
Abstract
Background:
Weber B fractures with concomitant deltoid ligament injury have traditionally been operated with open reduction and internal fixation of the fibular fracture. More recently, clinical studies have suggested that some fractures have concomitant partial deltoid ligament injury with the deep posterior tibiotalar ligament intact (SER4a), allowing for nonoperative treatment in this subgroup. This study explores whether plate fixation of the fibula improves ankle stability in an SER4a injury model. And if so, does it restore native ankle stability?
Methods
Fifteen cadaver ankle specimens were tested in 3 states using an industrial robot: intact joint, SER4a models without plate fixation of the fibula, and SER4a models with plate fixation of the fibula. The robot measured ankle stability in lateral translation, valgus, and internal and external rotation in 3 talocrural joint positions: 10 degrees dorsiflexion, neutral, and 20 degrees plantar flexion. Furthermore, fluoroscopic mortise view radiographs were taken to measure isolated talar shift and talar tilt.
Results:
The talar shift and tilt tests showed no differences between the SER4a injury model with and without fibular plate fixation at neutral ankle position with a mean difference of −0.16 mm (95% CI −0.33 to 0.01 mm, P = .071) for talar shift and −0.15 degrees (95% CI −0.01 to 0.30 degrees, P = .068) for talar tilt. However, plate fixation increased external rotation stability, with mean improvements ranging from −7.43 to −9.52 degrees (P < .001 for all comparisons), but did not restore intact ankle stability. For internal rotation, plate fixation resulted in minor differences.
Conclusion:
The results of this suggest that plate fixation of the fibular fracture primarily improves external rotation stability but does not substantially improve lateral translation, valgus, or internal rotation stability in SER4a injury models. In this robotic cadaver model, fibular plate fixation did not fully restore intact ankle stability after simulated SER4a injury.
Clinical Relevance:
This study offers insights into the effects of fibular plate fixation on Weber B/SER4a injury models and may assist informed decisions when selecting treatments for these types of fractures.
This is a visual representation of the abstract.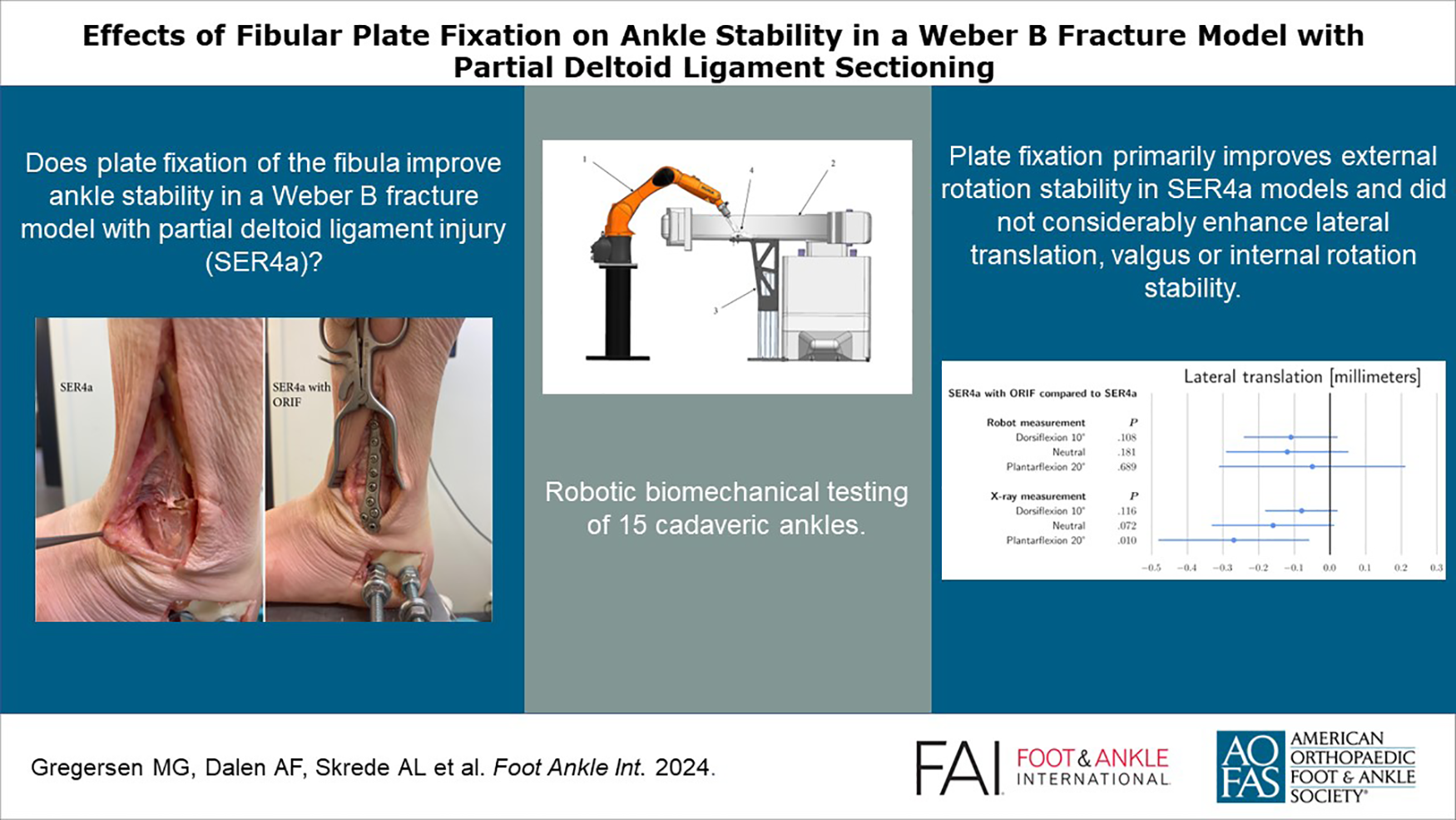
Introduction
Weber B/supination-external rotation (SER) fractures with signs of deltoid ligament insufficiency are considered unstable and traditionally treated operatively with open anatomic reduction and internal fixation of the fibular fracture, most commonly with plate and screws. However, understanding ankle fractures with concomitant deltoid ligament injuries has evolved.4-6 The traditional binary understanding of stability, either as stable or unstable, has been challenged by clinical and biomechanical findings