
Abstract
Background:
Conventionally, transsyndesmotic fibula fractures with concomitant signs of deltoid ligament injury have been considered unstable and thus treated operatively. Recent studies have indicated that partial deltoid ligament rupture is common and may allow for nonoperative treatment of stress-unstable ankles if normal tibiotalar alignment is obtained in the weightbearing position. Biomechanical support for this principle is scarce. The purpose of this study was to evaluate the biomechanical effects of gradually increasing deltoid ligament injury in transsyndesmotic fibula fractures.
Methods:
Fifteen cadaveric ankle specimens were tested using an industrial robot. All specimens were tested in 4 states: native, SER2, SER4a, and SER4b models. Ankle stability was measured in lateral translation, valgus, and internal and external rotation stress in 3 talocrural joint positions: 20 degrees plantarflexion, neutral, and 10 degrees dorsiflexion. Talar shift and talar valgus tilt in the talocrural joint was measured using fluoroscopy.
Results:
In most tests, SER2 and SER4a models resulted in a small instability increase compared to native joints and thus were deemed stable according to our predefined margins. However, SER4a models were unstable when tested in the plantarflexed position and for external rotation in all positions. In contrast, SER4b models had large-magnitude instability in all directions and all tested positions and were thus deemed unstable.
Conclusion:
This study demonstrated substantial increases in instability between the SER4a and SER4b states. This controlled cadaveric simulation suggests a significant ankle-stabilizing role of the deep posterior deltoid after oblique transsyndesmotic fibular fracture and transection of the superficial and anterior deep deltoid ligaments.
Clinical Relevance:
The study provides new insights into how the heterogenicity of deltoid ligament injuries can affect the natural stability of the ankle after Weber B fractures. These findings may be useful in developing more targeted and better treatment strategies.
This is a visual representation of the abstract.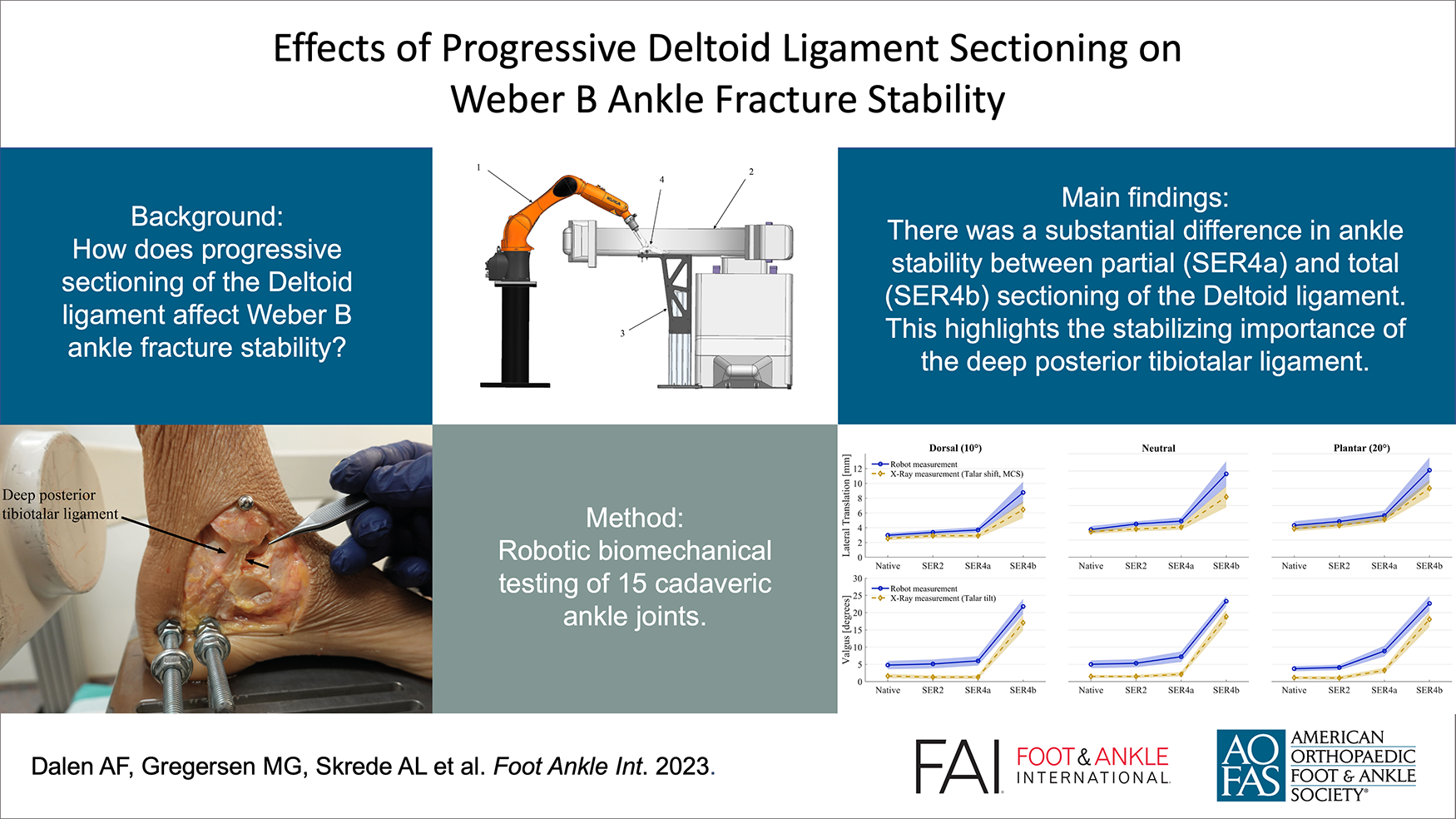
Introduction
Unstable Weber B/Lauge Hansen supination-external rotation (SER) ankle fractures are important to identify, in order to advise the correct treatment and reduce the risk of complications such as posttraumatic osteoarthritis (PTOA) of the ankle.4,5,10,11,19 An intact deltoid ligament prevents instability, even in fibula fractures, known as SER2 fractures. Traditionally, all fractures with radiographic and clinical signs of instability have been operatively treated. However, recent clinical studies have demonstrated that these fractures may appear with normal joint alignment if the radiographs are taken in the weightbearing position and thus may be considered as stable. It has been suggested that these are termed SER4a fractures 7 ; acceptable clinical and functional outcomes in the short and midterm have been reported after nonoperative treatment.3,6-8,13,15,16 However, the primary concern with nonoperative treatment of SER4a fractures is the risk of occult instability leading to PTOA in the long term.7,14
This study builds on Gougoulias and Sakellariou’s theory advocating that the superficial layer and deep anterior deltoid ligaments are injured whereas the deep posterior deltoid ligament remains intact in SER4a fractures. 7 From a biomechanical viewpoint, the superficial components of the deltoid ligament have no attachments to the talus itself. Thus, they are not directly crucial to stabilizing the talus in the mortise.6,16 Conversely, the deep anterior and posterior deltoid ligaments are critical stabilizers of the talus in the mortise as they originate from the medial malleolus and attach to the medial body of the talus.2,9 The deep anterior ligament has been found to be tight in plantarflexion and loose from plantigrade through dorsiflexion. 8 The exact opposite is valid with the deep posterior ligament. 8 This may explain why radiographic stability indicators can change depending on the ankle’s position.1,3,18 The probable cause for observed instability in radiographic stress tests of SER4a fractures may be ankle plantarflexion during stress radiography acquisition, which is a position where the intact deep posterior ligament naturally not engages, resulting in the appearance of an unstable mortise. On the contrary, in the weightbearing position with a more neutral positioned ankle joint, the deep posterior ligament will be engaged and therefore stabilize the ankle mortise by holding the talus in normal congruency with the tibia articular surface.
