
Abstract
Migrant care-workers (MCWs) are often the main caregivers for frail older persons. We examined the complex relationship between MCWs and primary family caregivers (PFCs) in Israel to better understand how MCWs and PFCs perceive the formal and informal nature of their relationship. Given the high prevalence of two-income families who are unavailable for caregiving, the relationships among MCWs, PFCs, and care-recipients warrants examination, particularly when PFCs serve as managers of care and the care-recipient has dementia. The sample of 116 MCWs and 117 PFCs included 92 MCW–PFC pairs who were part of a larger study on home care for frail older persons. A mixed-methods approach was used involving quantitative (correlations/paired t-tests) and qualitative (grounded theory framework) analyses conducted on data obtained from structured interviews. A significant correlation was found between ratings of the quality of the relationship by MCWs and PFCs, although PFCs rated it significantly more positively than MCWs. MCWs’ ratings of their relationship with the PFCs were significantly correlated with their ratings of the quality of their relationship with the care-recipient. Four main thematic categories emerged from the qualitative analysis: (1) communication, (2) dependence, (3) relationship quality, and (4) triad: MCW–PFC–care-recipient. For each theme, we present perspectives of MCWs and PFCs, reflecting either “closeness” or “distance” in their relationship. The findings highlight the complexity of such relationships, with the potential for a meaningful positive bond or mistrust or abuse. The study provides a basis for testing methods for ameliorating the negative experiences described by some participants.
Keywords
Background
Caregiving for older adults is one of the main occupations in which migrant workers are employed in Israel, where most older adults choose to remain at home as they become dependent (Asiskovitch, 2015). Around a quarter of dependent adults in Israel are cared for by live-in migrants (Asiskovitch, 2015; Brodsky et al., 2016). While, in the past, older adults in Israel were mostly taken care of by a primary family caregiver (PFC), today this responsibility is increasingly shared by migrant care-workers (MCWs) and PFCs. The growing demand for MCWs is due to structural societal changes, such as population aging, women’s unavailability for informal caregiving due to increased participation in paid employment, and inadequacies in formal care services (Cangiano & Shutes, 2010; Cohen-Mansfield et al., 2013). The demand for MCWs is also based on most older persons’ desire to “age in place,” that is, to stay in their own home rather than to move to a congregate living arrangement, which requires a transition and decreases autonomy. Thus, MCWs are increasingly hired in Israel and elsewhere (Cohen-Mansfield et al., 2013). While prior studies have tended to focus on the relationship between the older person and the MCW, for example, Porat and Iecovich (2010), Teshuva et al. (2019), and Walsh and Shutes (2013), this article complements them by focusing on the relationship between the PFC and MCW.
In Israel, MCWs provide home care, which is partly supported by the government based on eligibility criteria (Ayalon et al., 2014; Cohen-Mansfield et al., 2013; Lavee & Katz, 2003). Israel’s National Insurance Institute’s benefit to finance migrant-based care is available mainly to those who have reached retirement age and have significant functional and/or cognitive impairment, generally involving frail older adults (Israel National Insurance Institute, 2023). Home-based personal care-workers represent almost 90% of the long-term care workforce, and 71% of long-term care workers are foreign born (OECD, 2020). At the end of 2021, there were 71,548 authorized and illegal foreign care-workers in Israel (Israel Population and Immigration Authority, 2022). The rates of usage and regulations concerning MCWs vary greatly across countries (Cohen-Mansfield et al., 2013). For frail older persons in Israel who need continuous care, the use of MCWs is often the only viable option, especially since the government partially subsidizes this type of care. The MCW most often lives with and takes care of the frail older person around the clock. Legal regulations govern the free time and living conditions to which MCWs are entitled (Cohen-Mansfield et al., 2016).
Although most employers understand and follow government regulations regarding the employment and living conditions of MCWs (Cohen-Mansfield et al., 2016), others expect MCWs to provide constant care (Cohen-Mansfield et al., 2016). Some MCWs have reported being exposed to different types of exploitation, including economic, workload, mental, physical, sexual, and nutritional (Ayalon, 2009a). According to Israel’s Foreign Workers Law, most foreign workers must renew their work permits annually, for up to 5 years, but MCWs are permitted to remain in Israel as long as their current employer needs them (Amit, 2014). This law creates a dependency of MCWs on their employers.
Employing an MCW has been found to be associated with a reduction in PFC burden (Chiatti et al., 2013). Many PFCs describe their role in this new triad as “care manager” (Ayalon, 2009b), a role with responsibilities like improving the communication between the MCW and the older person, particularly if there is a language or cognitive barrier.
Four types of employer–manager relationships between Taiwanese employers and live-in Filipino migrant workers who performed childcare and/or eldercare functions were described by Lan (2003): (1) maternalistic managers, who are generous and benevolent, but regard themselves as morally superior and define migrant workers as needy and immature; (2) managers who take a personal approach, building a relationship with the caregiver without imposing a strict hierarchy; (3) hierarchal managers, who maintain distance and define the migrant worker’s role as inferior; and (4) business managers, who closely regulate the caregiver and create a clear separation between work and private space. These approaches are aligned with two types of social boundaries: socio-categorical boundaries that relate to class and ethnicity/nationality, and socio-spatial boundaries that relate to separate public and private spaces (Lan, 2003). Occasionally, a relationship develops in which the MCW is “adopted” as a family member, receives affection, and carries out family-role obligations (Baldassar et al., 2017). This form of relationship was described by Karner (1998) as “fictive kin,” a conceptualization that enables the family to continue to maintain a cultural ideal of “family-caring,” preserving a familial atmosphere despite familial unavailability for day-to-day caregiving. Ayalon (2009b) suggested that PFCs often expect MCWs to provide emotional care for older persons, although this is not part of the MCW’s job description. Rather than paying them more for this additional responsibility, some PFCs consider MCWs as “part of the family,” inviting them to family events, and giving them gifts.
The role of MCWs inside the home is influenced by cultural differences and language barriers (Bourgeault et al., 2010). Relationships between MCWs and care-recipients in home and long-term care settings have been described as diverse from the perspectives of both. Such relationships can be mainly professional without emotional attachment, or friendly or family-like (Teshuva et al., 2019), or discriminatory, as exemplified by racist verbal abuse (Bourgeault et al., 2010; Walsh & Shutes, 2013). Iecovich (2014) found that less ambivalence in these relationships predicted less loneliness among care-recipients. The notion of “being part of the family” can imply that the MCW must accept a 24-hour work-day, perform “free favors,” and carry out emotional as well as physical labor (Hondagneu-Sotelo, 2001; Puppa, 2012). However, some research has shown that kin-like relationships between MCWs and care-recipients are an important aspect of quality care (Baldassar et al., 2017). Since systems of formal and informal care are connected, boundaries of assistance between MCWs, older adults, and PFCs are often unclear (Baldassar et al., 2017).
Given the limited empirical research concerning the relationship between MCWs and PFCs, especially from the perspective of PFCs (Salami et al., 2017), we examined this relationship using both quantitative and qualitative methodologies to gain a better understanding of how MCWs and PFCs perceive the formal and informal aspects of their relationship, with the goal of offering insights into how to strengthen those relationships and ultimately improve quality of care for care-recipients.