indicating that partial deltoid ligament injuries, where the deep posterior tibiotalar ligament (dPTTL) remains intact, are common.2,4-6,9 It has been proposed to classify such injuries as SER4a. 4 In clinical practice, this injury is identified by an unstable radiographic stress test but a stable weightbearing radiograph.4-6 Conversely, injuries that are genuinely unstable, potentially featuring a complete deltoid rupture, can be classified as SER4b based on both stress tests and weightbearing radiographs indicating instability.
The traditional practice of operative treatment of stress unstable ankle fractures is controversial. A solitary randomized controlled trial found no significant difference in functional outcomes between operative and nonoperative treatment. 12 Other studies have suggested that fractures that are stable on weightbearing radiographs (SER2 and SER4a) can be treated nonoperatively with satisfactory short- and midterm results.3,5-8,11,13,14
We defined ankle stability as the joint’s ability to remain anatomically aligned in the presence of deforming forces. Two recent biomechanical studies support the nonoperative treatment of SER4a fractures.2,9 These studies demonstrated that ankles upheld stability with oblique transsyndesmotic fibular fracture and transection of the superficial and deep anterior deltoid ligaments. Still, they showed substantial increases in instability between the SER4a and SER4b states, suggesting a significant ankle-stabilizing role of the dPTTL, indicating that rupture of the dPTTL (SER4b) may represent the threshold for when the ankle becomes unstable. However, no previous study has evaluated the stabilizing effect of plate fixation of the fibula on SER4a injury models. This study aimed to quantify the biomechanical effects of anatomic reduction and plate fixation on ankle stability in SER4a injury models compared with SER4a injury models without plate fixation and intact joints.
Materials and Methods
Eighteen fresh frozen human cadaver foot and ankle specimens (mid-crus to toe-tip) (Science Care, USA) were acquired for this study. Donors had consented to donation for research purposes. No cadaver specimens had a medical history of injury or hardware/scars indicating operative ankle or hindfoot treatment. Investigations were performed at Aalesund Biomechanics Lab, Aalesund, Norway.
Test Setup, Specimen Preparation, and Fixation
The test setup, specimen preparation and fixation have previously been described in detail. 2 The tests were performed using a floor-mounted industrial robot (KR6 R900 Sixx; KUKA, Augsburg. Germany) fitted with a force/torque sensor (Gamma; ATI Industrial Automation, Apex, NC) measuring all 6 components of force and torque independently. A C-arm (FlexiView 8800; GE Healthcare, Chicago, IL) captured ankle mortise view radiographs. The test setup is shown in Figure 1.