As biomechanical support for this SER 2 vs SER4a vs SER 4b theory is scarce, this study aimed to investigate the biomechanical effect of transsyndesmotic fibula fracture with no, partial, and total deltoid ligament injury compared to the native ankle joint. It was hypothesized that talar shift and valgus tilt of SER2 and SER4a models would be stable compared to native joints but unstable when comparing SER4b models.
Materials and Methods
The Regional Committee for Medical and Health Research Ethics approved the study (ref. 178067). Investigations were performed at Ålesund Biomechanics Lab, Ålesund, Norway.
Eighteen fresh frozen human cadaveric foot and ankle specimens (mid-crus to toe-tip) (Science Care, USA) were acquired for this study. Donors had consented to donation for research purposes. No cadaveric specimens had a medical history of injury or hardware/scars that indicated operative treatment of the ankle or hindfoot.
Test setup
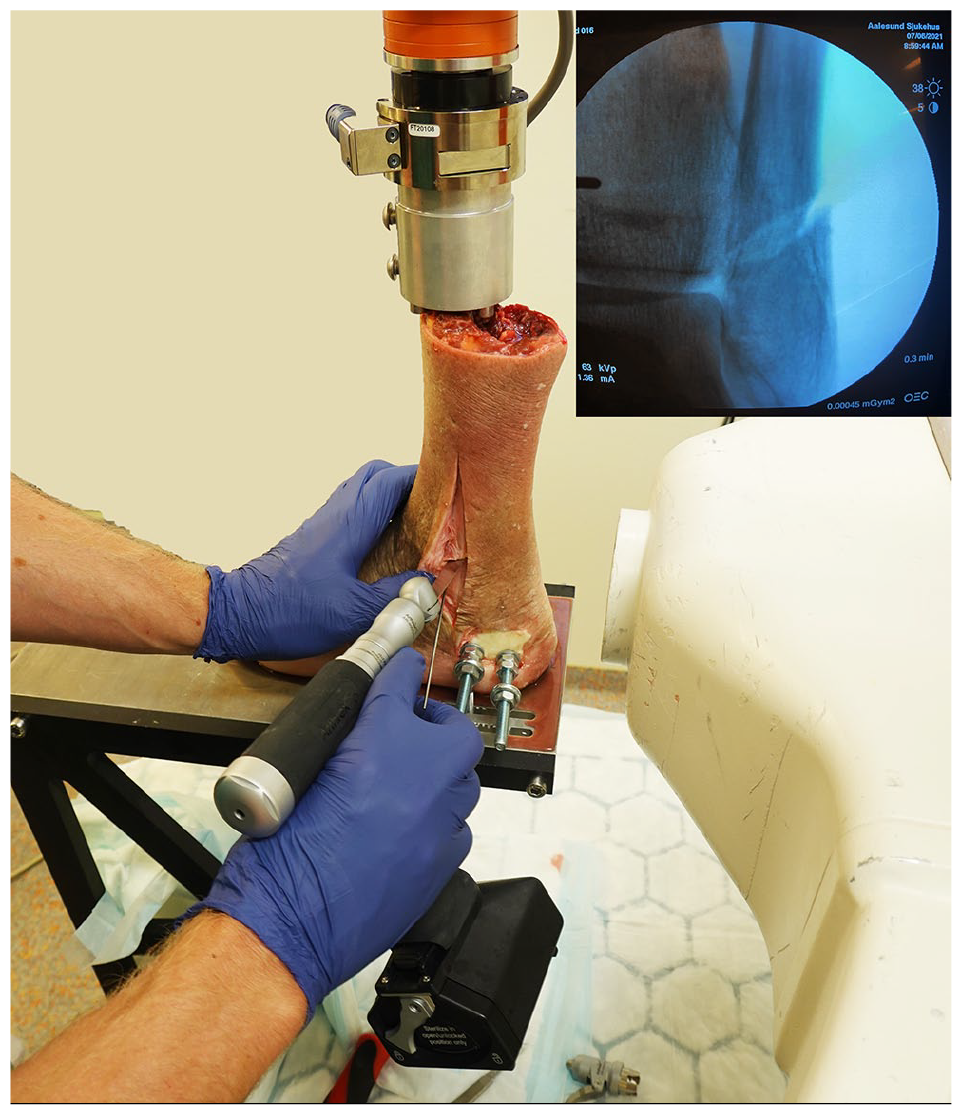
We used a floor-mounted industrial robot (KR6 R900 Sixx; KUKA, Augsburg, Germany) equipped with a force/torque sensor (Gamma, ATI Industrial Automation, NC, USA). The sensor was calibrated according to the SI-130-10 ATI standard, ensuring a resolution of 1/20 N and 1/800 N·m, and measuring all 6 components of force and torque. The robot has a pose repeatability of 0.03 mm and complies with ISO 9283. Each specimen was mounted with the ankle joint in neutral position with regard to rotation, flexion, and varus/valgus and oriented keeping the ankle dorsi-plantarflexion parallel with the working axis of the robot. The calcaneus was rigidly fixed to a mounting platform using 2 threaded rods and then the proximal tibia was fixed to the distal robot arm/force-torque sensor (Figures 1-3). Ankle specimen preparation and fixation are explained in detail in Appendix 1. A C-arm (FlexiView 8800, GE Healthcare, USA) was placed between the robot and the fixation platform to obtain radiographs of the ankle mortise. The test setup is shown in Figure 4.