Methods
This inquiry into the relationship between MCWs and PFCs is part of a larger survey study on home care for frail older persons (Cohen-Mansfield et al., 2016; Cohen-Mansfield & Golander, 2022; Teshuva et al., 2019).
Participants
We identified 215 households in which MCWs provided care for older persons in Jerusalem and the greater Tel Aviv area in Israel. Seventy-three percent (156/215) of recruited households were contacted through cooperation with the National Insurance Institute of Israel, which regulates and partially funds the hiring of MCWs. At our request, the institute sent letters to eligible households informing them of this study opportunity. For those who informed the institute that they were willing to participate, the institute transmitted contact information to the research team. Other individuals were recruited by such means as posting advertisements at adult day centers and snowballing from recruitment efforts for other studies. The recruitment process is illustrated in Figure 1. Inclusion criteria required MCWs to work full-time as a live-in caregiver at an older person’s home and to speak sufficient English or Hebrew to participate in an interview. We recruited 116 MCWs and 117 PFCs, including 92 pairs of MCWs and PFCs. Recruitment of participants.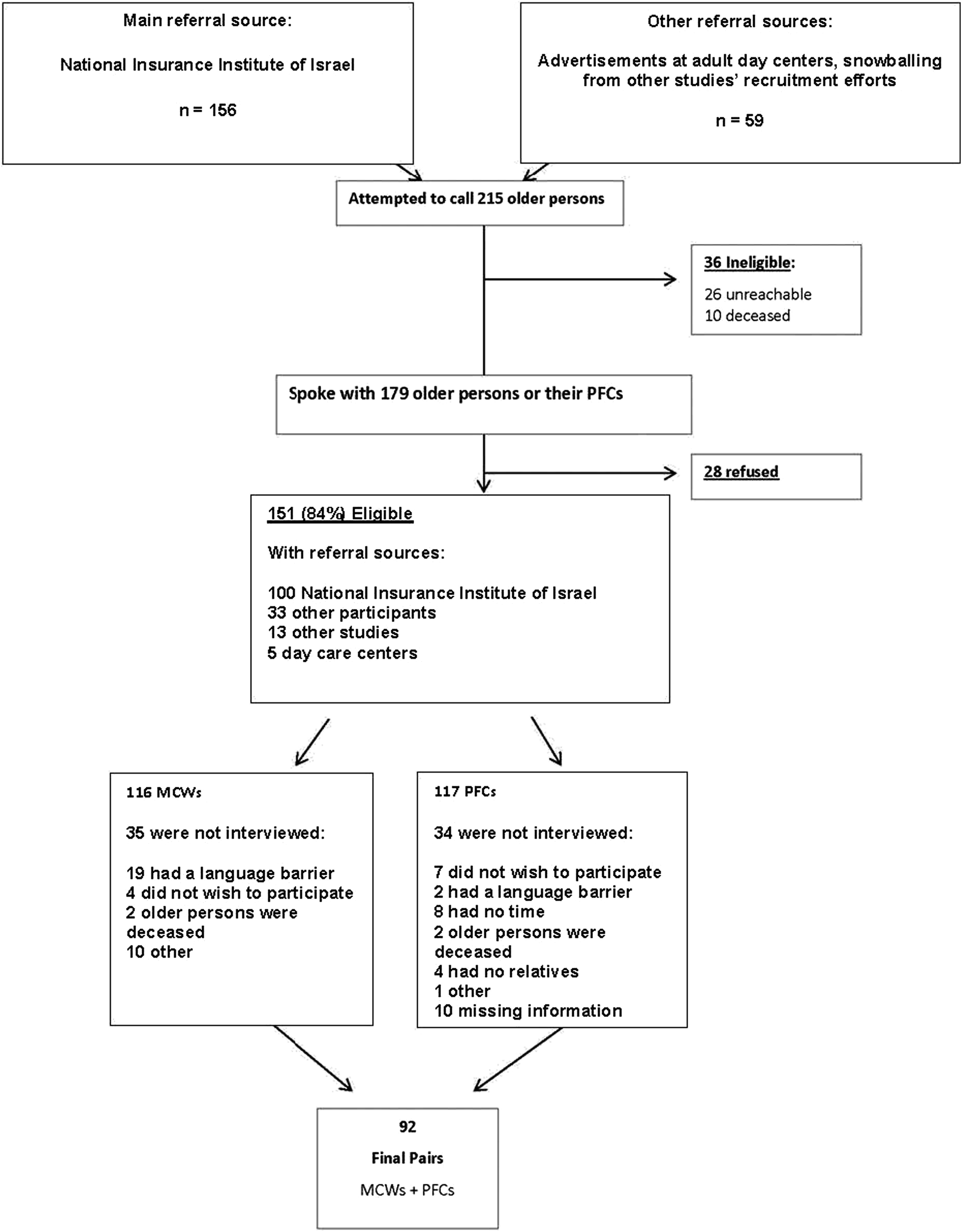
Process
After receiving contact information via one of the study’s recruitment methods, we telephoned potential participants, described the study, and verified that they were either a PFC or an MCW and that they cared for an older person for whom daily care was provided by a live-in MCW. We then asked those we reached if they wished to participate, and 84% (151/179) agreed. The one-on-one interview meeting began with provision of further information about the study, the signing of an informed consent form, and then the administration of the structured interview at a location of the participant’s choice.
Interviews
The interview questions reported in this paper were developed by the research team in line with this study’s aims. The larger study, of which this is a portion, included both previously validated assessments and assessments developed specifically for this study (Cohen-Mansfield et al., 2016; Cohen-Mansfield & Golander, 2022; Teshuva et al., 2019). Background information, including age, gender, country of birth, and education level, was collected during structured interviews conducted separately with MCWs and PFCs. For the quantitative analysis, both PFCs and MCWs were asked to rate the quality of their relationships (PFC–MCW and PFC/MCW–older person) on a 6-point scale ranging from 1 = “terrible” to 6 = “excellent.” In order to further illuminate the relationship between MCWs and PFCs, we examined qualitative data from open-ended interview questions. The three main questions were as follows: (1) What are the reasons for your quality-of-relationship ratings? (2) What are the good things in the relationship? (3) What can be improved in the relationship? We also reviewed comments to other questions, such as those relating to aspects of the MCWs’ working conditions and the care they provided.
Procedure
The study was approved by the Tel Aviv University Institutional Review Board, and written informed consent was obtained from all participants. Most of the interviews were conducted in participating older persons’ homes, as MCWs could not leave care-recipients alone. According to interviewers’ ratings, most interviews were conducted in complete privacy. However, about 10% were not conducted in complete privacy, and more than a quarter were conducted in partial privacy. Structured interviews were carried out in either Hebrew or English and lasted about 90 minutes. This time frame included collection of other data as part of the larger study.
Although this paper deals with PFC–MCW dyadic relationship, the approach taken was that of separate interviews (Eisikovits & Koren, 2010), which was more appropriate than joint interviews given the sensitive topics raised, such as challenging behaviors and problematic practices. Correspondingly, participant interview answers were not shared with the other member of the dyad.