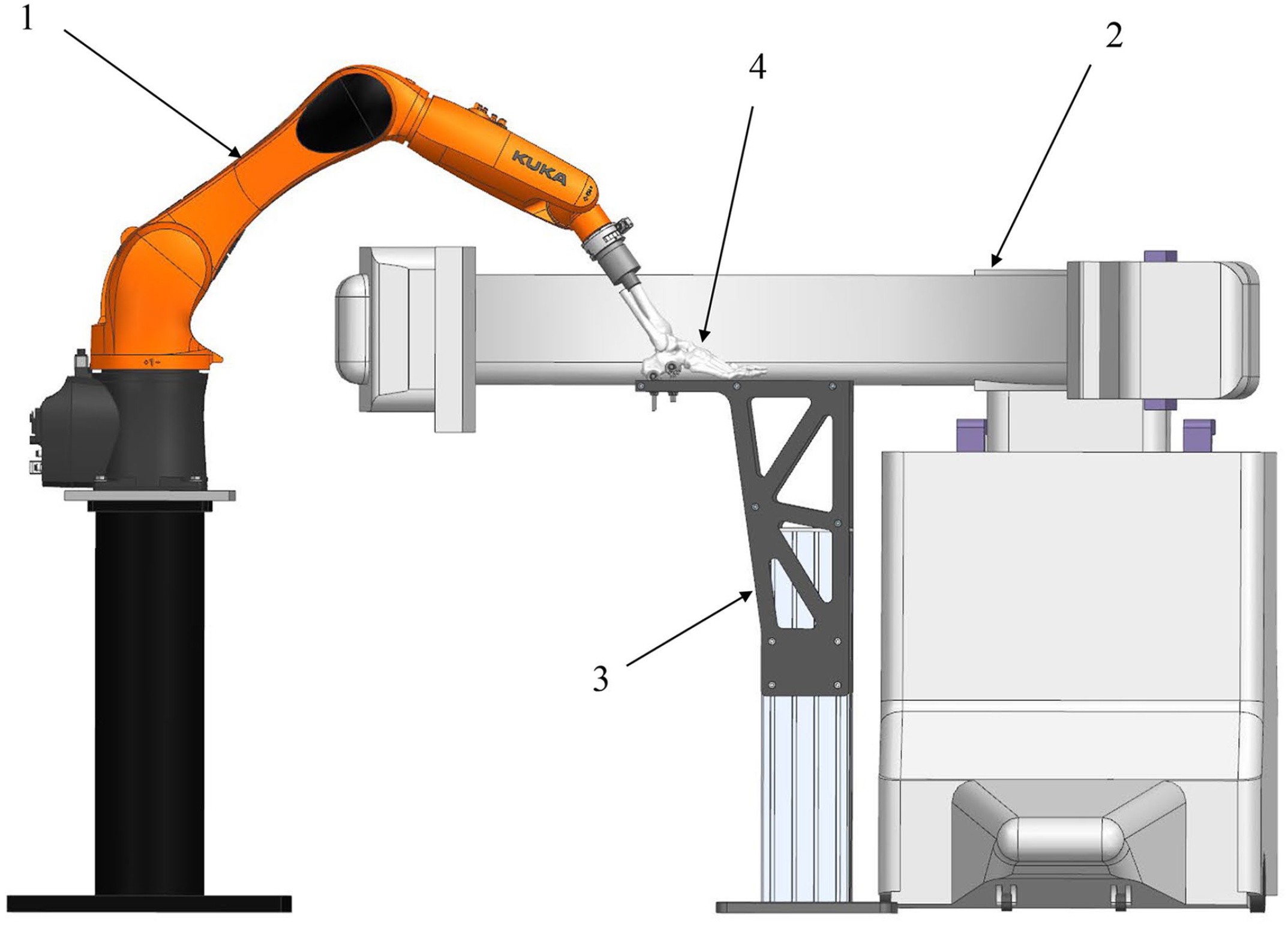
Schematic representation of the experimental setup for ankle stability testing, showing the robot (arrow 1), C-arm (arrow 2), fixation platform (arrow 3), and ankle cadaver specimen (arrow 4).
All specimens were stored at −23°C and thawed at room temperature for at least 12 hours before dissection and testing. The medial aspect of the ankle was thoroughly dissected, exposing the deltoid ligament with all the individual bands marked for later sectioning. The tibia shaft was osteotomized 22 cm proximal to the distal tip of the medial malleolus. The skin, soft tissue, and muscle were removed from the proximal 6 cm of the tibial shaft, and the fibula was osteotomized at the same level as the remaining soft tissue, leaving the fibula free. The proximal part of the remaining tibia was embedded in an aluminum cylinder using a 2-component polyurethane casting resin blend (Rencast FC 52/53 Isocyanate, Polyol FC 53, Filler DT 082; Huntsman Corp, Woodlands, TX). The calcaneus cavity was reinforced through a lateral cortical window using the same 2-component resin. Then, 2 threaded rods (M8, stainless steel) were drilled through the calcaneus from lateral to medial and secured with washers and nuts on each side.
