
Abstract
The experience of a patient’s death on medical students is powerful and may entail distress and anxiety. We review the experience of death and dying as perceived by medical students. Students are exposed to death and dying while dissecting cadavers in pre-clinical years, following patient death in clinical years, and commonly as a result of personal exposure. Students report sadness and anger in response to patient death, particularly following their first experience. The patient’s identity and the student’s past exposure to death were found to influence the way students experience death and dying. Coping methods may include conversation, reflection, and religion as well as detachment and avoidance. Although time and resources are invested in preparing students for a patient’s death, many of them feel inadequately prepared. Greater understanding of and investment in processing medical students’ experience of patient death may be helpful in their personal and professional development.
Introduction
In most medical specialties, exposure to death and tragedy is inevitable.1,2 Physicians are expected to continue acting professionally amidst the emotional turmoil of experiencing a patient death. 3
Studies have focused on the care team’s response to patients’ death, primarily that of physicians. However, over the last 15 years, the student’s perspective has received more attention. Students experience difficulty facing patient death, occasionally accompanied by a feeling of helplessness. For many, this will be their first in-person exposure to death and dying and the experience may color their professional future.
Previous publications focusing on the students’ experience of death and dying commonly include the following subjects: End-of-life (EOL) education, students' experience and emotional response, coping strategies, and the effects of unprocessed feelings. Most of these publications are limited in depth or in scope, focusing on one or two of the themes listed above. A review of death and dying as experienced by medical students is therefore necessary.
Materials and Methods
We conducted a narrative review of the literature addressing EOL education and students’ experience of patient death. To that end, we searched PubMed for peer-reviewed, English language articles published between 1990 and March 2023, using the key terms ‘medical students’, ‘patient death’, ‘end-of-life’, or ‘coping strategies’, in several variations. We first read the abstracts and excluded articles which mainly discussed the clinical aspects of EOL. Key articles which shed a new light on the research field in the different periods were selected. Subsequently, we reviewed the references lists of these articles and identified additional papers. A total of 72 articles were selected for review.
Results
Medical Students’ Exposure to Death and Dying
Patient loss during clinical years is not the first time a medical student encounters death in his or her studies. This most commonly occurs during pre-clinical years while dissecting cadavers in the anatomy lab. The experience of dissecting a human body may provoke a powerful emotional and stressful response in students.4,5 However, students may experience peer-pressure and avoid acknowledging or expressing their emotional distress and anxiety. This hidden curriculum may lead to a casual outlook upon death and dying which may affect their future professional identity as doctors. 6
Medical Students’ Experience of Patient Death
The experience of a patient death, however, is an experience distinct from prior exposure to death and dying. Students experience patient death in the various ways.
Personal Emotional Response
Patient death has a major emotional impact on health care practitioners in general, and medical students in particular, leading to deep seated memories that remain with them for a long time.7,8
Many students experience distress and anxiety in response to a patient’s death, 9 sometimes even in cases where they had no personal connection to the deceased. 10 These emotions may include sadness, anger, guilt 11,12 and shock.7,13,14
These emotions may also trigger traumatic memories. The most powerful memories are those linked to the basic senses; sounds, smells, and sights. Many students report remembering a dead patient's skin color 7 and the voices of their family heard from the hallway. 10 The most memorable death among medical students is that of their first patient. 15
Patient characteristics have a crucial impact on the emotional reaction of medical students. Universally, students perceive the death of a young child as unjustified, 16 and when it occurs, they experience significant emotional distress. Children are naturally perceived as innocent and weak, which elicits the need to protect them. 11 Conversely, the death of elderly patients, particularly when suffering from severe or chronic diseases, is more commonly perceived as a natural event. 16
Another factor thought to influence the emotional experience of the students is the personal connection with the patient 17 and his family, a phenomenon also common among senior staff. 16
Death of a Loved one
It has been suggested that healthcare provider’s personal experience and life circumstances may influence the way they face EOL issues.18,19 Many medical students have previously experienced the death of a relative or friend20,21 even prior to medical school, with reports ranging from 29% to 99%. 12 A personal loss may indeed be a source of motivation to becoming a physician. 22 When treating dying patients, this motivation may lead to complex emotions, which can manifest in several ways. Exposure to dying patients may evoke previous experiences of bereavement and cause stress and anxiety.21,23 Students may actively avoid situations involving death and dying. 23 When caring for patients with characteristics similar to that of a deceased relative or friend, students report difficulty interacting with the patients and their families.7,15,20 This may result in communication avoidance, culminating in a distant relationship 21 which may harm students’ satisfaction in their own professional role. 24