Analytic Methods
For the quantitative analyses, we used correlations and paired t-tests to examine (1) the relationship between the rated quality of relationship as reported by PFCs and MCWs and (2) the relationship between the reported ratings of quality of relationship between PFCs and MCWs, and that of their ratings of their relationship with the care-recipient. For the qualitative analysis, we first used thematic analysis (Braun & Clarke, 2006), involving reading and re-reading the data in search of meanings and patterns, and creating a list of codes, with codes clustered into main groups based on similarity and overlap. The initial groupings were further refined, resulting in the identification of main themes and sub-themes. Several staff members reviewed and discussed the findings until they reached consensus. The next step in the analysis sought to deepen our understanding of the findings using a grounded theory framework (Strauss & Corbin, 1998): (1) collection and analysis of data administered without a preconceived framework in mind, based on the thematic analysis; (2) development of theories and ideas based on the data grounded in participants’ experiences, with the goal of reaching flexible conclusions in order to accommodate any future contradictory data; (3) development of conclusions through broad concepts and then more specific themes; and (4) emphasis on keeping the data analysis process as open and transparent as possible. We analyzed each theme from the points of view of the PFCs and MCWs, and present representative quotations below, identifying each by participant number, PFC gender, and MCW gender.
The analytical approach concerning the dyadic relationship sought to clarify the point of view of each member of the dyad, but the analysis was not dyadic, in that the data were not initially organized as the text of narratives provided by the 92 dyads and read as dyads. Rather, the texts were read as those provided by PFCs and those by MCWs, and themes that were representative of their statements were searched for and considered. The analysis focused on clarifying the respective points of view of each dyad member. Clarifying both points of view and understanding their diversity and similarity were the central goals of the study. The analysis yielded corresponding themes among PFCs and MCWs. Those themes were then compared and contrasted—between the two groups and within the positive and negative manifestations of the themes. The quantitative analysis was more directly dyadic in that it used paired t-tests to compare the rating attributed to the relationships between the respective members of the dyads.
Quantitative Results
Participants’ Characteristics
Most MCWs were female (91.4%) with an average age of 38.9 (SD = 7.2) years. Almost two-thirds of MCWs were born in the Philippines (63.5%), followed by Nepal (14.8%), India (11.3%), Sri Lanka (8.7%), and Moldova (1.7%). Over half of MCWs indicated being married (60.3%) with an average number of 2.3 (SD = 1.3) children. MCWs had an average of 13.0 (SD = 2.1) years of education, and the vast majority of them indicated having had some caregiving training (82.5%). Close to a third of MCWs indicated working for an older person who had dementia (29.3%). Corresponding older care-recipients (n = 54) had an average age of 85.9 (SD = 6.2) years. When age information was available from older care-recipients’ PFCs, average age of older care-recipients was reported to be 87.9 (SD = 6.8) years. None of these demographic characteristics were significantly associated with our outcome measures and have been excluded from further analyses.
The average age of PFCs was 63.98 (SD = 10.3) years. Most PFCs were female (70.1%) and born in Israel (65.5%). Almost three-quarters of PFCs were the care-recipient’s son/daughter (73.5%), followed by spouse (19.7%), son/daughter-in-law (3.4%), grandchild (1.7%), sibling (.9%), and others (.9%).
Analysis of Ratings Concerning the Quality of Relationship
The Relationship Between PFC and MCW According to Both Sources.
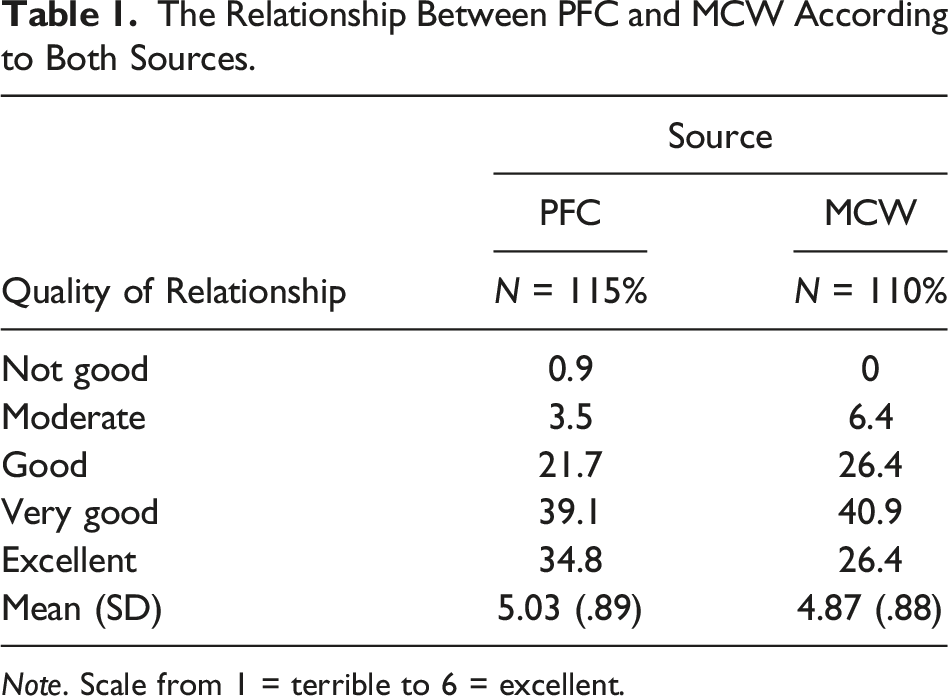
Note. Scale from 1 = terrible to 6 = excellent.
A significant correlation was found between ratings of quality of relationship by MCWs and PFCs (r = .347, two-tailed p = .001, n = 88), although PFCs rated it significantly more positively than MCWs (t87 = 2.06, two-tailed p < .05). MCWs’ ratings of their relationship with the PFC were significantly correlated with their ratings of the quality of their relationship with the care-recipient (r = .351, two-tailed p < .001, n = 109). PFCs’ ratings of the quality of their relationship with the care-recipient were not significantly correlated with their ratings of the relationship with the MCW.