The specimen was placed with the foot plantigrade on the rigid fixation platform and then positioned with the plane of the ankle dorsi-plantarflexion parallel to an engraved centerline marking the working axis of the robot. The calcaneus was rigidly fixed to the platform using 2 eyebolts around each threaded rod. The eyebolts were running through slots in the plate and secured with nuts. During the hindfoot fixation process, fluoroscopy was used to ensure that the upper talar articular surface was horizontally aligned with the mounting plate in the frontal plane. Next, the cylinder on the proximal tibia was attached to the force-torque sensor on the distal robot arm, keeping the ankle joint in an anatomically neutral position concerning rotation, flexion, and varus/valgus.
Biomechanical Testing Protocol
The robot biomechanical tests were conducted by moving the tibia relative to the fixed calcaneus. Initially, in the native state for each tested specimen, the robot centralized the ankle joint by applying 45 N axially along the tibia and equilibrating the arising forces along the anterior-posterior and medial-lateral axes. The centralized position was also verified by fluoroscopy. This served as the initial position for all subsequent tests. The stability tests were performed in 3 positions of the talocrural joint: 10 degrees dorsal flexion, neutral, and 20 degrees plantar flexion. These joint positions were selected to test the stability of the dPTTL in different states of tension. A constant 45-N axial force was applied to the tibia for all flexion angles during all tests. This force is substantially lower than the actual ankle loading when walking or standing. A higher load would increase stability because of the bony congruence of the joint surfaces, and we chose to use this load as our test setup was designed to maximize sensitivity for detecting instability.
For each position, the robot performed 4 stability tests: (1) lateral translation, (2) external rotation, (3) internal rotation, and (4) valgus. The robot measured the combined movements of the talocrural and subtalar joints. Additionally, isolated movement in the talocrural joint was measured on radiographs for lateral translation and valgus tests and reported as talar shift and tilt. A 30-N force was applied, displacing the tibia medially for the lateral translation test while maintaining the 45-N axial load. Movement of the tibia was purely axial or lateral-medial. During the rotational and valgus tests, the ankle joint was rotated around the respective axes until a 2-Nm torque was achieved or reached 25 degrees for valgus or 40 degrees for external and internal rotation. Two-newton-meter torque was selected based on experience from previous studies, as it was high enough to demonstrate the difference in magnitude of rotation between tests and states, but at the same time, it did not stretch the soft tissue extensively in each robot test sequence. In pilot studies, convergence to 2 Nm was achieved within 0 to 25 degrees for valgus and 0 to 40 degrees of rotation, and these were selected as the outer displacement limits. An ankle mortise view radiograph was obtained for the lateral translation and valgus tests when the force or torque limit was reached.
The testing protocol was repeated in 3 successive steps for each specimen. In step 1, baseline measurements were obtained from an intact specimen with all anatomical structures intact and the deltoid ligament visualized. In step 2, an SER4a injury model was tested. An oblique transsyndesmotic fibular osteotomy was made using an oscillating saw. The joint line was marked with a pin guided by fluoroscopy. The osteotomy was oriented approximately 30 degrees to the axis of the fibula, starting distal on the anterior aspect of the fibula approximately 5 mm proximal to the joint line and continuing to a proximal posterior exit point (Figure 2C). The tibiofibular syndesmosis was released by cutting the anterior and posterior inferior tibiofibular ligament attachments to the distal part of the fibula. The intraosseous part and the syndesmosis proximal to the osteotomy was left intact. The distal part of the fibula was confirmed to be mobile using fluoroscopy and manual displacement. Finally, the deltoid ligament complex’s superficial and deep anterior parts were sectioned, keeping only the dPTTL intact. In step 3, anatomic reduction and plate fixation of the fibula osteotomy was done using an EVOS lateral distal fibula 3.5-mm, 7-hole locking plate (Smith & Nephew, Watford, England, UK). All screw holes were used in every case, securing a stable fixation. All injuries and repairs were made while the specimen was securely fixed to the test rig, and the specimen was not detached between the biomechanical tests, ensuring that the placement of the specimen was the same for each test.