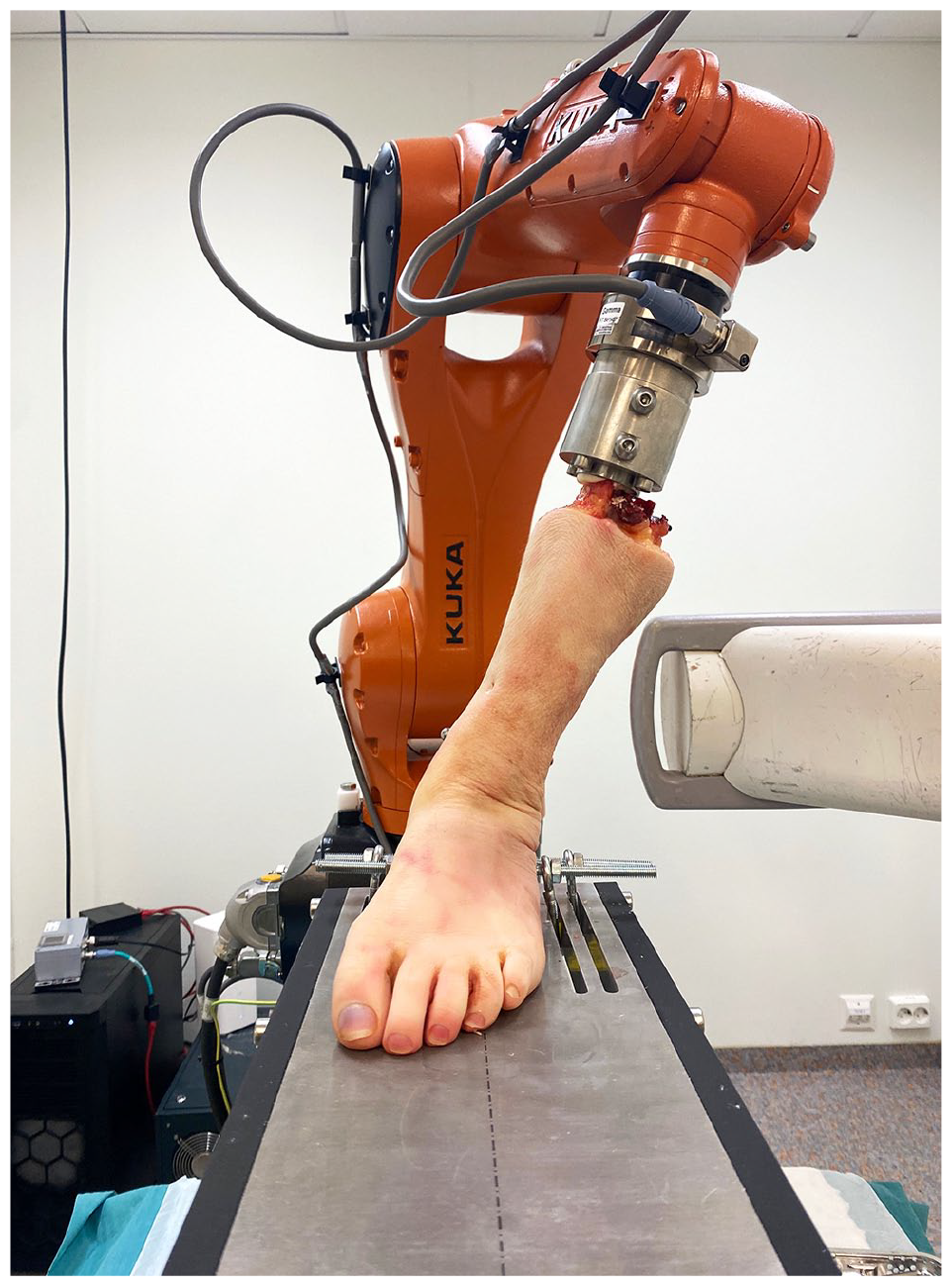
Actual test setup with the robot performing a valgus test on a specimen.
Depiction of how oblique, transsyndesmotic fibula osteotomies were made.
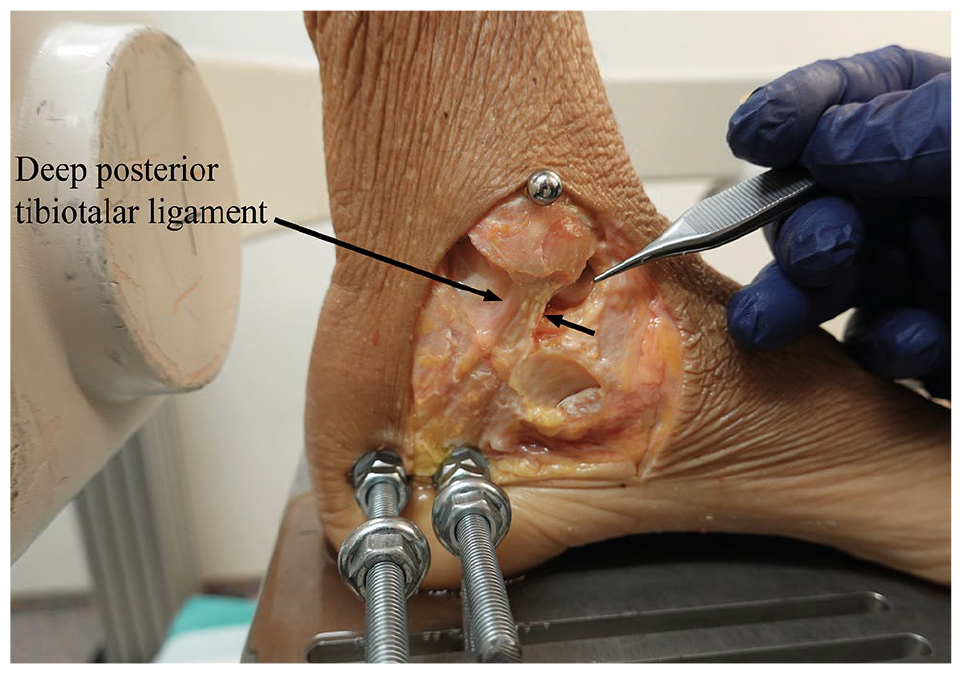
Medial view of an SER4a model showing an intact deep posterior tibiotalar ligament. The superficial and deep anterior deltoid ligament bands are removed.