Qualitative Findings
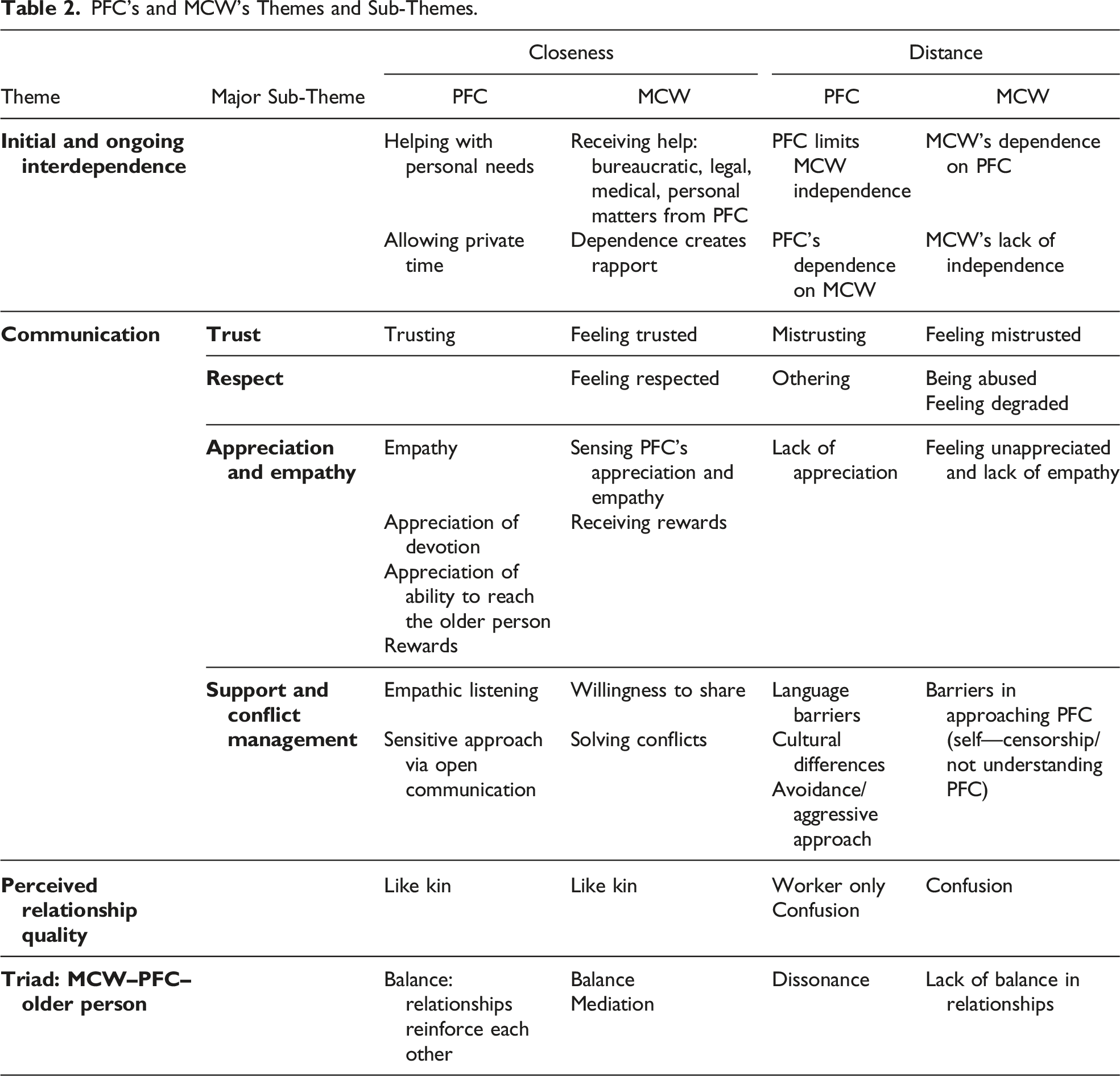
PFC’s and MCW’s Themes and Sub-Themes.
Theme 1: Initial and Ongoing Interdependence
MCWs were usually dependent on their employers for help in dealing with bureaucratic, medical, legal, and personal matters because they were new to the country and needed to maintain their visa/work-permit status. PFCs tended to be dependent on MCWs because they were usually unable to take care of the care-recipient by themselves in case the MCW quit or was dismissed, in which case finding an acceptable replacement could be complicated and time-consuming.
Closeness: PFC
Helping With Personal Needs
MCWs often needed help accessing health and other services, such as arranging an internet connection, finding grocery stores which sold food to which they were accustomed, and the like. Some PFCs helped MCWs with these matters: “I take care of all kinds of problems. She has some health problems. She got married and has had problems getting pregnant. I take her to the doctors, everything she says. I spoil her a little, everything she asks, even when her head aches” (#113 PFC-F; MCW-F).
Allowing Private Time/Some Independence
Some PFCs validated the importance of rest and ventilation for MCWs: “[She’s got] two hours a day to go wherever she wants. Sometimes she has errands, sometimes she meets a friend” (#73 PFC-F; MCW-F).
Closeness: MCW
Receiving Help
MCWs often described receiving help from PFCs with bureaucratic issues, such as visa status, doctor appointments, and health insurance. When asked to list reasons why she considered the relationship quality high, one MCW said, “She’s helpful, the daughter. If I need a doctor, she calls to make me an appointment. If I need something, she looks on the internet and tells me” (#136 MCW-F; PFC-F).
PFCs’ Dependence Creates Rapport
Some MCWs perceived the PFC’s dependence on them as promoting closeness: “We are like a family, one family. No one can stay with her [care-recipient] for long. I can” (#76 MCW-M; PFC-F).
Distance: PFC
PFC Limits Independence
Most of the time, MCWs could not leave the care-recipient alone. For example, “Father can’t stay alone at all, so he [the MCW] can’t leave. If there is something unusual, he asks me in advance and I come there, but it is rare” (#18 PFC-F; MCW-M).
PFCs’ Dependence on MCW
In some cases, the relationship was governed by the PFC’s dependence on the MCW’s services. For example, when one PFC was asked why she did not replace an MCW with whom she was dissatisfied, she answered, “Because there are no other employees. And mother is afraid someone else will come and run away. It is the lesser evil” (#55 PFC-F; MCW-M).
Distance: MCW
MCWs’ Dependence on PFC
MCWs felt constrained from making requests due to dependence on the PFC to maintain legal status: “If I ask her [the employer] for too much [time to go out] she will kick me [out] and then I will have to go back to the Philippines, and I want to stay more and make more money” (#59 MCW-F; PFC-F).
MCWs’ Lack of Independence
MCWs usually worked 24 hours a day, 7 days a week. As described by one MCW, “when you work 24 hours with no time off, and the family is not supportive, it is very difficult” (#106 MCW-M; PFC-F).
Theme 2: Communication
Trust
Both MCWs and PFCs spoke about the importance of mutual trust as a determinant of the quality of their relationship.
Closeness: PFC
PFCs often expressed trust in MCWs, usually basing it on the way MCWs treated the older care-recipient, as in, “You can trust her. [She is] creative, has solutions and ideas, [is] very dedicated, caring” (#16 PFC-M; MCW-F).
Closeness: MCW
For MCWs, trust was connected to the help they received from the PFC. For example, “Let’s say I have a problem, they [the family] support me. They understand me, even if I have a problem with their mother, they believe me … they trust me” (#71 MCW-F; PFC-M).
Distance: PFC
Mistrust
Some PFCs expressed doubts about MCW trustworthiness: I wanted to install cameras because you can never know, even though I see a decent person … but he’s not family. I don’t know if you can really know, that’s the worst part … it’s not like this is only me; it’s the same for everyone. (#118 PFC-F; MCW-M)
Distance: MCW
Feeling Mistrusted
MCWs often described feeling mistrusted as a reason for rating the relationship quality as low. For example: They put the camera in the house when I was in my country, but I don’t care. Always, I’m feeling it is not nice because they are watching in the camera, there is tension about that. If I ask them to take it away, they will ask why. They are watching everything, at the beginning, my friends stopped coming because of the camera, but I told them, “No, we are not doing anything wrong.” I sleep in the living room where the cameras are, but I can’t undress [there] because they are always watching. (#86 MCW-F; PFC-F)
Respect
This sub-theme concerns recognition of human needs and equality.