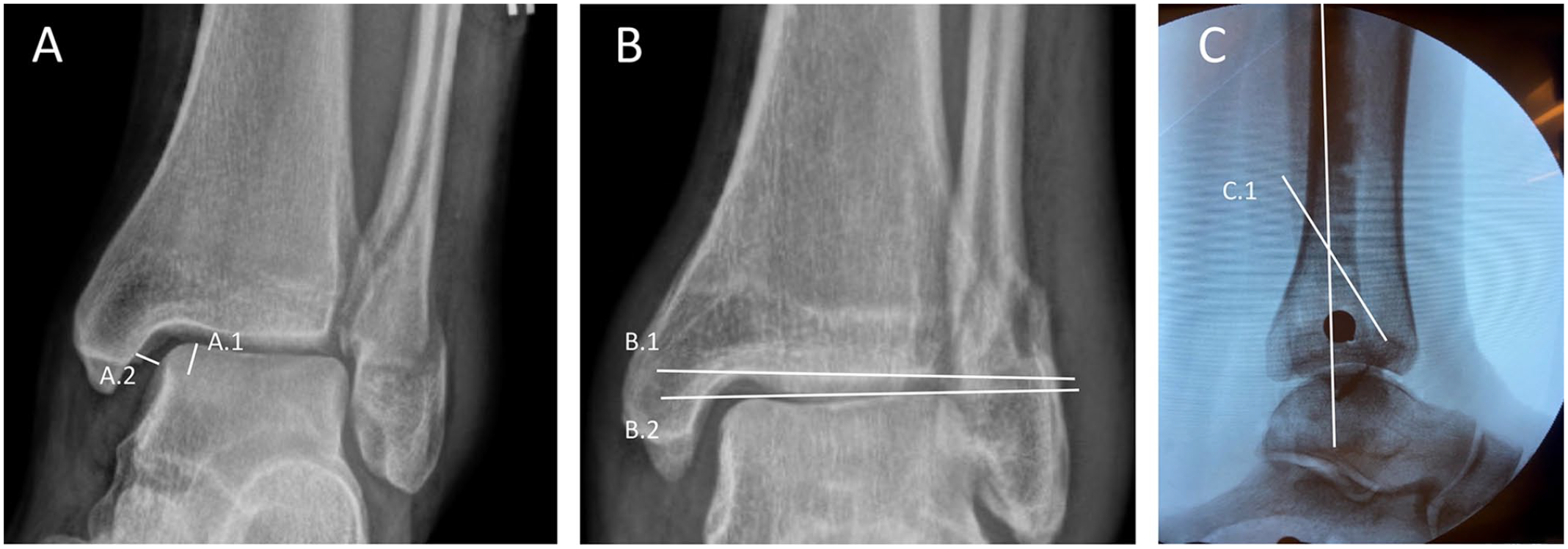
The figure shows the method for obtaining talar shift and talar tilt measurements from mortise view projections in (A) lateral translations and (B) valgus tests. (A) Additionally, the figure shows the orientation of fibular osteotomies (C). For talar shift, we marked a 5.0-mm distance starting at the talar dome and caudally (line A1). Then, talar shift was measured as the shortest distance between the medial border of the talus and the lateral border of the medial malleolus 5.0 mm below the talar dome (line A.2). (B) Talar tilt was measured as the angle between the articular surface of the tibial plafond (line B.1) and the articular surface of the talar dome (line B.2). Fibular osteotomies were oriented approximately 30 degrees to the axis of the fibula, starting distal on the anterior aspect of the fibula approximately 5 mm proximal to the joint line to proximal posterior (line C.1).
Outcomes
The primary outcome was the difference in radiographic talar shift (millimeters), measured at neutral ankle position, for SER4a injury models with plate fixation, compared to SER4a injury models without plate fixation. Talar shift was calculated as the medial clear space (MCS) recorded on mortise view radiographs. Consistent with previous descriptions,5,10 we defined the MCS as the distance between the talus’s medial border and the medial malleolus’s lateral border on a line parallel to and 5.0 mm below the talar dome, as shown in Figure 2.
Secondary outcomes included the difference in radiographic talar valgus tilt (degrees), robotic measurements of lateral translation (millimeters), valgus (degrees), and internal and external rotation (degrees) comparing SER4a injury models with plate fixation with SER4a injury models without plate fixation, and SER4a injury models with plate fixation with intact ankles. Talar tilt was measured as the angle between the tibia’s distal articular surface and the talus’s superior articular surface (see Figure 2).
Radiographic measurements were obtained using Sectra IDS7, version 23.2 (Sectra AB, Sweden).
Statistical Analysis
Descriptive statistics were presented using means and corresponding SDs. In addition, 95% CIs were calculated under the assumption of normality. Normality was tested using the Shapiro-Wilk normality test and investigated by visual inspection of histograms for each combination of subgroup and outcome. For most subgroups, the results did not indicate significant deviance from normality. We used linear mixed models with random intercepts on study specimens to account for data dependency when testing for pairwise differences in means between groups. We considered this a descriptive study without formal hypothesis, and no power analyses were done a priori. All analyses were done using Stata, version 17.0 (StataCorp, College Station, TX).
Results
Specimens
On specimen dissection, it was found that 2 had significant ankle osteoarthritis and 1 had major arthrofibrosis, implying previous ankle trauma. These 3 specimens were excluded, leaving 15 to be analyzed. Of these, 7 were female (46.7%), and 7 were right ankles (46.7%). The average age at death was 71.3 years (range 55-87 years).
Biomechanical Tests
All measurements with SDs are available in Table 1.
