
Abstract
Background:
Patients with advanced non-small-cell lung cancer (NSCLC) frequently experience severe symptoms and functional decline, underscoring the need for early end-of-life (EOL) care discussions to improve care quality. Additionally, enhancing patients’ death literacy may strengthen these discussions. However, how patient characteristics influence death literacy in this population is largely unknown.
Objective:
This cross-sectional study explored baseline levels of death literacy and examined associated patient characteristics in advanced NSCLC.
Design:
A cross-sectional study was conducted.
Methods:
A total of 103 patients aged ⩾18 years with stage IIIB or higher NSCLC who had completed at least first-line cancer treatment were recruited using convenience sampling. Data were collected between June 2024 and June 2025 using structured questionnaires assessing sociodemographic, medical conditions, prior EOL care experience, and death literacy (using the traditional Chinese version of the Death Literacy Index, score range = 29–145). Descriptive statistics, Pearson’s correlation, independent t test, and stepwise regression were used to analyse associations between patient characteristics and death literacy.
Result:
The mean participant age was 61.62 ± 10.86 years, and the mean Karnofsky Performance Score was 67.57 ± 12.48. Many had prior experience of EOL care provision (58%) and had lost a relative (90%), but few had discussed EOL care with a physician (29%). Overall, death literacy was moderate (94.08 ± 16.45). Higher death literacy was significantly associated with experience of EOL care (β = 13.390, p < 0.001), having had an EOL care discussion with a physician (β = 10.901, p < 0.001), and being a women (β = ‒8.671, p = 0.001). These factors explained 37.1% of the variance in death literacy (F = 21.030, Adjusted R2 = 0.371).
Conclusion:
Healthcare providers should recognize patients’ lived experiences as important contributors to fostering open conversations around EOL care preferences. Interventions such as the Life Journey Tea House or broader public health strategies may help stimulate reflection and encourage dialogue.
Plain language summary
Patients with advanced non-small cell lung cancer (NSCLC) experience severe cancer-related symptoms and functional limitations, which makes end-of-life (EOL) care decisions more complicated. In a study with 103 patients hospitalized in Northern Taiwan, we asked about their backgrounds, health, and experience with EOL care. We also measured their “death literacy,” meaning how much they know and feel confident about understanding and discussing death. We found that patients who had cared for someone at the end of life, had discussed EOL care with a doctor, or being women demonstrated higher death literacy. These three factors contribute to the knowledge and skills required to understand, access, and make informed decisions about end-of-life care and death. Highlighting that direct, personally lived experiences of EOL care situations helps people feel more comfortable talking about death. Healthcare providers should use these experiences as chances to start important conversations. We suggest that public initiatives—such as Life Journey Tea House, online educational programs, and massive open online courses—may help stimulate reflection and foster meaningful dialogue about death and dying.
Introduction
According to the latest global cancer epidemiological report, lung cancer remains one of the most common and deadliest cancers worldwide, with approximately 2.48 million new cases and 1.8 million deaths reported in 2022, highlighting its significance as a global public health challenge. 1 The high incidence and mortality rates of lung cancer are also observed in Taiwan. According to the 2022 Taiwan Cancer Registry, lung cancer accounted for 17,982 newly diagnosed cases, 2 in the same year, lung cancer accounted for 10,053 cancer-related deaths, making it the leading cause of cancer mortality in Taiwan. 3
Non-small-cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer diagnoses, with approximately 60% of the patients at their advanced and incurable stage at diagnosis. 4 Evidence suggests that patients with advanced NSCLC have very limited survival, with the overall 5-year survival rate for NSCLC remaining poor, ranging from approximately 68% in patients with stage IB disease to as low as 0%–10% in those with stage IVA–IVB disease. 5 Evidence suggests that the high mortality rate in this population is associated with both the aggressive nature of the tumour and delayed diagnosis. 6 Moreover, patients with advanced NSCLC experience severe cancer-related symptoms and functional limitations compared with those with other cancers, which complicate the goals of end-of-life (EOL) care. 7 This highlights the important and urgent need to initiate early discussions about the goals of EOL care for advanced NSCLC patients for better healthcare outcomes. 8
‘Death literacy’ was proposed by Noonan et al. in 2016 and defined as ‘a set of knowledge and skills that make it possible to gain access to understand and act upon end-of-life and death’. 9 High-quality care for patients with advanced NSCLC involves early integration of palliative care and enhancement of death literacy.10,11 Engaging in advance discussions and planning regarding EOL care goals has been shown to improve symptom management and goal-concordant care during EOL care. 12 Previous research shows that death literacy is associated with an individual’s reflections on their own EOL care preferences. 13 In Taiwan, the National Health Research Institute emphasizes the importance of improving public death literacy as a key objective in the development of palliative care, as outlined in the 2019-White Paper on Hospice and Palliative Care Policy. 14 However, the concept of ‘death literacy’ has not yet been widely introduced or adopted in Taiwanese society, particularly among patients with cancer.