Closeness: MCW
Feeling Respected by PFCs
Some MCWs offered comments like, “They respect me, and I respect them” (#98 MCW-F; PFC-M).
Distance: PFC
Othering of MCWs
“Othering” occurs when an individual or a group is classified as being “not one of us,” with different, less human qualities (Jensen, 2011). For example, when asked to what extent he considered the MCW’s work mentally difficult, one PFC said: Look, if he was an Israeli, I could give a score [of difficulty] but since he is not ... their attitude toward working with older persons is different …. If I had to work with an older man, and wipe his ass, and when he vomits, [and] to clean his saliva—mentally, it would exhaust me, but the Nepalese mentality … they have no impediment to doing all these things. To feed the older person with a spoon, it doesn’t bother them; they see it as a mission. (#137 PFC-M; MCW-M)
Some PFCs tried to present themselves as enlightened and caring and may have been oblivious to the othering outlook revealed by their words: “I try to treat her like a human being, and not as a black worker; I am not degrading” (#84 PFC-F; MCW-F).
Distance: MCW
Being Abused
Although interviews were not always private, nevertheless, some MCWs mentioned being abused or humiliated by PFCs. Some MCWs described being asked to do tasks which were not part of their job description (e.g., washing the car, cleaning others’ houses, and providing care for additional people). One MCW who described exploitation specifically referred to her dependence due to her migrant status: The husband said I also had to take care of their four children. The house was messy. [There were] many lies. The husband said [my] papers were in the embassy and said that I had to take care of their four children, but he would never show me the papers … The husband [would] hold me like he wants to be with me, and for months I don’t speak to him about it. When I told him I want to go, he asked me why, and I told him, “you are always touching me,” and I told him, “I have a husband and I don’t want him.” When the agency asked why I wanted to leave, I didn’t tell them because, [do] you think they [would] believe me? (#124 MCW-F; PFC-M)
Feeling Degraded
Some MCWs indicated that their living conditions were not satisfactory or private, for example, “… some of [their] friends sleep in the living room [where I sleep], and how can one work if one doesn’t sleep comfortably?” (#29 MCW-F; PFC-F).
Appreciation and Empathy
Many PFCs described appreciation for MCWs’ dedication and commitment.
Closeness: PFC
Empathy
Many PFCs understood MCW’s stressful life circumstances and personal needs: “[It is] mentally difficult because she is away from her family. She has three small children abroad. She doesn’t take a day off—she needs the money, she’s got very serious financial pressure” (#5 PFC-F; MCW-F).
Appreciation of MCWs’ Devotion
PFCs often emphasized that MCWs were devoted to the care-recipient and that the care was sincere and beyond the job’s requirements: “My mother matters to her. She [the MCW] treats her like a person, not necessarily as someone for whom she works. [It is] more than that” (#11 PFC-M; MCW-F).
Appreciation of MCWs’ Ability to Reach the Care-Recipient
Some PFCs acknowledged that the care-recipient was difficult and appreciated MCWs’ skill at managing challenging behaviors with dedication: She [the caregiver] can tolerate her [the care-recipient] being a nagger. The fact that she’s sick all the time, it can freak you out, and I say that from experience. Right now, she [the MCW] understands that she can’t get out of the house too much. When Grandma is in the hospital, I see how she [the care-recipient] behaves, [yet] she [the MCW] does not move from her. She is very dedicated, and there is also sensitivity to this. (#151 PFC-F; MCW-F)
Rewards
When close relationships developed between MCWs and PFCs, some PFCs rewarded MCWs with presents like a computer or communication device to maintain contact with their families abroad, loans, presents for holidays, and the like. For example, “When she [the MCW] has a birthday, she receives a gift. On her holidays, she receives gifts. When I’m on vacation, I buy her a present” (#98 PFC-F; MCW-F).
Closeness: MCW
Sensing PFCs’ Appreciation and Empathy
MCWs appreciated when communication by PFCs included gratitude: “They tell me they appreciate my work and love me and understand I have my life. They say, ‘I know that you love my mother so much and we love you too’” (#62 MCW-F; PFC-M).
Rewards
MCWs usually understood gifts given by PFCs as acts of gratefulness: “They are generous, they give me some stuff. On holidays, they give me a gift” (#32 MCW-F; PFC-M).
Distance: PFC
Lack of Appreciation
Several PFCs expressed misgivings when MCWs failed to demonstrate initiative. For example, “She [the caregiver] is not so good. You need to tell her [what to do]. If you don’t tell her, she doesn’t do it. Her life is [spent] talking on the phone” (#2 PFC-M; MCW-F). Some PFCs thought that MCWs worked mainly to extend their stay in Israel: “She came here for the money … She is trying very hard to keep my mother in good shape because she wants to stay here [in Israel]” (#9 PFC-F; MCW-F); “If she [the MCW] had to return there now, it would be a downward move for her in every way” (#16 PFC-M; MCW-F).
Distance: MCW
Feeling Lack of Empathy and Appreciation from PFCs
Lack of recognition added to the emotional burden of caregiving: “Being a caregiver is very mentally exhausting. Twenty-four hours to be with the older person is difficult and to be paid minimum wage is not enough. … If … Israelis worked 24-hours they [would] explode” (#106 MCW-M; MCW-F).
Support and Conflict Management
Closeness: PFC
Empathic Listening
Some PFCs offered emotional support to MCWs: I listen to her. It’s not easy for her. She needs a listening ear. [Perhaps] it’s enough to have someone to talk to from our family … and we try to help her, even if it’s very little help, we care. I feel like there’s much more to her than what we can see. … I’m sure she cries. She has a 3-year-old son in Moldova. The fact that I listen to her and that she knows she can talk to me helps the relationship. (#73 PFC-F; MCW-F)
Sensitive Approach
Some PFCs expressed sensitivity to MCWs’ needs: “Sometimes I have complaints concerning my mother, not about her. When mom nags her while she’s on the phone, I tell her [my mother], she has no family here, she’s alone, we should help her” (#135 PFC-M; MCW-F). Some PFCs found gentle ways to address shortcomings they noticed in MCWs’ work: “… If something doesn’t seem right to me, I tell her courteously, sometimes with a sense of humor. My mother is satisfied and the caregiver is satisfied as well” (#22 PFC-F; MCW-F).
Closeness: MCW
Willingness to Share
In some cases, MCWs described open lines of communication: “We speak together about Ruth’s condition and we share with one another about our families … we are open” (#98 MCW-F; PFC-M).
Solving Conflicts via Open Communication
Some MCWs felt that their ability to function effectively was aided by the PFC: I talk to her [the PFC] openly. I will tell her what I want, what the problem is. It is good that if we have a problem between the two of us [MCW and care-recipient] … then the daughter [PFC] doesn’t talk to me on the phone; she comes here and talks to me in person and it is better. It is easier to understand her [in person] than over the phone. (#107 MCW-F; PFC-F)
Open communication was also thought to head off conflict: “… we don’t fight. We always share ideas. He [the PFC] is like a brother and a friend. You can say what you want ….” (#62 MCW-F; PFC-M).