In contrast, some studies suggest that in cases when students had properly processed their emotions following a personal loss, they benefited both professionally and personally 21 and were more likely to regard EOL care positively. 25 In some studies, students who had personal experience with death felt more comfortable treating dying patients, communicating with the family and supporting them, 9 and were more realistic regarding patients’ needs and emotions. 26
Death as a Professional Failure
Beyond their personal response, students may also experience feelings of professional failure. After patient death, some students report fear that their knowledge is inadequate, that they had exercised bad judgment, 16 or acted incorrectly. 7 Cases of unexpected death, 17 as well as cases where errors of judgment may have contributed to the patient’s death, may increase the students’ distress. 11 While these experiences are common among physicians, the early professional identity of medical students is affected as well. 27
In the past, the overarching goal of the physician was death prevention, and therefore the occurrence of death was considered a failure.28,29 This approach is still present, especially among veteran doctors. 7 However, medical culture has shifted. Physicians are now expected to alleviate pain and suffering and adapt treatment to the patient’s goals of care.30–32 This perceptual change has permeated into medical school curriculum and culture 11 and consequently, the majority of students today do not perceive death as a professional failure.11,33,34 Notable exceptions are cases in which human error has occurred which may have contributed to the patient’s death. 11
Coping Strategies
Conversation
Open conversation is a common coping strategy among medical students.7,35 In addition to providing emotional comfort,9,10,17 conversations contribute to students’ professional development. 9
Students prefer to talk with friends or family rather than with physicians,17,35 since they feel free to express their thoughts and emotions without concern of academic and professional evaluation 9 and judgement. 36 Moreover, when the conversation takes place outside the hospital environment, the students’ perspective expands beyond the academic and professional aspects. 36 For their part, physicians tend to avoid discussions with students about patient death. When such conversations do occur, clinical rather than emotional aspects are commonly addressed. 7
Physician support of medical students experiencing patient death may influence the manner in which medical students respond to EOL situations. 37 Many students do not feel emotionally supported by attending physicians, compounding the difficult emotions they experience. 13 In some cases, students who cried in response to intense emotional situations were met by ridicule or contempt from physicians. 38 In contrast, when senior physicians expressed empathy toward dying patients and empathy for the students’ emotional responses, the students experienced significant relief 11 and were appreciative.7,35 This illustrates the importance of role modeling and the hidden curriculum in medical education. 37
Reflection
Reflection is a central component of professionalism and an essential skill for both the personal and professional development of physicians. 39 Among others, the General Medical Council of the UK has emphasized the significance of physicians cultivating coping strategies, including reflection, in their clinical practice to ensure their well-being. 40 Reflection also has importance in the development of medical students’ professional identity. 41
Students who utilized reflective practice as a coping strategy found that it increased their confidence and comfort with EOL situations. Reflection enabled students to explore and examine their emotions and responses, to learn from their experience 42 and to develop their professional identity. 36
Distraction
Hobbies are correlated with a lower risk of burnout among students 43 as well as palliative care physicians. 44 In the clinical years of medical school, stress, exhaustion and high-pressure might may decrease the time that can be invested in hobbies. 9 Nonetheless, many students still make a point of adopting hobbies, such as exercise, watching movies and reading, as a coping strategy to relieve stress 37 and provide a helpful distraction from thoughts about death and dying. 7
Religion
Turning to religion is frequent used as a coping strategy among medical students.7,9,11 Spirituality and belief in the afterlife have been found to have an inverse association with death anxiety, and emotional distress. 45 Religious beliefs may help with the acceptance of death, following the view of the limited control over life and the impossibility of changing “god’s will”. Interestingly, students who do not define themselves as religious sometimes embrace religious attitudes to deal with patient death. In addition, some students believed prayer was helpful for the dying patient. 11 According to Firth-Cozens and Field, 46 religious students experienced the loss of a patient as a less stressful event and have a lower risk of becoming afraid of death.