To the best of our knowledge, evidence regarding advanced NSCLC populations remains scarce. Patients with advanced NSCLC are more likely to suffer from severe cancer-related symptoms and life-threatening complications, 7 making them a vulnerable population with a high risk of mortality. Better death literacy might enable them to express their EOL care preferences more clearly, leading to better symptom management and goal-concordant care during EOL. It may also help them identify deficiencies in specific dimensions, thereby facilitating the design of appropriate interventions and resources. This study serves as an initial investigation into death literacy among people with advanced NSCLC, aiming to explore the baseline performance of death literacy and its associated factors in this patient group.
Materials and methods
Study design
This study is part of a larger project aimed at exploring the association between death literacy in patients with lung cancer and their life-sustaining treatment preferences. This article reports baseline data on death literacy performance and its influencing factors. This study adopted a cross-sectional correlational design using structured questionnaires to collect data from patients with advanced NSCLC who were hospitalized in a medical centre in Northern Taiwan (Figure 1). The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist was used for reporting (Supplemental Material). 15

Research framework of factors influencing death literacy.
Study setting and sampling
This study was conducted in a 37-bed Chest Medicine ward at a single national medical centre in Northern Taiwan from June 2024 to June 2025. The National Taiwan University Hospital provides a comprehensive range of specialty and subspecialty services, with more than 2300 beds and over 7500 staff members, and serves as one of the largest medical centres in Northern Taiwan. We adopted convenience sampling and recruited patients aged ⩾18 years with cancer stage IIIB or higher who had completed at least first-line cancer treatment, to ensure that they had adequate experience with the cancer trajectory and clinical decision-making, which could influence their perspectives on care planning. Participants were excluded if they had (1) primary lung cancer with brain metastases that impaired their consciousness status, comprehension, or expression; (2) could not communicate or read fluently in Mandarin or Taiwanese; or (3) were diagnosed with multiple types of cancer (i.e. two or more distinct primary cancers), to reduce potential sample heterogeneity and confounding effects.
The effect size was estimated using Cohen’s f 2 method, 16 and based on preliminary data from the larger project, yielding an effect size of f 2 = 0.324. The minimum sample size was determined using G*Power version 3.1.9.2 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). Assuming an effect size of f = 0.324, α = 0.05, power = 0.80, and 11 predictors, the minimum sample of 63 participants was estimated to be necessary to achieve the required statistical power. Accounting for a potential attrition rate of 20%, 17 at least 76 participants were deemed necessary.
Data collection process
The first author (G.-F.L.) screened patients in the Chest Medicine ward for eligibility by reviewing their electronic medical records and informed the treating clinician about potential candidates. Eligible patients were then verbally invited to participate in the study. To ensure data completeness, the first author, serving as the interviewer, provided a detailed explanation of the study to the participants and addressed all their questions. Participants were provided with at least 24 h to consider their participation. Written informed consent was obtained from all participants prior to scheduling the interviews. The consent form included information on the study’s purpose and methods, as well as the inclusion and exclusion criteria, participants’ rights, confidentiality, and provisions for distress protocols. The interviews were conducted based on the participants’ preferences, including the choice of time and location (i.e. ward, lounge, or consulting room). Most of the participants were able to complete the questionnaire independently. Some participants with difficulties in reading or writing due to poor physical condition or the presence of medical devices (e.g. peripheral venous catheters, oximeters, and oxygen devices) required assistance; hence, the interviewer read each question and recorded the participants’ responses. A voucher equivalent to NTD 200 (approximately USD 7) was provided to the participants to appreciate their time.
Measurements
Data were collected using structured questionnaires consisting of the traditional Chinese version of the Death Literacy Index (DLI) and participants’ sociodemographic data, medical condition, prior first-hand experience, including sex, age, Karnofsky Performance Score (KPS), survival time after diagnosis (months), marital status, educational status, retirement status, religious beliefs, experiences of EOL care discussions with a physician, experiences of EOL care provision, and experiences of losing relatives, amounting to a total of 11 independent variables.