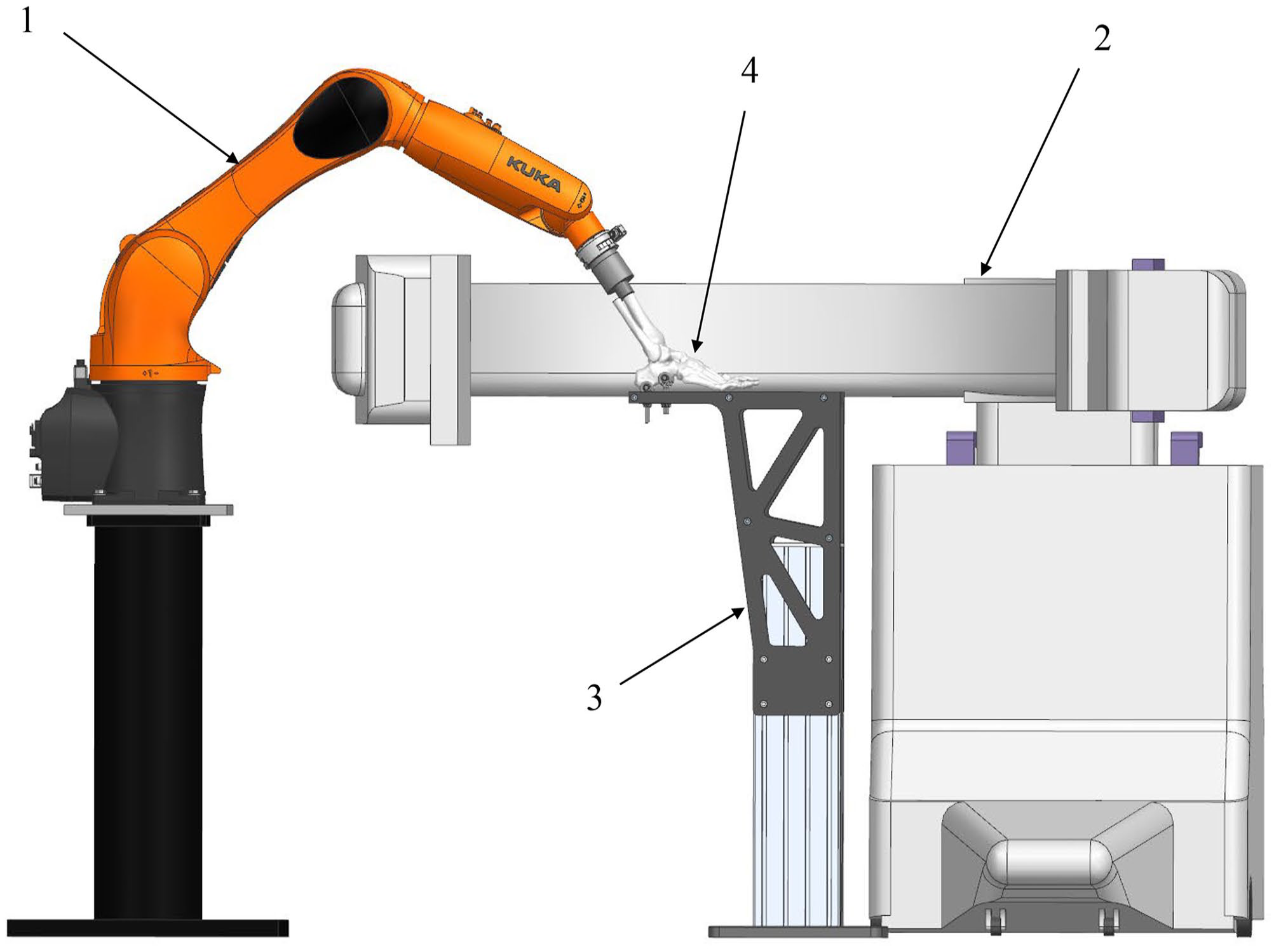
Schematic representation of the experimental setup for ankle stability testing, showing the robot (arrow 1), C-arm (arrow 2), fixation platform (arrow 3), and ankle cadaver specimen (arrow 4).
Biomechanical Testing Protocol
The force-guided robot performed the biomechanical tests by moving the tibia relative to the fixated calcaneus. Before each test, the ankle joint was centralized by the robot to achieve 0 N along the anterior-posterior and medial-lateral axes of the ankle. The position was confirmed by fluoroscopy. The robot applied a constant 45 N axial load on the tibia during the whole testing sequence. An axial load of 45 N was selected to reduce bias from congruent stability in the ankle joint. The stability tests were performed in 3 talocrural joint positions; 10 degrees dorsal flexion, neutral, and 20 degrees plantarflexion. The positions were defined by the robot in the global coordinate system and verified by fluoroscopy. Within this range of motion, the subtalar involvement is minimal, the posterior deep deltoid ligament ranges from tight to loose, 8 and the positions are achievable in a clinical setting. All specimens were expected to reach these positions. Still, a torque limit was set to 3 N·m when moving the ankles to plantar- and dorsiflexion. Any specimen reaching this torque would stop and then be tested at that position.
In each position, the robot performed 4 tests for stability: a lateral translation test followed by external rotation, internal rotation, and valgus tests. The lateral translation test applied a 30-N force oriented laterally while maintaining the 45-N axial load. Any force that arose in the anterior-posterior axis was ignored, and movement of the tibia was purely axial or lateral-medial. The rotational and valgus tests were performed as rotation about the respective axes until achieving a torque of 2 N·m or until reaching 25 degrees for valgus or 40 degrees for external or internal rotation. A valgus test is demonstrated in Figure 1. When the force or torque limit was reached, an ankle mortise view radiograph was obtained for the lateral translation and valgus tests. The industrial robot measured movements of the whole ankle complex, including the talocrural and subtalar joints. Isolated movement in the talocrural joint in lateral translation and valgus tests was measured on radiographs as talar shift and talar tilt, respectively.
All specimens were tested sequentially as native joint, SER2, SER4a, and SER4b models.
Creation of progressive joint injury
Description of Lauge-Hansen SER classification and corresponding bone and soft tissue injuries used in the creation of injury models are described in Table 1. The Weber B fracture was made by inserting a 1.6-mm Kirschner wire through the fibula at the same level as the talocrural joint line, marking the lower limit of the fracture. Then an oblique osteotomy in the fibula was made level with the syndesmosis with an oscillating saw, sloping downward from the posterior to the anterior cortex and from the lateral to the medial cortex of the fibula (Figure 2) and the SER2 model was tested. The relevant parts of the deltoid ligaments were transected using a scalpel. In the SER4a model, the superficial and deep anterior fibers of the deltoid were transected and the deep posterior tibiotalar ligament fibers were preserved (see Figure 3). After testing this, the SER4b model was created by transecting the remaining deep posterior tibiotalar ligament fibers.
Description of Lauge-Hansen SER Classification and Corresponding Bone and Soft Tissue Injuries Used in the Creation of Injury Models.
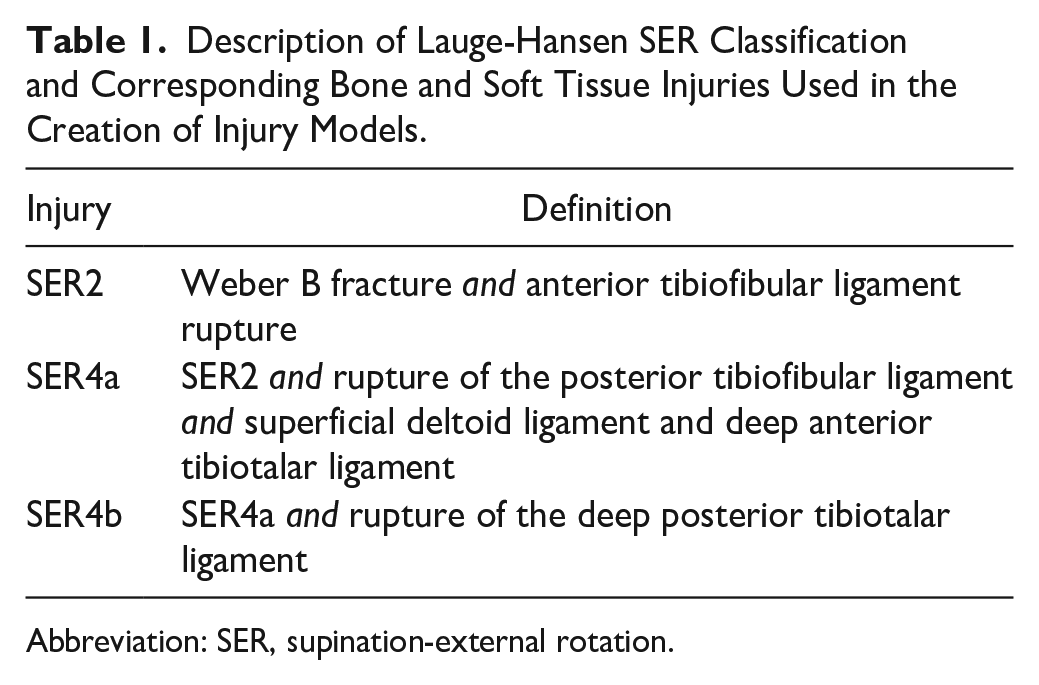
Abbreviation: SER, supination-external rotation.