Distance: PFC
Language Barriers
PFCs sometimes blamed MCWs for communication difficulties: “[She should] learn the language better. She has been here for more than five years … She knows a lot of words in Hebrew and knows a little reading, but to construct a proper sentence—no!” (#66 PFC-F; MCW-F).
Cultural Differences
PFCs sometimes wanted MCWs to be more open with them and perceived the MCW’s behavior as reflecting a diverse outlook: “I contact her about everything I need, I feel free to tell her everything I need. She doesn’t disclose everything, but it’s because of her culture. They are very closed people” (#100 PFC-M; MCW-F).
Dealing With Conflicts: Avoidance and Aggression
One way of dealing with conflicts was avoidance, which, nevertheless, caused stress, as one PFC suggested: “I don’t tell her everything I think because I decided that my mother is running her and giving her remarks [direction], although it’s hard for me not to say what I think, and it creates some tension” (#91 PFC-F; MCW-F). Some PFCs interacted with MCWs in a verbally abusive manner: “She comes on a Saturday night [from a day off]. She doesn’t say hello, doesn’t ask how she [the care-recipient] is … I told her, if you do not treat her well, I’ll throw you out!” (#135 PFC-M; MCW-F).
Distance: MCW
Barriers to Communication
Only a few MCWs indicated communication barriers, such as self-censorship due to fear of employment and/or visa/work-permit status forfeiture: “I keep quiet because I must finish [my work]. I don’t like switching jobs all the time. How much I suffer, I suffer” (#135 MCW-F; PFC-M). Some MCWs thought PFCs were not open with them: “I don’t know how they feel … I sometimes ask if they like me and if I have hurt their feelings. It’s better to know if you did something wrong, better to be open than to hide something” (#98 MCW-F; PFC-F).
Theme 3: Perceived Relationship Quality Between MCWs and PFCs
While some described “feeling like a family,” as mentioned by Ayalon (2009b), some felt distant or confused concerning the MCW–PFC relationship.
Closeness: PFC
Like a Family Member
Many PFCs considered MCWs as more than workers: “The relationship that has developed over the years is that we see her as a family member. She is more than a caregiver. She understands household and family matters” (#127 PFC-M; MCW-F).
Closeness: MCW
Like a Family Member
Similarly, many MCWs felt accepted as part of the care-recipient’s family: “He [the PFC] is like a father, he is asking me if I want to eat, if I want to go somewhere. He worries about me, sometimes when I go out, he calls to see I’m okay” (#40 MCW-F; PFC-M). Other MCWs considered their situation a temporary replacement for their own family: “She’s [the care-recipient] like my mother and grandmother because I’m far from my family, and the love I need to show them I give to her. … Also, her family treats me like family” (#98 MCW-F; PFC-F).
Distance: PFC
Worker Only
Other PFCs saw the relationship as strictly professional: “It’s the same way as when I go to work, this is her job. She isn’t my friend and she isn’t my family” (#133 PFC-M; MCW-F).
Context-Dependent Relationships
Some PFCs described changeability or ambiguity in their relationship with MCWs: “It’s a problem. Sometimes a family member and sometimes a worker, it varies” (#21 PFC-F; MCW-F).
Distance: MCW
Confusion
Some MCWs described a conflicted status: “I feel that I am a part of the family, but still, I am only the caregiver. There is a limit” (#16 MCW-F; PFC-M).
Theme 4: Triadic Relationships—MCW–PFC–Care-Recipient
Both PFCs and MCWs felt that the relationship between the MCW and older person affected the relationship between the MCW and PFC. Likewise, the relationship between the PFC and older person sometimes affected the relationship between the MCW and PFC.
Closeness: PFC
Triadic Relationships Reinforced Each Other
Usually, if care-recipients maintained good relationships with MCWs, this positively impacted the relationship between the PFC and MCW, as described by one PFC: “Anyone who loves my father like this and takes care of him also wins my love” (#18 PFC-F; MCW-M). Some PFCs thought their relationship with the MCW would affect how the MCW treated the older person, as in, “If I don’t have a great relationship with her [the MCW], then what have we done? I’ve got to have a great relationship with her so she can take care of her [my mother] like her mother” (#93 PFC-F; MCW-F).
Closeness: MCW
Different Types of Support Facilitated Triadic Functioning
MCWs emphasized the nexus between their relationship with the PFC and the MCW’s ability to function effectively. For example, “I get a lot of support from Danny [the care-recipient’s son], and it helps me do my job well” (#50 MCW-M; PFC-M). Similarly, mediation by a PFC can support the MCW’s ability to function: “The daughter is very understanding; if there is trouble with her mom, she can explain [the situation] to her mom ….” (#84 MCW-F; PFC-F).
Distance: PFC
Dissonance
In a few cases, there was dissonance within the triadic relationship, as when the PFC was not satisfied with the MCW, while the care-recipient refused to dismiss the MCW: “I feel anger towards him [the MCW] …. I don’t say anything to him because she [the care-recipient] doesn’t let me tell him. I’d have kicked him out long ago” (#55 PFC-F; MCW-M).
Distance: MCW
Lack of Balance
In some cases, MCWs had good relationships with older care-recipients, but less so with PFCs: “I need a lot of patience … I can’t say [to the PFC], ‘don’t come’. I’m not here for a lifetime. I wish the son would be here less, but it is really good for [his] mother that he is here. She can’t start eating without him” (#16 MCW-F; PFC-M).
Discussion
The quantitative results revealed that the relationship quality between PFCs and MCWs was rated positively by a majority, with PFCs rating it significantly higher than MCWs, and with the correlations between the ratings being positive and statistically significant, albeit not high. Relationship quality between PFCs and MCWs was significantly correlated with MCWs’ relationships with care-recipients, but was not significantly correlated with PFCs’ relationships with care-recipients.