The DLI developed by Australian scholars, Leonard et al. in 2020, 18 is the first instrument globally created to assess levels of death literacy across populations, communities, organizations, and national systems. It provides valuable insights that inform and improve existing care strategies and policy planning. 13 The original scale was developed in an Australian community setting, 13 and has since been adapted and validated across various countries, including the United Kingdom, 19 Sweden, 20 Turkey, 21 and China. 22 Death literacy is a novel concept in literature, and research on it remains limited. 21 Existing studies primarily focus on the general public, 19 healthcare professionals,17,23 students, 24 caregivers, 25 and community-dwelling people with chronic illnesses. 26 Previous studies have demonstrated that older age, being widowed, retirement status, religious beliefs, death of a relative, and experience of EOL care provision are associated with higher levels of death literacy.18,26,27 The DLI consists of 29 items and four subscales—practical knowledge (eight items), experience knowledge (five items), factual knowledge (seven items), and community knowledge (nine items). All items are rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with a total score ranging from 29 to 145; higher scores indicate greater death literacy.
Considering cultural adaptation and social contextual differences, we adopted the traditional Chinese version translated by Yeh in 2022, 28 who previously recruited 708 community participants for the validation of the DLI. Confirmatory factor analysis demonstrated an acceptable model fit: χ2(369) = 1644.314, p < 0.001, Comparative Fit Index = 0.913, Non-Normed Fit Index = 0.891, and Root Mean Square Error of Approximation = 0.070, indicating that the revised model adequately fit the observed data. Additionally, the overall Cronbach’s alpha coefficient of the translated DLI was 0.938, while the subscales were 0.779–0.939. 28 In this study, Cronbach’s alpha for the traditional Chinese version of the DLI was 0.920, and for the subscales, it was 0.868 (practical knowledge), 0.906 (experiential knowledge), 0.819 (factual knowledge), and 0.756 (community knowledge).
Statistical analysis
Data were analysed using the IBM SPSS Statistics® version 30 (IBM Corp, Armonk, NY, USA). Descriptive analyses, including means, standard deviations, frequencies, and percentages, were used to identify participant characteristics. Distribution indicators of the subscales and the DLI total score showed skewness and kurtosis between +1 and −1, indicating a normal distribution. Bivariate analysis was performed using Pearson’s correlation coefficient for continuous variables and independent t tests for two-group comparisons. Variables that showed significant differences or correlations with DLI scores were subjected to further analysis using multiple linear stepwise regression to examine the most significant factors. Statistical significance was set at 0.05.
Results
Demographics of patients with advanced NSCLC
We approached 110 eligible patients, 103 of whom agreed to participate in the study, with a response rate of 93% (4 were not interested, and 3 were too weak to participate). Participants’ mean age was 61.62 ± 10.86 years (range: 34–83 years), and the mean KPS was 67.57 ± 12.48 (range: 40–90). Among these, 52% were men, 55% had survived for more than 12 months after diagnosis, 59% had an education level below senior high school, 59% were retired, 78% were in a partnership, and 73% had religious beliefs. Additionally, 58% had experience of EOL care provision, and 90% had experience of losing relatives, but only 29% had experienced EOL care discussions with a physician (see Table 1).
Demographic characteristics of NSCLC patients (n = 103).