Outcomes
The primary outcome was the change from the native joint in radiographic talar shift (millimeters) at the 3 stages of joint injury (SER2-4b) measured at neutral ankle position. Talar shift was defined as the medial clear space (MCS) recorded in millimeters on mortise view radiographs. Consistent with previous descriptions,9,17 we defined the MCS as the distance between the medial border of the talus and the lateral border of the medial malleolus on a line parallel to and 5.0 mm below the talar dome, which in previous studies has demonstrated excellent reliability. 9 The minimal clinically important difference (MCID) for defining talar shift instability was previously defined as 1.0 mm.15,19
Secondary outcomes included change from the native joint in movements of radiographic talar valgus tilt (degrees) and robotic measurements of lateral translation (millimeters), valgus (degrees), and internal and external rotation (degrees) in the whole ankle complex at the 3 stages of progressive joint injury (SER2-4b). Talar tilt was measured as the angle between the tibia’s distal articular surface and the talus’s superior articular surface. Our MCID for talar tilt instability was 7.0 degrees, consistent with a previous report. 16 No MCID value for defining rotational instability exists.
Radiographic measurements were obtained using Sectra IDS7, version 23.2 (Sectra AB, Linköping, Sweden).
Statistical Analysis
Descriptive statistics were presented using means and corresponding SDs. Ninety-five percent CIs were calculated under the assumption of normality. Normality was tested using the Shapiro-Wilk normality test and investigated by visual inspection of histograms for each combination of subgroup and outcome. For most subgroups, the results did not indicate significant deviance from normality. To test pairwise differences in means across groups, we used linear mixed models with random intercepts study specimens to account for dependency in the data. As this was considered a descriptive study, no formal power analyses were done a priori. All analyses were done using Stata, version 17.0 (StataCorp, College Station, TX).
Results
Specimens
On dissection, major ankle osteoarthritis (n = 2) or major arthrofibrosis indicating previous ankle trauma (n = 1) was discovered, excluding these 3 specimens. The remaining 15 were included in the analyses. Seven of 15 were female, with 7 right ankles. The average age at death was 71 years (range, 55-87).
Biomechanical Tests
Figures 5 and 6 displays biomechanical stability in native joints, and 3 stages of progressive injury (SER2, SER4a, and SER4b) measured in 10 degrees dorsiflexion, neutral, and 20 degrees plantarflexion.
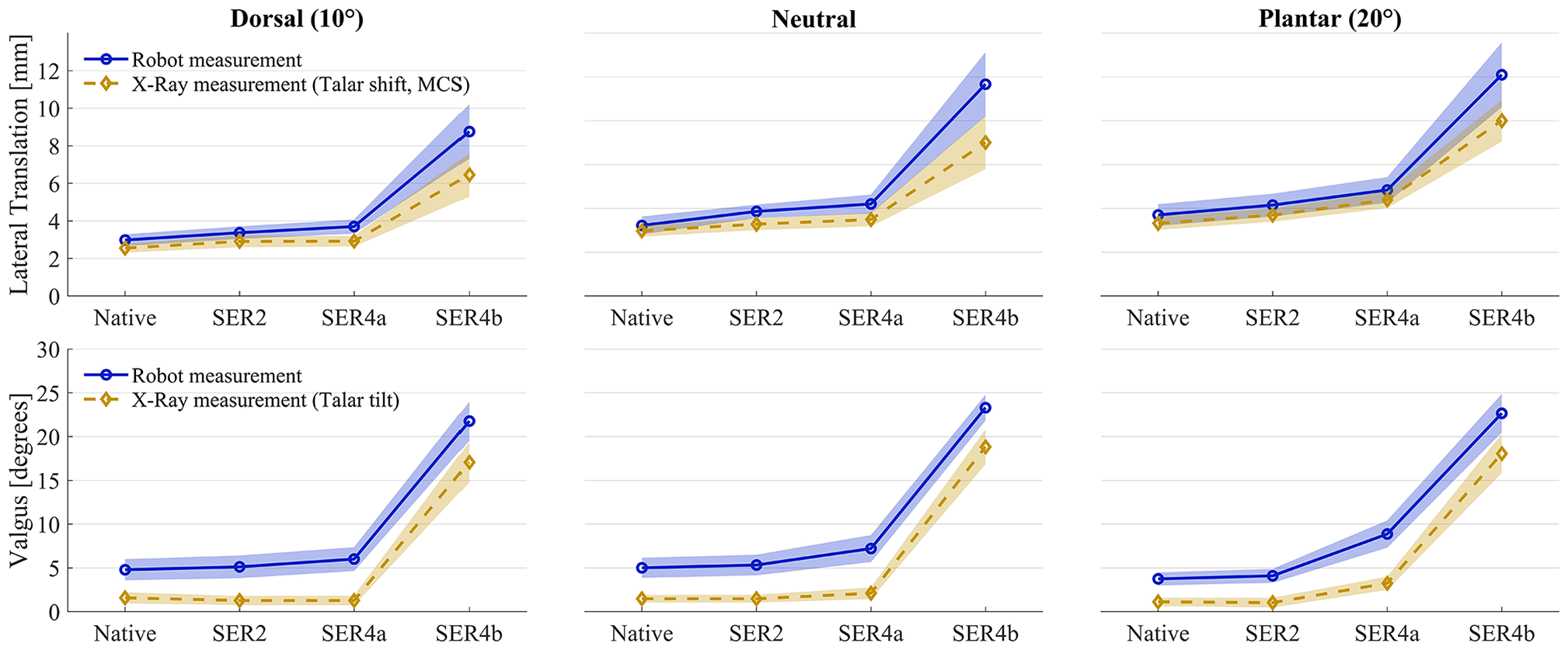
Biomechanical stability measurements for lateral translation and valgus tests for 15 ankle specimens tested sequentially as native, SER2, SER4a, and SER4b models. The figure shows a substantial difference in ankle stability between SER4a and SER4b models. The markers represent means, whereas the shaded areas indicate the 95% CI for the mean. Blue circular markers with shade represent robot measurement over the entire ankle complex, including the talocrural and subtalar joints. Yellow diamond markers and shade represent the radiographic measurements, with talar shift measured as medial clear space (MCS) for lateral translation, and talar tilt for valgus.