Stability Measurements of 15 Ankles Tested Sequentially as Native, SER4a, and SER4a With Plate Fixation. a
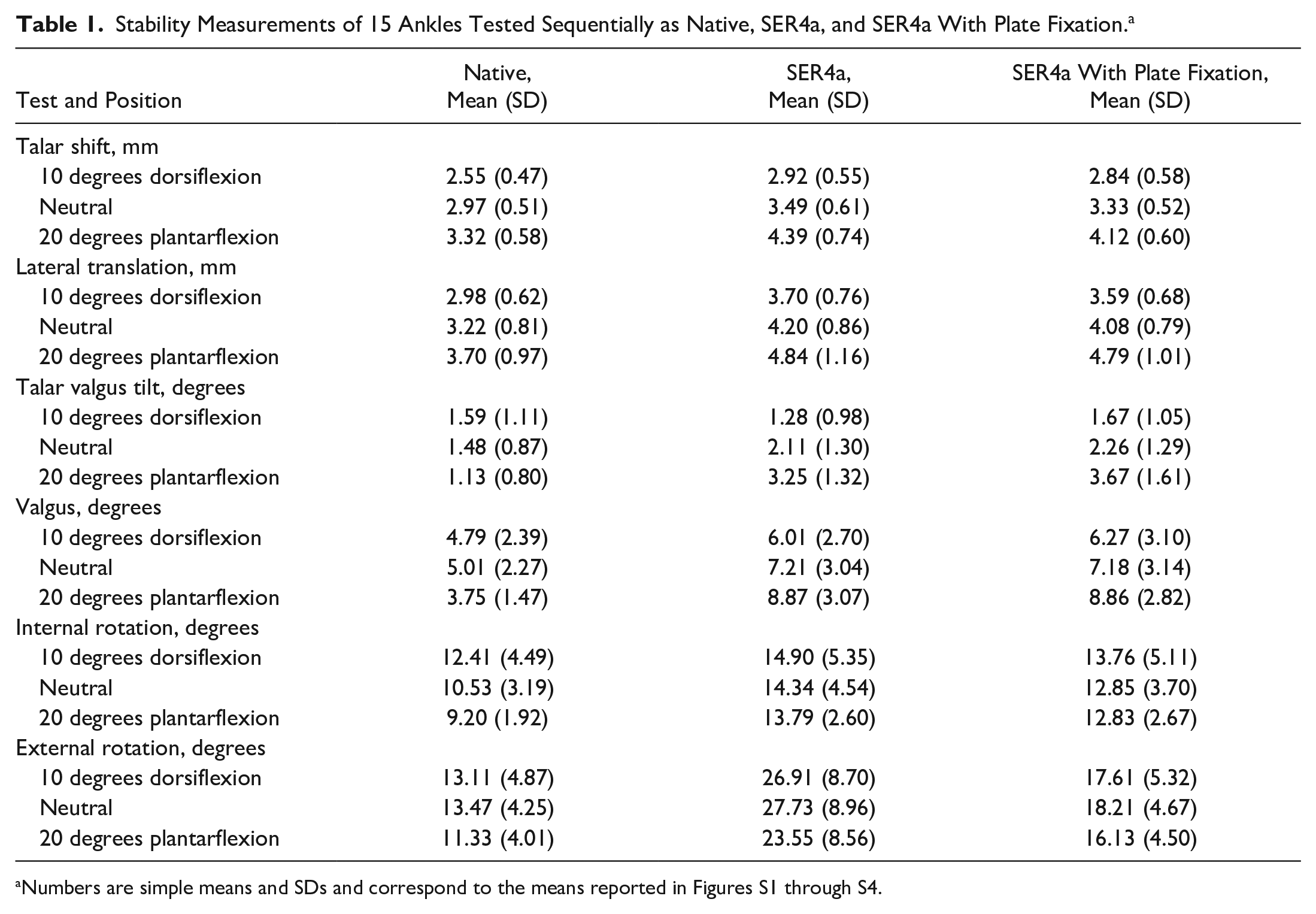
Numbers are simple means and SDs and correspond to the means reported in Figures S1 through S4.
Comparing SER4a injury models with plate fixation and SER4a injury models without plate fixation, lateral translation and valgus tests showed that plate fixation only led to minor stability improvements (see Figures S1 and S2). At neutral ankle position, the mean difference was −0.16 mm (95% CI −0.33 to 0.01 mm, P = .071) for talar shift and −0.15 degrees (95% CI −0.01 to 0.30 degrees, P = .068) for talar tilt. The only statistically significant improvement was seen in measurements of talar shift at 20 degrees of plantar flexion but with a small magnitude improvement at mean −0.27 mm (95% CI −0.48 to −0.06 mm, P = .010). Significant improvements were observed for external rotation when tested in dorsiflexion, neutral, and plantarflexion, with degrees ranging from −7.43 to −9.52 degrees (P < .001 for all comparisons) (see Figure S3). Internal rotation also showed significant improvements (P < .001 for all comparisons), but the magnitude of the stability increase was smaller, ranging from −0.96 to −1.49 degrees (see Figure S4).