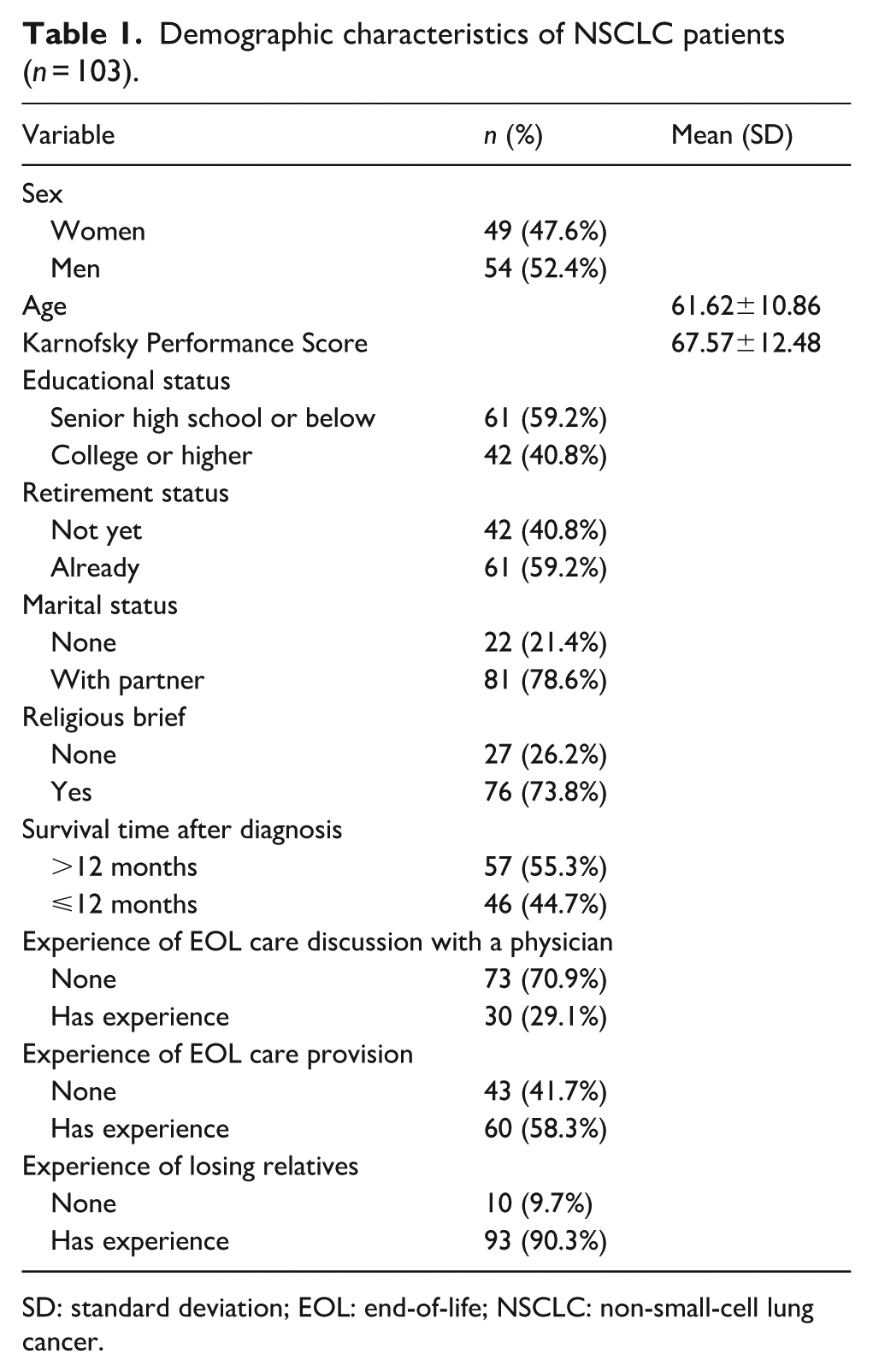
SD: standard deviation; EOL: end-of-life; NSCLC: non-small-cell lung cancer.
Baseline death literacy performance
The average total score of death literacy among patients with advanced NSCLC was 94.08 ± 16.45. The mean scores for the four subscales were as follows: practical knowledge: 27.41 ± 6.63; experiential knowledge: 20.08 ± 4.00; factual knowledge: 23.25 ± 5.28, and community knowledge: 23.34 ± 4.70. The kurtosis and skewness of the scales and subscales were also between +1 and −1, indicating a normal distribution suitable for using the parametric method for statistical analysis (see Table 2).
Mean of subscale dimensions and total death literacy.