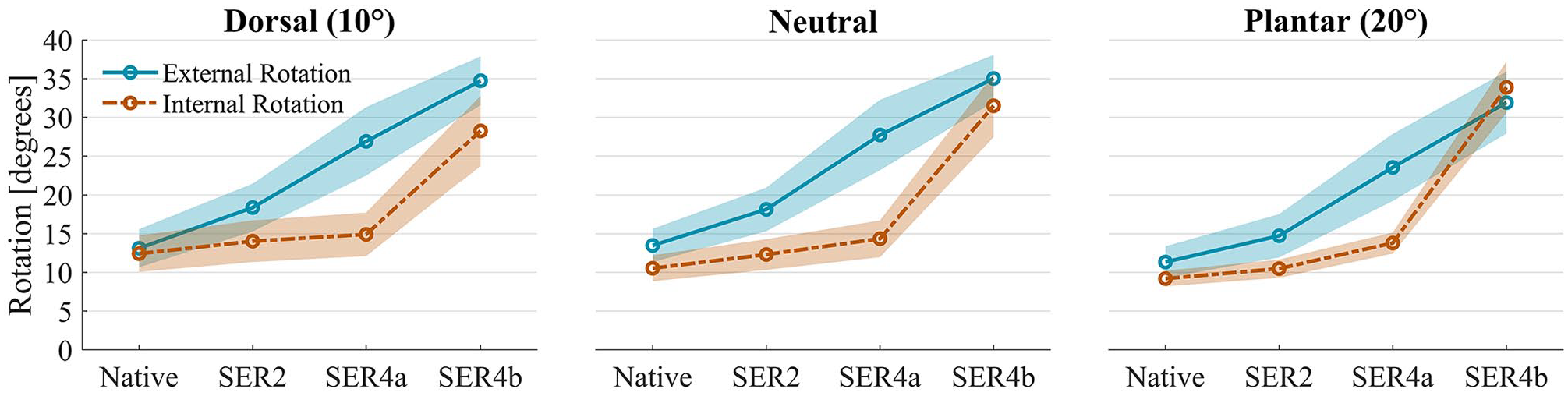
Biomechanical stability measurements for internal and external rotation for 15 ankle specimens tested sequentially as native, SER2, SER4a, and SER4b models. The figure shows a substantial difference in ankle stability between SER4a and SER4b models for internal rotation (dashed line). However, for external rotation, all injury states were unstable. The markers represent means, and the shaded areas indicate the 95% CI for the mean. All measurements were done using the robot.
All comparisons between native joint and injury models with mean differences, 95% CIs, and P values are available in Table 2, and all measures with SDs in Table 3.
Mean Difference in Stability for 15 SER2-4b Injury Models Compared to Native Ankles. a
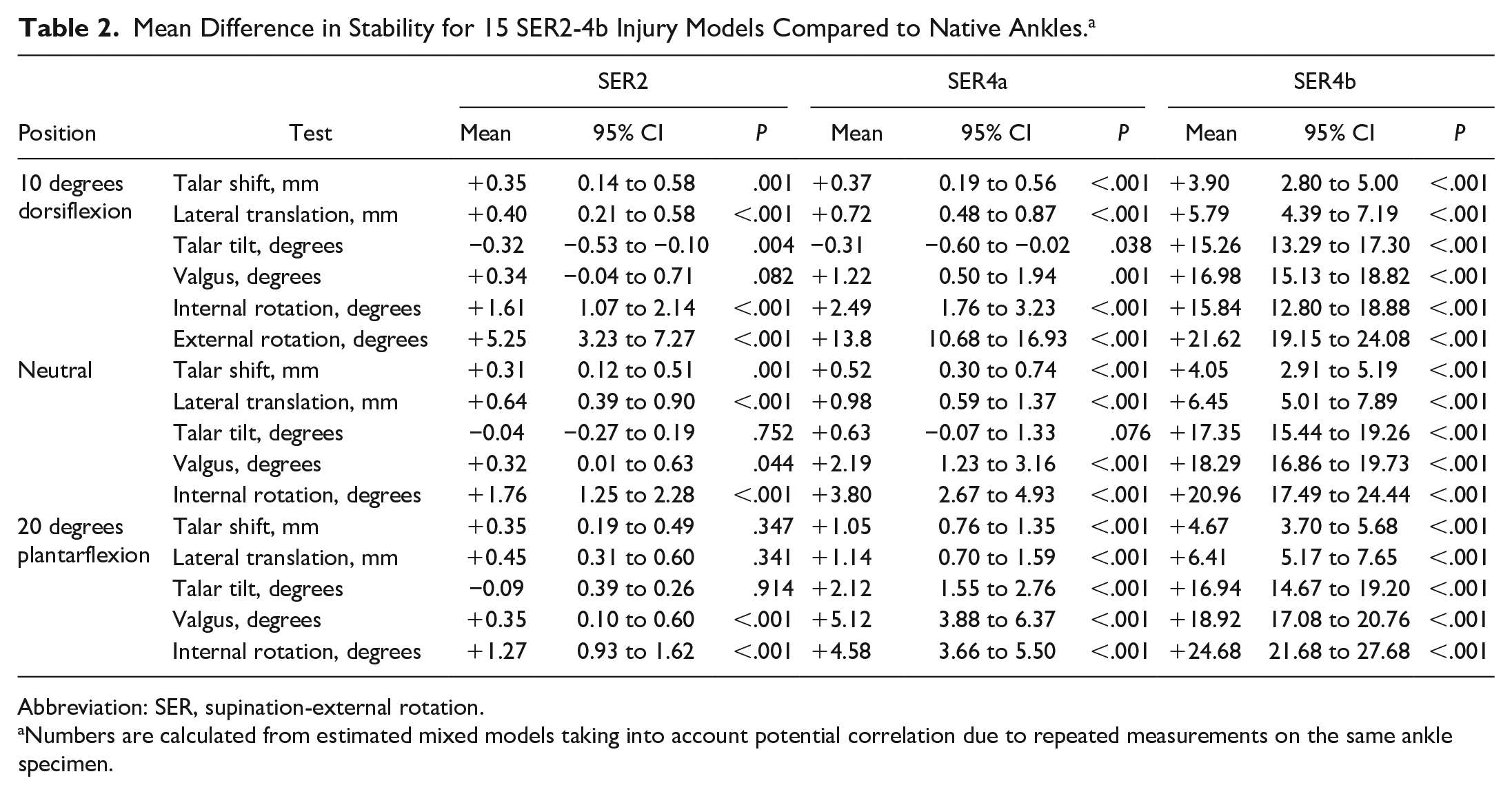
Abbreviation: SER, supination-external rotation.