Avoidance
Coping strategies among physicians may also include detachment, avoidance, and emotional withdrawal. 47 A study conducted in 1991 which examined strategies for coping with patient death among medical students, found that “the most frequently used strategy was that of passive acceptance, which entailed accepting, rationalizing and assimilating the event into one’s everyday work performance”. Only 21% of the participants talked to people for support. 46
Although patient death is a powerful experience, doctors and students’ professional duties are essential.7,46 Engaging in different tasks allows to focus on rational aspects and reduce emotional preoccupation with death and dying. However, accepting and internalizing events are vital as well, 11 and a balance is necessary. Some students choose to stay busy and focus on their ward tasks, 7 focusing on their professional identity in assisting other patients. 11 Other students carry on with their clinical responsibilities to avoid an emotional response. 17
Following a patient’s death, some students choose to avoid their emotions, 17 allowing them wane with time. 46 Others prefer to discuss their experience only at the clinical level. 36 In other cases, students avoid or deny the loss, as they believe that any discussion or thoughts about death and dying are neither necessary or helpful. 46
The Importance of Experience Processing
The importance of processing the feelings that emerge following an emotionally powerful experience is recognized in the literature,48–50 and accordingly is practiced in various medical education programs.
Students who do not come to terms with their feelings after patient death, may see their emotional response as unprofessional. 10 They may therefore be exposed to a higher risk of distress and burnout, 51 and more frequently become cynical physicians. 52
Caregiver burnout is “a work-related syndrome involving emotional exhaustion, depersonalization and a sense of reduced personal accomplishment”, 53 which may lead to reduced effectiveness at work. 54 Burnout was found to be a prevalent phenomenon among medical students as well as practicing physicians.55,56
Physically and emotionally exhausted students, with unrecognized and unresolved emotional issues, will likely find communication with patients and families more difficult 57 Additionally, they will commonly experience difficulty in supporting the dying patient and their family. 20 On the other hand, when emotional processing is conducted appropriately, students may improve the quality of care they provide. 58
Preparation for the First Experience of Patient Death
The subject of patients’ death is of great interest to many medical students 59 and is a major concern to many of them in the transition to clinical years. 60
Until the early 1990's, formal EOL training in medical schools was relatively scarce. 20 The Institute of Medicine published a report in 1997 that determined that physicians are not trained properly to provide satisfactory EOL care, and therefore recommended that “Educators and other health professionals should initiate changes in undergraduate, graduate, and continuing education to ensure the practitioners have relevant attitudes, knowledge, and skills to care well for dying patients”. 58
Over the years, more EOL and palliative care training has been integrated into the curriculum of medical schools, 61 and yet in many programs EOL education is not sufficient. 62 Although the number of EOL courses has increased over the last decade63,64 and pre-clinical and clinical education have improved students’ confidence in treating dying patients, 65 students still feel inadequately prepared to deal with patient death.17,35,66 Some students have difficulty coping with patients’ fear of dying and death, and struggle to support grieving families.11,33 A possible explanation for the students’ feeling of unpreparedness is that EOL training is often conducted through lectures and rational philosophical discussion, 67 whereas the experience of a patient death is primarily emotional. 11 This gap may cause tension between pre-clinical EOL education and the students’ emotional response 10 causing some students to believe that medical school cannot properly prepare them for patients’ death 35 or EOL care, which to their mind, can only be learned by experience. 16 Indeed, young doctors report a lack of exposure to dying patients with palliative care needs during their medical school training. 68 Notably, some institutions have attempted to incorporate student interactions with patients with palliative care needs during pre-clinical years, which made them feel more comfortable discussing EOL issues.36,41,42,69 In addition, a recent study found that medical students highly value the discussion on the process of death and dying during pre-clinical years, and perceive it as important to the practice of medical profession. 34
Discussion
The perception of patient death has changed in the medical field, a change which is reflected in each aspect of the experience; preparation, comprehension of the event, and coping with the emotions following it. The change in the preparation phase is reflected in the curriculum content and the time devoted to EOL education in medical schools. However, despite the increased resources invested in the field, studies suggest that many students still feel inadequately prepared to deal with patients’ death. Some medical schools have adopted a first-hand experience-based approach to EOL learning. In studies of curricula where students were exposed to a dying patient during pre-clinical years, they reported a more positive attitude towards EOL care.