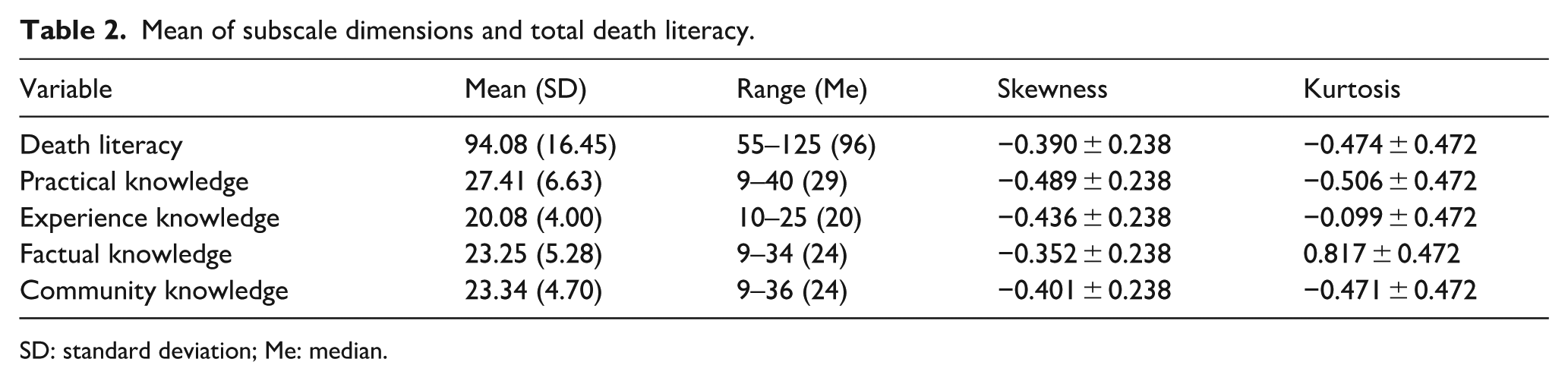
SD: standard deviation; Me: median.
Association between participant characteristics and death literacy
Women demonstrated significantly higher levels of death literacy than men (t = 3.127, p = 0.002), and scored significantly higher on the subscales of practical knowledge (t = 4.055, p < 0.001) and experiential knowledge (t = 2.648, p = 0.009). Furthermore, participants who had experience discussing EOL care with a physician (t = −4.254, p < 0.001), experience of EOL care provision (t = −5.466, p < 0.001), or experienced losing relatives (t = −2.200, p = 0.030) demonstrated significantly higher overall death literacy compared to those without such experiences. In terms of the DLI subscale performance, participants who had discussed EOL care with a physician scored significantly higher on practical knowledge (t = −4.791, p < 0.001), experiential knowledge (t = −2.719, p = 0.008), and factual knowledge (t = −4.180, p < 0.001). Participants with experience of EOL care provision scored significantly higher on all the subscales: practical knowledge (t = −4.198, p < 0.001), experiential knowledge (t = −3.256, p = 0.002), factual knowledge (t = −4.980, p < 0.001), and community knowledge (t = −3.522, p < 0.001). In addition, those who had experienced the loss of relatives showed significantly higher scores for experiential knowledge (t = −2.094, p = 0.039) and community knowledge (t = −2.419, p = 0.017; see Table 3).
The association of sample characteristics and death literacy.

SD: standard deviation; EOL: end-of-life.
There were no statistically significant correlations among age, KPS, and the total death literacy score or its four subscale scores.
Factors influencing death literacy
Stepwise regression analysis showed that experience of EOL care provision (p < 0.001), experience of EOL care discussion with a physician (p < 0.001), and sex (p = 0.001) were the three robust factors explaining 37.1% of the variance in the death literacy of patients with advanced NSCLC (F = 21.030, adjusted R2 = 0.371). Factors that were significantly associated with high level of death literacy were: participants’ experience of EOL care provision (β = 13.390, p < 0.001), experience of EOL care discussion with a physician (β = 10.901, p < 0.001), and being a woman (β = -8.671, p = 0.001; see Table 4).
Influencing factors related to death literacy from stepwise regression (N = 103).

β: standardized regression coefficients; CI: confidence interval; SE: standard error; EOL: end-of-life; VIF: Variance Inflation Factor.
Model 1: F = 29.881; p < 0.001; R = 0.478; R2 = 0.228; adjusted R2 = 0.221. Model 2: F = 23.478; p < 0.001; R = 0.565; R2 = 0.320; adjusted R2 = 0.306. Model 3: F = 21.030; p = 0.001; R = 0.624; R2 = 0.389; adjusted R2 = 0.371.