Numbers are calculated from estimated mixed models taking into account potential correlation due to repeated measurements on the same ankle specimen.
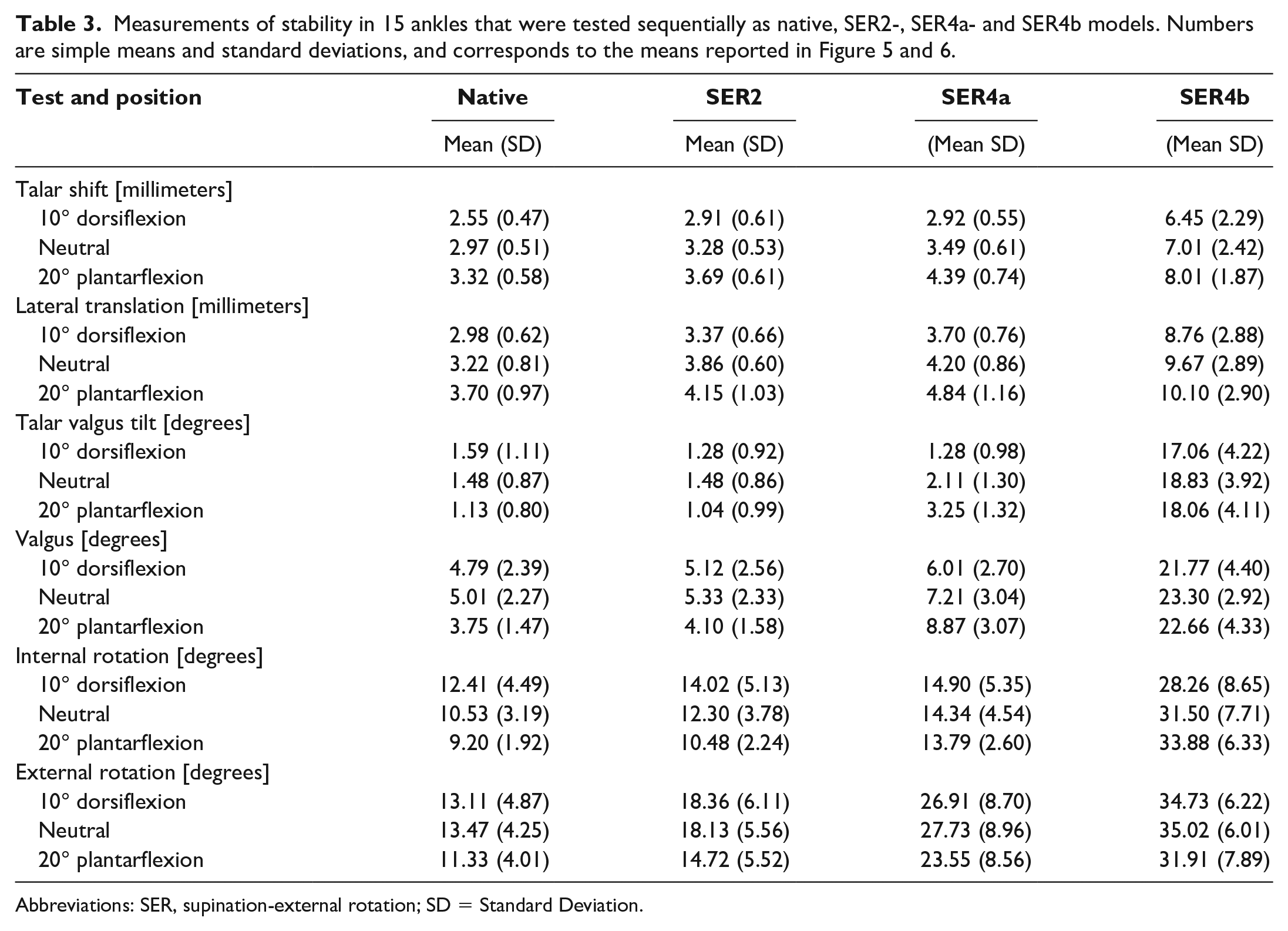
Abbreviations: SER, supination-external rotation; SD = Standard Deviation.
Talar Lateral Shift and Lateral Translation Tests
Reviewing talar shift (radiographic measurements) at neutral ankle position, all comparisons with native joints were significant (P < .001 for all comparisons), but only SER4b models were unstable with +4.05 mm. Comparable increases but larger magnitudes were observed with lateral translation (robot measurements). Similar changes were observed at 10 degrees of ankle dorsiflexion, with only differences between SER4b models and native state at +5.79 for the robot and +3.90 mm for radiographic measurements being unstable (P < .001 for both comparisons). At 20 degrees ankle plantarflexion, compared to the native state, only SER4a and SER4b models were unstable with +1.05 and +4.67 mm, respectively, on radiographs and +1.14 and +6.41 mm, respectively measured by robot (P < .001 for all comparisons).
Talar Valgus Tilt and Valgus Tests
At neutral ankle position, compared to the native state, mean increases of −0.04 degrees (P = .752), +0.63 degrees (P = .076), and +17.35 degrees (P < .001) talar tilt (radiographic measurement) were demonstrated for SER2, SER4a, and SER4b models, respectively, with SER4b models being unstable. Similarly, increases in valgus (robot measurements) were +0.32 degrees (P = .044), +2.19 degrees (P < .001), and +18.29 degrees (P < .001) for SER2, SER4a, and SER4b models, respectively. Tests at 10 degrees of ankle dorsiflexion yielded similar results, with only SER4b models being unstable at mean +15.26 degrees (P < .001) talar tilt and +16.98 degrees (P < .001) valgus. Greater magnitudes in the SER4a models occurred with 20 degrees ankle plantarflexion relative to the native state with mean +2.12 degrees talar tilt and +5.12 degrees valgus (P < .001 for both comparisons), but only SER4b models were unstable with +16.94 degrees talar tilt and +18.92 degrees valgus (P < .001 for both comparisons).
Internal Rotation Tests
With internal rotation, all comparisons significantly differed from the native state (see Table 2). In SER4a models, the mean change from the native was +3.80 degrees, +2.49 degrees, and +4.58 degrees measured at neutral, 10 degrees of ankle dorsiflexion, and 20 degrees plantarflexion (P < .001 for all comparisons), respectively. Major instability was observed in the SER4b models (all >+15.00 degrees) in all positions (P < .001 for all comparisons).
External Rotation Tests
With external rotation, all comparisons significantly differed from native (see Table 2). Changes in external rotation differed from other tests in that a more linear increase occurred from native through SER2, SER4a, and SER4b models, as visualized in Figure 6. In SER2 models, differences of +5.25 degrees (P < .001) or more were observed at all positions. The SER4a and SER4b models demonstrated +12.22 degrees (P < .001) and +20.58 degrees (P < .001) or larger differences compared to the native state, respectively.