The qualitative findings revealed two process themes: interdependence and communication, and two structural themes: (1) a perceived model of quality of relationship between MCWs and PFCs and (2) relationship as a link within triadic relationships: MCW–PFC–care-recipient. All themes were articulated by PFCs and MCWs, and each theme was experienced as more positive (fostering closeness) by some and as more negative (furthering distance) by others. Taken together, the themes reveal a process schematically summarized in Figure 2. A schematic theoretical framework for the factors affecting the perceived quality of relationship between PFCs and MCWs.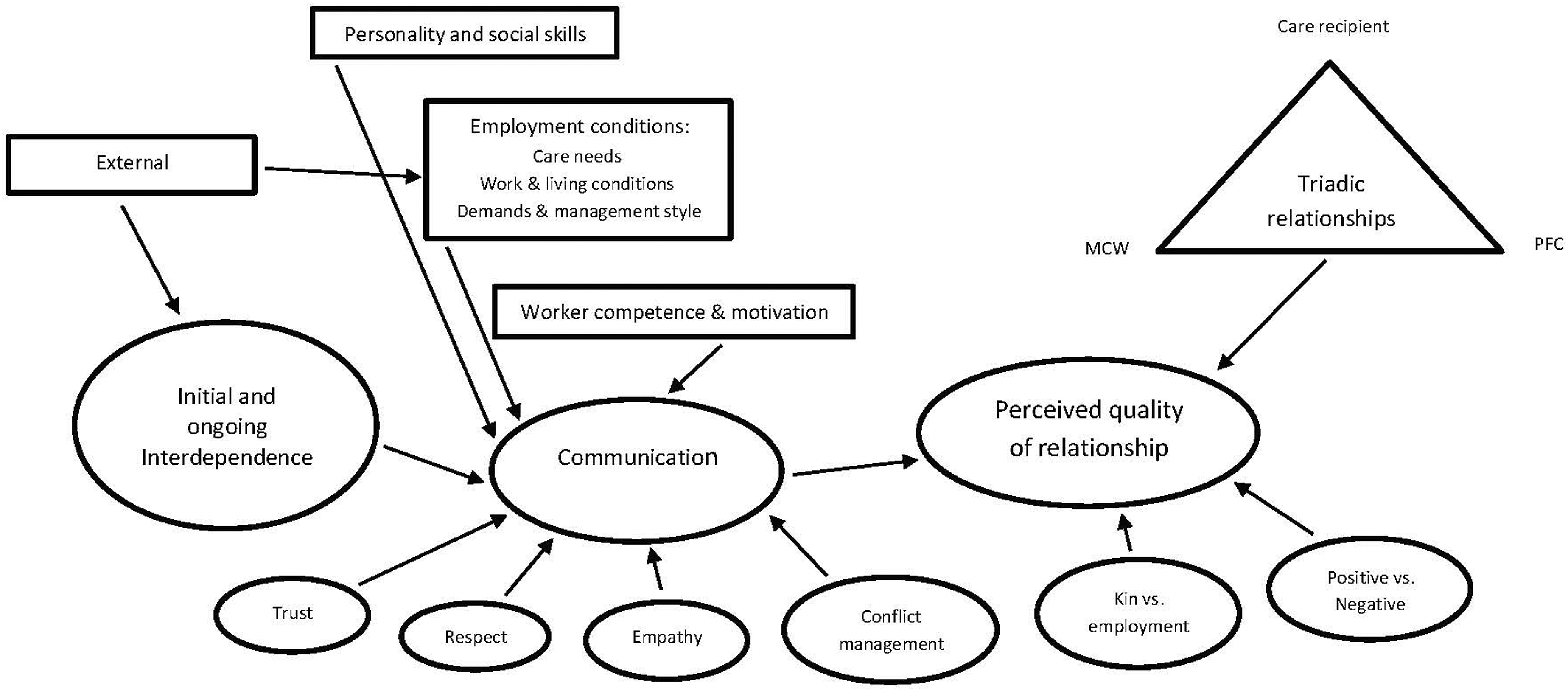
A high level of interdependence binds PFCs and MCWs together. PFCs are confronted by the need to provide care for a dependent relative, and MCWs face the challenges of non-citizens working in a difficult and highly regulated labor sector. Their respective circumstances require continuing overt and covert negotiations for the sake of providing quality care to frail older persons and assuring fair employment conditions for MCWs (see Walsh and Shutes (2013)).
Communications between PFCs and MCWs can involve trust, respect, empathy, appreciation, support, and conflict management. Feeling respected and/or trusted can be indicative of relationship quality. A combination of social skills—such as empathy, management style (e.g., demanding, abusive vs. accommodating), MCWs’ employment conditions, their motivation, and competence—all impact the relationship. The sum of MCW–PFC experiences results in a relationship level that can be characterized on an axis of quality as in kinship, versus classic employment, versus ambiguity, and on a quantitative axis of intensity. The present study is consistent with the Walsh and Shutes (2013) study that found that older care-recipients in Ireland and the United Kingdom highly valued love, compassion, kindness, and trust in their relationship with MCWs. The distinctions in relationship characteristics stem from our focus on MCWs and PFCs rather than on care-recipients.
The MCW–PFC relationship is affected by its respective interactions with the care-recipient. Sometimes, one aspect of the triad, such as MCW–care-recipient, affects the PFC–MCW dyad, or those relationships may be independent. A PFC’s recognition of a good relationship between the care-recipient and MCW may evoke the PFC’s appreciation that one’s relationship with the MCW can impact quality of care. Positive relationships that include support, companionship, instrumental support, and validation can have a salutary impact on the mental health of the older person and the PFC (Lauzier-Jobin & Houle, 2021) and enhance the social aspects of the care provided by the MCW (Cohen-Mansfield et al., 2019). Additional insight into aspects of the triadic relationship has been suggested by Xu et al. (2021). In the context of care by multiple family members, Xu et al. (2021) found that lower quality of family care coordination was associated with negative caregiver outcomes. Thus, coordination discord between PFCs and MCWs may impact the wellbeing of all parties, a topic warranting future research.
Further insight into the MCW–PFC–care-recipient triad can be derived from a study of experiences of dyads in situations involving serious illness (Persson et al., 2020), which revealed two meanings based on participants’ lived experiences of “being available” and “upholding continuity.” “Being available” was an essential characteristic of the “live-in” care provided by the MCW, though at times, there were complaints that the MCW was involved with others, for example, spending time on the phone or on the computer. “Upholding continuity” was more likely to be experienced in the relationship of the older person with the PFC. Both types of experiences were considered cornerstones of dignity in the context of caring for persons with serious illness.
The finding that PFCs tended to rate relationship quality more positively than did MCWs may be a manifestation of cognitive dissonance. Family members are often uneasy about hiring non-kin to care for close relatives. Conceiving of the MCW as kin might decrease guilt feelings concerning the delegation of responsibility for intimate and emotional care. The work of MCWs involves long hours, physical and emotional exertion, and sometimes performance of unpleasant tasks involving personal care for older adults who may be acutely ill and/or physically frail and/or cognitively impaired. When MCWs and PFCs perceive the triad as familial in nature, MCWs may be more accepting of their typically low wages, and PFCs may have less concern about whether they are unduly exploiting MCWs (Ayalon, 2009b).
There was a significant correlation between MCWs’ assessments of their relationship with the care-recipient and with the PFC, as contrasted with a lack of significant correlation between the PFCs’ assessments of their relationship with the care-recipient and with the MCW. The reactions of PFCs to MCWs may be impacted by the attitudes demonstrated by care-recipients concerning the MCW. Thus, MCWs perceived their relationship with the care-recipient and with the PFC as similar. In contrast to MCWs, the PFC’s relationship with the care-recipient is longstanding and unlikely to be significantly changed by the hiring of an MCW. Therefore, the attitudes of PFCs toward MCWs are perhaps more shaped by other factors, including the goal of helping the care-recipient, PFCs’ management style and expectations, and MCWs’ motivation, competence, social skills, and expectations.
The findings point both to similarities and discrepancies in MCWs’ and PFCs’ perceptions and the meanings they attribute to the quality of their relationship. Although PFCs and MCWs described positive and negative aspects, the most negative ones were raised by MCWs, including abuse and unfavorable employment conditions. Ehrenreich and Hochschild (2000) found that while MCWs might be viewed as “part of the family,” they could also be invisible, unless trouble arose. The gap in perceptions was particularly apparent when PFCs installed cameras to monitor MCWs’ and older care-recipients’ activities, where PFCs considered it a necessity to assure care-recipient security, and MCWs experienced it as an act of distrust and violation of privacy.