Discussion
Death literacy appears to be a reliable tool that individuals can use for their own benefit and strengthen their capacity for future caring. 9 Since patients with advanced NSCLC are likely to experience life-threatening emergency complications and severe cancer-related symptoms, early EOL discussions in this population are both critical and time sensitive. To the best of our knowledge, this is the first study to examine death literacy and its associated factors in patients’ individual characteristics with advanced NSCLC. The study achieved a high participation rate of over 90%. This may be attributed to the involvement of treating clinicians, who assisted in inviting eligible patients to participate in the data collection process. Participants had a mean age of 61.62 ± 10.86 years (range = 34–83 years), which was higher than that reported in a Turkish study of patients with chronic diseases (49.68 ± 15.15 years; range = 18–82 years). 26 This difference may be attributed to the disease characteristics of NSCLC, which typically occur between 65 and 84 years of age. 5 Participants demonstrated a moderate level of death literacy (mean score of 94.08 out of 145, tertiles: ⩽88, 89–103, >103), similar to a previous study conducted with patients with chronic diseases in Turkey. 26 The results of our study identified three influencing factors associated with higher levels of death literacy: experience of EOL care, experience of EOL care discussion with a physician, and being a woman.
In this study, an individual’s past experiences of EOL care emerged as the most influential factor associated with death literacy. These findings further confirm the experiential-based hypothesis proposed in previous research, highlighting that direct, personally lived experiences of EOL care situations are important events that shape an individual’s level of death literacy.26,27 Although past personal experiences cannot be changed or created, their role as emotional and cognitive triggers emphasizes the need for structured reflection opportunities, which enable more informed and value-aligned decisions, enhancing EOL care planning.
Previous research shows that planning one’s own EOL was positively related to death literacy. 29 Similar findings were also found in our study. Although only 29% of the participants in the present study had experience with EOL discussions with a physician, this proportion is lower than the approximately 40% reported in a previous study conducted in Canada. 7 This finding reflects the sociocultural context of Chinese culture, in which conversations about death are often avoided. Our results show that participants with EOL discussion experience demonstrated higher levels of death literacy than those without such experience, particularly in the subscales of practical, experiential, and factual knowledge. We believe that these individuals not only possess a greater understanding of the impact of disease trajectory on quality of life and the ability to discuss disease progression with a physician, but also have a better understanding of death-related systems, such as funeral and burial practices and relevant laws. More importantly, they appeared to be more capable of translating their insights into concrete actions in EOL planning.
Sex was identified as a key influencing factor in this study. Although NSCLC is more prevalent in men, 30 neither disease status nor survival time after cancer diagnosis appeared to improve death literacy. This finding aligns with the results of a previous study involving community-dwelling patients with chronic diseases in Turkey; there was no statistically significant difference in chronic disease duration and death literacy. 26 Additionally, women demonstrated higher levels of death literacy than men, particularly in the practical and experiential knowledge domains. These results differ from those of previous studies, which indicated that men scored higher on factual knowledge in those with chronic diseases. 26 In the Taiwanese cultural context, women are traditionally responsible for domestic affairs, whereas men handle public and social affairs. 31 In a patriarchal heritage society, the practice of mothering is deeply embedded within patriarchal structures. Care provision is often considered an assumed duty for women, closely associated with societal expectations that compel them to undertake caregiving roles within the family.32,33 As in previous research, through hands-on care, individuals not only improve their care skills but also gain valuable experience that ultimately leads to more informed and proactive participation in EOL care planning for themselves. 34 We believe that women take on more care responsibilities in the Taiwanese cultural context, which is one reason they may have a high level of death literacy.
However, in Asian societies, ‘death’ is often regarded as a misfortune, leading to avoidance of discussions on related topics. 35 Consequently, even individuals who have cared for dying persons may not have had opportunities to reflect on or integrate these experiences, limiting the meaning they derive and their understanding of death. Evidence suggests that death literacy should be cultivated across the general population and promoted through culturally sensitive approaches, such as compassionate community initiatives and death education programs. 36 Viewing palliative care as a public health strategy ensures that everyone in the community can access appropriate care whenever it is needed. 37 A 2025 systematic review further emphasized the importance of training programs that strengthen community engagement in caregiving and improve the quality of care for individuals with life-limiting conditions. Additionally, it highlighted the importance of considering caregivers’ and families’ needs in community education frameworks, given their vital role in sustaining palliative care and maintaining their own health and well-being following a patient’s death as part of broader public health strategies. These considerations should be integrated into both formal and informal education for healthcare professionals and the general public and volunteers, respectively. 38
In Taiwan, the Taipei City Government has integrated the Compassionate City Charter into municipal policies, implementing initiatives, such as Life Cafés, Life Education Course, across schools, businesses, and temples to promote death literacy and enhance understanding of what constitutes a good death.36,39 A previous study indicated that providing training for health professionals in implementing patient-centred communication strategies, along with organizing awareness programs in health institutions, helps increase death literacy among populations with chronic diseases. 26 Moreover, we believe that enhancing death literacy among both healthcare professionals and patients can foster open dialogue and facilitate value-based, concordant care, thereby improving the quality of care for patients with advanced cancer.