Although students’ background may influence the way they experience patient death and should be taken into consideration, studies that deal with the impact of life circumstances on the experience of the event are scarce. Prior exposure to death may have either positive or negative impacts on the student’s ability to process death. One determining factor may be whether this event was appropriately processed prior to the medical school years.
Studies from the last decade have found that students do not see a patient’s death as a professional or personal failure. Additionally, they perceive their emotions as a natural reaction. Students use different strategies to cope with a patient’s death. Efforts should be made to promote helpful methods of processing these experiences.
The attention given by doctors to student’s experiencing death is crucial as role modeling has a central role in the students’ perception of the clinical practice. In some cases, post patient death discussions do not occur, or are only focused on the clinical aspect. Those doctors' attitude towards the event probably stems from the fact that they were educated in an environment which avoided discussion about death and the emotions that followed it.
The first death a medical student experiences during medical school is during pre-clinical years, in the anatomy lab. The coping strategy chosen by students carries importance, as it represents an initial experience that will persist and shape their professional identity. Indeed, studies that examined the emotional response and coping strategies of senior doctors to patients death showed similar results to those of students (Figure 1).18,70–72 Thus, we suggest that the coping strategies used by doctors began to take shape at the beginning of their training, as students. Therefore, it is crucial for medical schools to anticipate and integrate EOL courses already in the pre-clinical years, prior to the student’s first encounter with death (Table 1).
Our study encompasses several limitations to be considered. First, the review is narrative in nature, which inherently cause a level of subjectivity in the selection and interpretation of the literature. Additionally, some of the papers included in our review are relatively old. Nonetheless, this serves our aim of exploring how medical students’ perceptions and coping strategies regarding patient death have shaped and evolved over time.
Furthermore, we included a variety of article types without focusing on specific study designs or methodologies, which might affect the consistency of our conclusions.