The findings suggest that many PFCs ignore aspects of MCWs’ lives, such as poverty, loneliness, disorientation in a new country, and the circumstances underlying their separation from homeland and family, sometimes involving leaving behind young children. Once the care-giving is in place, it may be adversely affected by language and cultural barriers, one of the findings of Walsh and Shutes (2013). However, Porat and Iecovich (2010) found that language was not a significant barrier to the quality of the relationship between care-recipients and MCWs. Rather, degree of similarity in personal qualities was found to be the most important determinant of closeness in those relationships. MCWs, who take on physically and emotionally rigorous care-giving work to improve their economic status, did not express recognition of the significant emotional and financial burden that providing care to older relatives poses for the typical Israeli, whose median take-home monthly wage as of June 2022 was equivalent to about $1,940 per month (Eretz, 2022).
Whereas the MCW–PFC relationship was most often characterized as positive, the overall situation was unbalanced between the party who provided a salary and gifts and the party who provided personal care services which most people eschew. The imbalance is most dramatically illustrated by the fact that MCWs’ visa status/work-permit status can be canceled by the Interior Ministry at any time. Thus, when asked about what things could be done to improve the MCW–PFC relationship, one MCW said, “I don’t know how to tell you,” and another, “Leave it,” and many others said “none.”
Trustworthiness of Findings
The trustworthiness of findings was initially established based on several methodological strategies, including multiple iterations in data analysis, use of multiple research staff to review, discuss, and revise the findings, and the use of a relatively large sample for the qualitative analysis. Trustworthiness was further established by repetition of themes across participant responses and by repetition of similar themes that emerged in the research of other investigators, where their focus involved the MCW–care-recipient relationship, for example, Porat and Iecovich (2010) and Walsh and Shutes (2013). The use of a grounded theory framework also contributed to trustworthiness of findings in that collection and analysis of data were not conducted with a preconceived sense of where the evidence might lead. Rather, the patterns that emerged were based on participants’ stated experiences. While the potential influence of individual bias cannot be dismissed, this research design, especially when employed with a relatively large sample, offers good prospects for yielding trustworthy findings involving the sensitive data our questions sought to elicit.
The analysis of trustworthiness follows that suggested by Stahl and King (2020). Credibility was established by (1) convergence with other research findings concerning this population (e.g., conceptualizing the MCW as kin as suggested in Ayalon’s research), (2) methodological triangulation through (a) the use of multiple research assistants for collecting the data and (b) collecting data from both sides of the relationship: PFCs and MCWs, (3) investigator triangulation through data analysis by multiple research staff, and (4) environmental triangulation by meeting participants in their preferred location, mostly in their homes, but also at other places. Transferability was bolstered by the large sample size and the inclusion of both quantitative results and qualitative findings. The large sample size resulted in many varied responses concerning MCW–PFC relationships, increasing the likelihood that the responses we elicited were representative of other dyads beyond our sample. Dependability was established by having a researcher, who was not involved in the analysis and writing, review, and comment on the paper. Confirmability was bolstered by our use of research staff who had no prior or subsequent involvement with the MCWs and PFCs beyond the interview itself.
Although this paper deals with the dyadic relationship of PFCs and MCWs, the approach taken was that of separate interviews (Eisikovits & Koren, 2010), which was more appropriate than joint interviews given the sensitive topics raised, such as challenging behaviors and questionable practices. Correspondingly, participant interview answers were not shared with the other member of the dyad, which further buoyed trustworthiness.
Ethical Considerations
Whereas the basic principles of ethical conduct in research are straightforward, such as receiving an IRB’s approval for conducting a study and obtaining informed consent from study participants, additional ethical considerations are important. A basic ethical consideration in qualitative research relates to accurate interpretation and trustworthiness of data when developing themes and interpreting data and findings, as detailed above. With respect to the proper interpretation of the findings, the authors’ intimate familiarity with Israeli society and frequent contact with MCWs and PFCs validated the findings such as the mutual dependency experienced between MCWs and PFCs, despite the seemingly “stronger” position of the PFC as the payer of services and provider of lodging. For most Israeli PFCs, the hiring of an MCW is an action taken only because no alternative solutions are available.
Another ethical challenge arises when participants report abuse. Given our promise to keep interview responses confidential, we did not act on any such reports. Participants whose responses indicated abuse appeared to be aware of the options available to them: reporting the matter to an abuse hotline established in Israel and/or resigning.
Limitations
Participants’ responses may have been biased by social desirability. This would be magnified in cases where privacy was limited during the interview, though most interviews took place in full privacy. Another limitation is that the sample consisted of those who voluntarily agreed to participate, which may have introduced selection bias. While some MCWs manifested great candor about the difficulties they faced, it is possible that some did not disclose problems because of their sense of dependence on the PFC or because they may not have trusted our assurance that their responses would be treated as fully confidential.
In this study, a dyadic thematic analysis was not used; that is, we did not analyze the responses of each dyad as the unit of analysis. Instead, the qualitative findings present themes raised by the respective members of each of the dyads. In order to perform an in-depth dyadic analysis, future research would need to organize the data in a quantifiable manner, addressing questions like, “What percent of MCWs shared the perception of PFCs with respect to the relationship being kin-like?”
Conclusion
This is the first study to specifically focus on describing and clarifying the relationship between PFCs and MCWs. It highlights the complexity of MCW–PFC relationships and reveals multiple layers of perception, as found in ratings of (1) quality by each member of the dyad and the gap between those, (2) types of communication involved, (3) perceived quality of relationship as kin-like or employment-like or a process in which both aspects are present or rejected, and (4) organization of the relationship according to the perspective of each dyad member’s relationship with the care-recipient. Whereas most respondents rated the relationship as positive, they also articulated room for improvement. In exploring ways to improve the relationship, the study’s theoretical framework provides an initial map suggesting paths that should be explored, including such processes as: • Perceptions of interdependence and reframing them in a more positive and useful way. • Social skills of one or both members of the dyad, with particular emphasis on effective communication, such as practicing respectful speech, enhancing empathy for the other party, establishing tools for conflict management, and exploring ways to develop and manifest appreciation of the other. • Background variables impacting the relationship that offer opportunities to improve the relationship by addressing deficits in those areas, such as: • Improving employment conditions for MCWs, including work and living conditions. • Enhancing management style and competency of PFCs. • Clarifying perceptions regarding the nature of the relationship, that is, kin or employment or another model, and decreasing gaps in those perceptions. • Enhancing MCW competence by offering mentoring in deficient areas.
Pursuing these paths for improving the PFC–MCW relationship will likely benefit the wellbeing of both parties, and that of the older care-recipient whose needs brought the PFC and MCW into their relationship. Can potential difficulties be screened at the beginning of the service period, and can certain interventions prevent some conflicts before they emerge? That needs to be explored in future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Minerva Foundation [grant number: 3158329500].
Ethical Approval
This study was approved by the Tel Aviv University Institutional Review Board without a specific approval number. Written informed consent was obtained from all participants.