Accordingly, from a public health perspective, reducing the general public’s fear of discussing death may serve as an initial step in promoting death literacy by providing a convenient and accessible medium for social communication. 40 A 2021 narrative review emphasized the need to establish national education programs to improve public health and death literacy by integrating learning with opportunities for reflection on personal attitudes and actions, and by creating accessible spaces—such as Death Cafés, online educational initiatives, massive open online courses (MOOCs) on death and palliative care, and virtual hospice Interactive platforms—that encourage open discussion about death and dying.40,41 However, considering the local cultural context in which death remains a taboo topic in Taiwanese society—where event titles that explicitly include the word ‘death’ may deter participation and reduce individuals’ willingness to engage—we suggest renaming ‘Death Café’ to ‘Life Journey Tea House’. 42 This more appropriately reflects the cultural values and social norms that favour implicit approaches to discussing death.
Strengths and limitations
The present study had several strengths. First, this is the first study to focus on an advanced NSCLC population in terms of death literacy and to identify robust related factors. Second, considering that patients with advanced NSCLC belong to vulnerable groups and usually have poor physical status and a severe symptom burden, we not only engaged treating clinicians to verbally invite eligible patients to participate, thereby enhancing the participation rate, but also conducted one-to-one data collection to mitigate missing data. However, some limitations of this study must be considered when applying these findings. First, this was a single-centre survey, and differences in cancer types and characteristics may limit the generalizability of our findings. Second, the use of clinician-assisted invitations and self-reported measures may have introduced a social desirability bias. To mitigate such bias, the anonymity of the participants was ensured while completing the questionnaires. Finally, as this was a cross-sectional study design, the causality between variables or changes in death literacy over the course of the disease could not be explored. Future studies should adopt longitudinal designs to track the changes in death literacy in this population.
Conclusion
The findings of this study indicate that death literacy among patients with advanced NSCLC is slightly above moderate, and higher levels of death literacy are associated with the experience of EOL care, discussion of EOL care with a physician, and being a woman. These findings reinforce the concept that death literacy develops through personal encounters with EOL care and death-related experiences. In hospital-based anticancer treatment settings, the need to discuss the goals of care and EOL preferences becomes increasingly urgent as the disease progresses in patients with advanced cancer. Healthcare providers should recognize patients’ personal experiences as valuable opportunities to foster open dialogue regarding EOL care preferences. Implementing interventions such as Life Journey Tea House, online educational initiatives, and MOOCs is recommended to foster reflexivity and meaning-making, and to promote open dialogue and knowledge exchange about EOL care preferences.
By clarifying these key influencing factors, this study contributes significantly to the existing body of knowledge on death literacy in patients with advanced cancer. It lays the foundation for further research to specifically explore how death literacy affects the expression and practical application of EOL care decisions, such as preference for life-sustaining treatments, potentially improving patient-centred care and decision quality. In summary, fostering death literacy through personal experience and facilitating dialogue in clinical settings are keys to advancing meaningful EOL care planning for patients with advanced cancer.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524251408892 – Supplemental material for Patient characteristics associated with death literacy in advanced non-small-cell lung cancer: A preliminary single-centre cross-sectional study
Supplemental material, sj-pdf-1-pcr-10.1177_26323524251408892 for Patient characteristics associated with death literacy in advanced non-small-cell lung cancer: A preliminary single-centre cross-sectional study by Gong-Fu Lin, Yi-Ling Yeh, Shiow-Ching Shun, Ching-Yao Yang and Cheng-Pei Lin in Palliative Care and Social Practice
Footnotes
Acknowledgements
We thank all the patients with advanced NSCLC who participated in this study. The authors also gratefully acknowledge the support and involvement of many individuals without whom this study could not have been completed, including administrative and clinical staff, physicians, and head nurses.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the Institutional Review Board of the National Taiwan University Hospital in Taipei City, Taiwan (approval number: 202307012RINC).
Consent to participate
Participants provided written informed consent prior to completing the questionnaire.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a grant from the National Taiwan University Hospital (Reference number: 113-N0004).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The raw data are not publicly available due to the conditions of institutional ethics approval.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.