When comparing SER4a injury models with plate fixation and intact joints, all comparisons significantly differed from intact joints (see Table 2). The only exception was talar tilt measured at 10 degrees ankle dorsiflexion at 0.12 degrees (P = .424). All comparisons with mean differences, 95% CIs, and P values are presented in Table 2.
Stability Differences in 15 Ankles Comparing SER4a Models With Plate Fixation to SER4a Models, and SER4a Models With Plate Fixation to Native. a
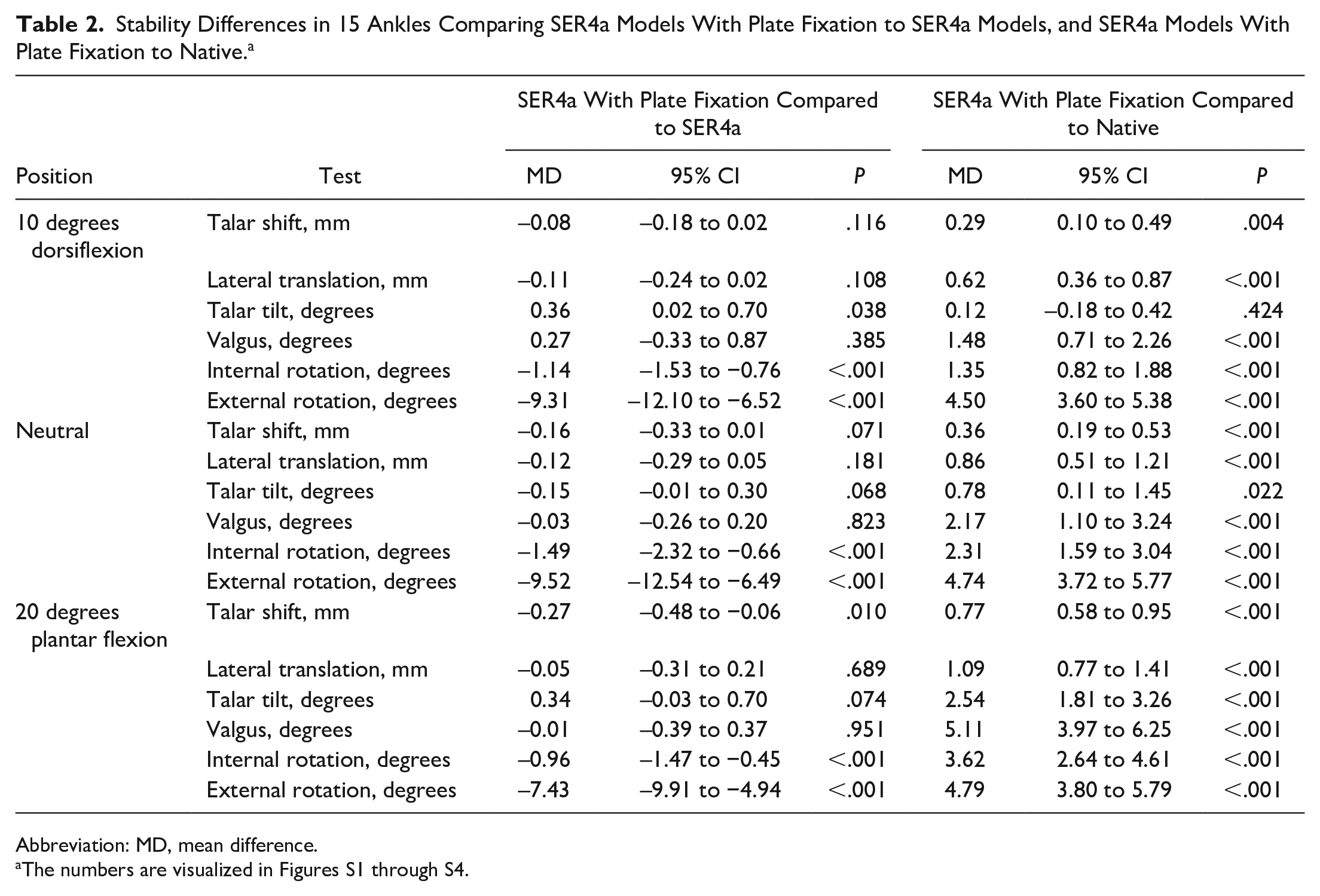
Abbreviation: MD, mean difference.
The numbers are visualized in Figures S1 through S4.