In conclusion, the medical world is currently undergoing a process of modifying its perception of experiencing a patient’s death. Consequently, students will most likely encounter a variety of responses from doctors, who are also experiencing this change themselves. It is essential to be aware of this in order to avoid adopting non-optimal behavioral mechanisms which may harm the student’s well-being and therefore patient treatment. Abbreviation: EOL, end-of-life. Figure 1: Medical students are exposed to death at various stages in their training. Some of them lost a relative prior to medical school, all of them are exposed to death as part of the anatomy labs, and in the clinical years they will encounter the death of a patient. In each of these situations, the student develops strategies for dealing with the emotions that arise from it. End-of-life (EOL) courses, in clinical and pre-clinical years, can help students develop coping strategies that benefit their well-being and their professional identity development. Coping strategy adoption is also affected by the behavior of the senior doctors in response to the death of a patient. In many cases, the student’s chosen coping strategies may remain unchanged or fixed. Therefore, it is crucial for students to develop a beneficial coping strategy during the early stages of their professional identity development. As initial exposure to death during studies occurs in the anatomy lab, EOL education should be integrated prior to clinical training. Recommendations for Improving Student’s Experience of Patient Death.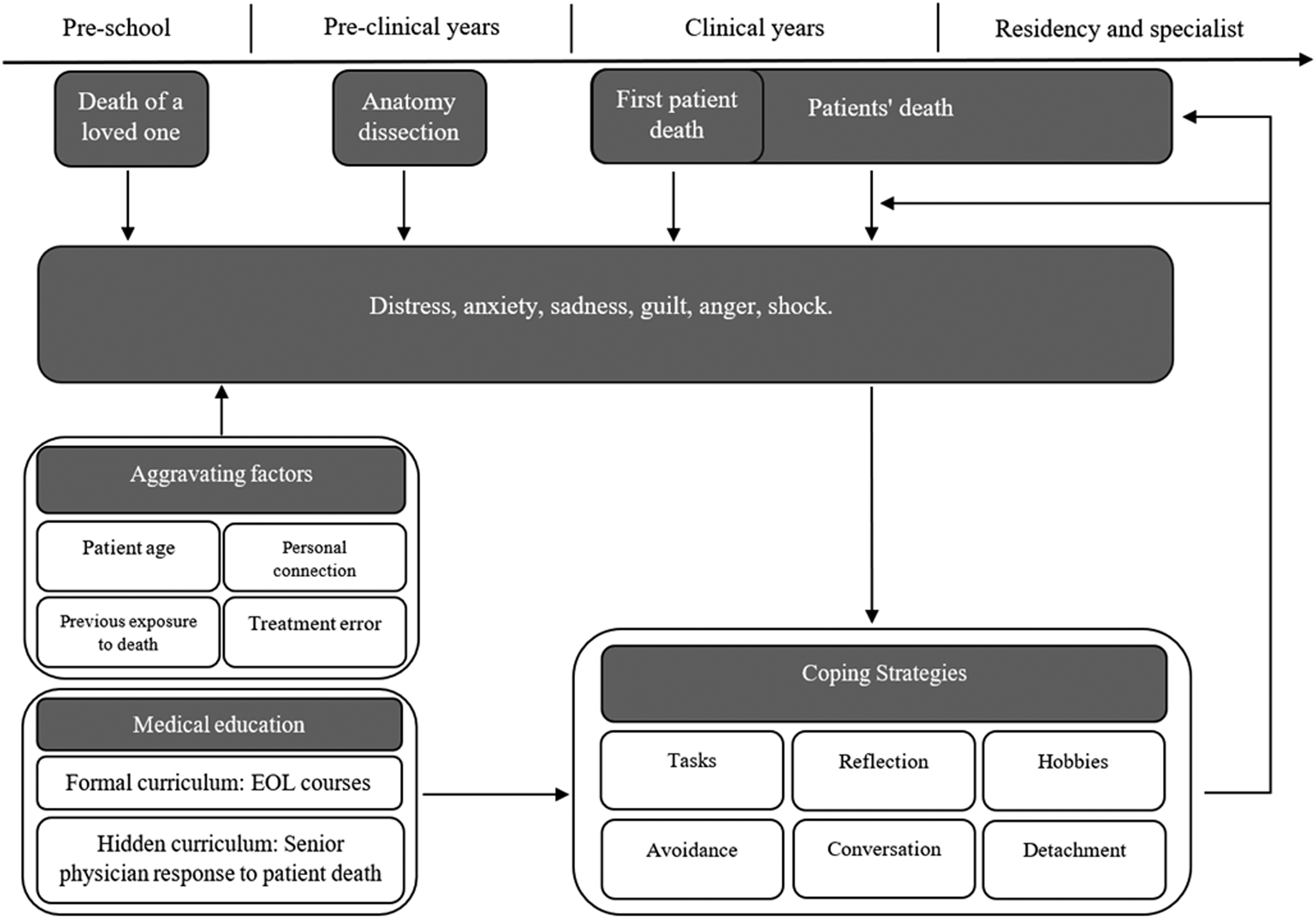

Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.