibia may not fully replicate the spectrum of injuries seen in clinical practice. The relative ease with which the ligament was repaired in this study may also not reflect the technical challenges encountered in a clinical setting. Another limitation was that robotic measurements included both the ankle and subtalar joints, whereas radiographic assessments were limited to evaluating isolated tibiotalar stability. Furthermore, the study did not account for the potential degradation of the reconstructed ligament over repeated tests. As the dPTTL was stretched during each test, it may have progressively weakened, potentially biasing the results against the effectiveness of deltoid repair alone, mainly as it was the last intervention tested. The lack of an a priori power analysis because of the descriptive nature of the study is another limitation that should be acknowledged.
Conclusion
This study indicates that the traditional practice of plate fixation on unstable Weber B fractures may not restore ankle stability, and additional deep posterior tibiotalar ligament reconstruction may be needed to achieve a stable ankle mortise. Further clinical studies should focus on distinguishing between patients with partial (SER4a) and complete deltoid ligament ruptures (SER4b) to evaluate if this has real clinical consequences.
Supplemental Material
sj-docx-2-fai-10.1177_10711007251334085 – Supplemental material for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning
Supplemental material, sj-docx-2-fai-10.1177_10711007251334085 for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning by Andreas F. Dalen, Martin G. Gregersen, Aleksander L. Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-docx-3-fai-10.1177_10711007251334085 – Supplemental material for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning
Supplemental material, sj-docx-3-fai-10.1177_10711007251334085 for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning by Andreas F. Dalen, Martin G. Gregersen, Aleksander L. Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-docx-4-fai-10.1177_10711007251334085 – Supplemental material for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning
Supplemental material, sj-docx-4-fai-10.1177_10711007251334085 for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning by Andreas F. Dalen, Martin G. Gregersen, Aleksander L. Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251334085 – Supplemental material for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning
Supplemental material, sj-pdf-1-fai-10.1177_10711007251334085 for Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning by Andreas F. Dalen, Martin G. Gregersen, Aleksander L. Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Footnotes
Ethical Approval
The Regional Committee for Medical and Health Research Ethics approved the study (ref. 178067).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.