Discussion
The main finding of this study was that anatomic reduction and plate fixation of the fibula osteotomy did not considerably enhance the ankle stability of SER4a injury models without plate fixation regarding lateral translation and valgus stability. However, our findings demonstrated that fibular plate fixation significantly improved external rotational stability. To our knowledge, this is the first study to evaluate the biomechanical effect of plate fixation in SER4a injury models.
Biomechanical data on the stability of Weber B fractures with partial deltoid ligament injury is scarce. A previous study demonstrated that external rotation instability already occurs to some degree in cadaver models with no medial side injury (Weber B/SER2 injury models). 2
Clinical Relevance
The reason for operative treatment of Weber B/SER fractures with an injured deltoid ligament, including both SER4a and SER4b fractures, is that they are unstable on both the lateral and medial side (bimalleolar-equivalent). The traditional practice has been to restore stability on the lateral side using screw and plate fixation of the fibula to improve ankle stability, ensure anatomical healing, and prevent posttraumatic arthritis caused by changes in joint kinematics. 4 However, recent biomechanical evidence suggests that Weber B fractures with a partial deltoid ligament tear but with an intact dPTTL are stable.2,9 These findings are coherent with clinical studies demonstrating acceptable patient-reported and radiographic outcomes in the short and midterm after nonoperatively treating SER4a fractures,4-6,13 and thus challenges the traditional practice of operative treatment of SER4a fractures because of potential instability. The results of the present study provide evidence that plate fixation of the fibula only improves external rotational stability, in SER4a injury models. However, we do not know what the long-term effects of potential decreased external rotation are.
Limitations
Although ankle fractures take distinct patterns and imaging studies have established that the SER mechanism can cause Weber B fractures with a partial deltoid ligament injury, 1 studying cadaver specimens that simulate these injuries cannot accurately capture the intricacies and variations of injuries that occur in vivo. By necessity both the orientation of the fracture line and the amount of deltoid injury were highly controlled. Although this has strong scientific advantage by reducing confounders, clinical relevance can be rightly questioned. Additionally, this study does not address diagnosis of SER4a vs SER4b and may be viewed as a limitation and a target for future research. Another limitation was that robotic measurements were obtained over the ankle and subtalar joints, whereas only radiographic measurements could assess isolated tibiotalar stability. The study setup allowed radiographic measurements for lateral translation and valgus tests but could not accurately measure isolated instability in the ankle joint when testing rotations. Although our study’s findings offer valuable insights into the effect of plate fixation on SER4a injury model stability, the effects and clinical relevance of predetermined loading amounts, safety margins, loading positions, and testing orders remain unknown. Acknowledging that this is a descriptive study, we did not conduct an a priori power analysis, which should be regarded as another weakness of this study.
Conclusions
The findings of this study indicate that anatomic reduction and plate fixation of the fibular fracture increase external rotation stability compared with no fixation. However, in this robotic cadaver model, plate fixation did not fully restore native ankle stability after the Weber B/SER4a fracture pattern.
Supplemental Material
sj-jpg-2-fai-10.1177_10711007241235903 – Supplemental material for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning
Supplemental material, sj-jpg-2-fai-10.1177_10711007241235903 for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning by Martin G. Gregersen, Andreas F. Dalen, Aleksander L. Skrede, Øystein Bjelland, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-jpg-3-fai-10.1177_10711007241235903 – Supplemental material for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning
Supplemental material, sj-jpg-3-fai-10.1177_10711007241235903 for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning by Martin G. Gregersen, Andreas F. Dalen, Aleksander L. Skrede, Øystein Bjelland, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-jpg-4-fai-10.1177_10711007241235903 – Supplemental material for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning
Supplemental material, sj-jpg-4-fai-10.1177_10711007241235903 for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning by Martin G. Gregersen, Andreas F. Dalen, Aleksander L. Skrede, Øystein Bjelland, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-jpg-5-fai-10.1177_10711007241235903 – Supplemental material for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning
Supplemental material, sj-jpg-5-fai-10.1177_10711007241235903 for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning by Martin G. Gregersen, Andreas F. Dalen, Aleksander L. Skrede, Øystein Bjelland, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241235903 – Supplemental material for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning
Supplemental material, sj-pdf-1-fai-10.1177_10711007241235903 for Effects of Fibular Plate Fixation on Ankle Stability in a Weber B Fracture Model With Partial Deltoid Ligament Sectioning by Martin G. Gregersen, Andreas F. Dalen, Aleksander L. Skrede, Øystein Bjelland, Fredrik A. Nilsen and Marius Molund in Foot & Ankle International
Footnotes
Ethical Approval
The Regional Committee for Medical and Health Research Ethics approved the study (ref. 178067).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Østfold Hospital Trust and the South-Eastern Norway Regional Health Authority (grant 2023014).
ORCID iDs
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.