Discussion
This study’s main findings suggest a substantial difference in ankle stability between SER4a and SER4b models and highlight the stabilizing importance of the deep posterior tibiotalar ligament. In general, the SER2 and SER4a models were stable according to our predefined margins. In contrast, in SER4b models, large-magnitude instability was observed in all directions and all test positions. These findings suggest a stability heterogeneity within Weber B ankle fractures with a concomitant deltoid ligament injury and support differentiating treatment between partial (SER4a) and complete (SER4b) deltoid ligament injuries.
Biomechanical data on the stability of Weber B fractures with partial deltoid ligament injury is limited. However, a recent study by McCormack et al 16 tested 8 cadavers as intact, SER2, SER4a, and SER4b models when axially loaded (750 N) and with external rotation stress reporting that ankles upheld stability up until division of the deep posterior tibiotalar ligament (SER4b model). Our study is comparable to previous research, but with some methodological differences: Our study involved more tests, combining both robot and radiographic measurements and using different force levels compared to previous studies. Previous studies were conducted with a large axial load, whereas we used less axial load (45 N) but greater displacement force (30 N). This design aimed to increase sensitivity to detect possible instability, owing to evidence that the highly congruent ankle joint autostabilizes with axial load.16,21 Although our stability findings likely does not accurately reflect weightbearing ankle stability, they do provide insight into the threshold at which fractured ankles become unstable. Our results support previous evidence and add new evidence of stability in various ankle positions and directions tested.
Clinical Relevance
Traditionally, Weber B ankle fractures with signs of deltoid ligament injury are considered unstable and treated with operative fixation, including both SER4a and SER4b fractures. However, the results of this study demonstrate that SER4a models were not more unstable than native joints by a clinically relevant amount in most tests, whereas SER4b models were. The rationale for operative fixation of ankle fractures is that potential talar displacement may lead to altered joint contact surface area, osteoarthritis development, and poor function. 7 The potential for talar displacement in this study was minimal in all tests of SER2 models and in tests at neutral and 10 degrees dorsiflexion of SER4a models. Noteworthy, we found clinically relevant talar shift instability when SER4a models were tested at 20 degrees plantarflexion. When testing internal rotation, comparisons of SER2 and SER4a models and native state were statistically significant, but differences were <2 and <5 degrees, respectively, and clinical relevance seems uncertain. External rotation tests stood out in that an instability increase was observed starting with SER2 models and continuing linearly through SER4a and SER4b models, indicating that even an isolated transsyndesmotic fibula fracture increases talar external rotation. These findings may be challenging to interpret as what constitutes a clinically relevant increase in external rotation is uncertain.
Although some clinical studies have suggested that nonoperative treatment can lead to good outcomes for SER4a fractures,9,12,13,20,22 there is still no consensus on whether operative or nonoperative treatment is the better option. Our findings align with the study by McCormack et al. 16 supporting that injury to the deep posterior tibiotalar ligament may represent the watershed for whether surgery is warranted. But even advocates of nonoperative treatment for SER4a fractures are divisive about alternative nonoperative approaches.7,9 Foremost, it has been argued that immobilization at a neutral ankle position is essential to avoid plantarflexion as plantarflexion may result in late deltoid insufficiency and increased risk of PTOA. 7 Such argument may be supported by our results, where SER4a models had an overall instability increase at 20° of plantarflexion. Although limits for when valgus and internal rotation instability affect the risk of ankle PTOA are unknown, lateral translation instability of +1.05 mm (P < .001) may be argued to be clinically relevant. These findings imply that stability is compromised in the plantarflexed position, which may have clinical implications in the nonweightbearing ankle, that is, in the swing phase of gait. Nonetheless, as the ankle joint is subject to less load and mechanical stress when unloaded, the clinical importance of instability in the plantarflexed ankle seems uncertain if the ankle is stable when loaded (i.e., during stance). These findings highlight the importance of understanding the biomechanics of ankle joint instability caused by partial deltoid ligament injury in different positions of ankle dorsiplantarflexion to develop targeted interventions and rehabilitation strategies (i.e., physiotherapy protocols) to reduce the risk of PTOA.
Limitations
The chosen equivalence margin is important for the study’s validity. Talar shift is considered the critical clinical parameter when evaluating the stability of ankle fractures and thus was our primary outcome. Although we do not know the exact degree of instability that increases the risk of PTOA, some data exist. Owing to evidence of substantial joint contact surface area loss with 1.0 mm lateral translation of the talus relative to the tibia,15,19 a change larger than this compared to the native joint may be considered clinically important. However, the study’s findings should be viewed as exploratory because evidence on what constitutes clinically important changes in valgus and rotations are limited.
Another limitation of this study was that the robotic measurements were obtained over the ankle and subtalar joints, whereas only radiographic measurements indicated isolated tibiotalar stability. In our test setup, radiographic measurements were possible for lateral translation and valgus tests, meaning the study could not accurately capture isolated instability in the ankle joint when testing rotations.
For the lateral translation test, the changes in MCS measurements between tests and test positions were small (<1 mm). And, because there is some uncertainty regarding the accuracy of radiographic measurements, these results must be interpreted with some caution.
Furthermore, ankle fractures exhibit specific patterns, and imaging studies have confirmed that the SER injury mechanism can result in Weber B fractures with partial deltoid ligament injury. 2 Still, cadaveric specimens with replicated injuries may not fully represent the complexity and variability of in vivo joint mechanics. Additionally the types of injuries we created may not truly replicate the range of in vivo injuries. And by necessity we preselected loading amounts, safety margins, loading positions, and order of testing. The effects of these variables and clinical relevance remains unknown. Although the findings of this study provide important insights into ankle joint stability and the role of a deltoid ligament injury in ankle fractures, future studies using in vivo measurements, other loading and tracking cadaveric simulated-injury systems, and larger sample sizes will be helpful to confirm and expand on these results.
Conclusions
This study provides new insights into the heterogeneity of Weber B ankle fractures with concomitant deltoid ligament injuries by demonstrating a meaningful difference in ankle stability between partial (SER4a) and complete deltoid ligament injuries (SER4b).
Supplemental Material
sj-docx-2-fai-10.1177_10711007231180212 – Supplemental material for Effects of Progressive Deltoid Ligament Sectioning on Weber B Ankle Fracture Stability
Supplemental material, sj-docx-2-fai-10.1177_10711007231180212 for Effects of Progressive Deltoid Ligament Sectioning on Weber B Ankle Fracture Stability by Andreas F. Dalen, Martin G. Gregersen, Aleksander L. Skrede, Øystein Bjelland, Tor Åge Myklebust, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231180212 – Supplemental material for Effects of Progressive Deltoid Ligament Sectioning on Weber B Ankle Fracture Stability
Supplemental material, sj-pdf-1-fai-10.1177_10711007231180212 for Effects of Progressive Deltoid Ligament Sectioning on Weber B Ankle Fracture Stability by Andreas F. Dalen, Martin G. Gregersen, Aleksander L. Skrede, Øystein Bjelland, Tor Åge Myklebust, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from The Regional Committees for Medical and Health Research Ethics in Norway, reference number 178067.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.