
Abstract
Sudden disruptions to the social environment of older adults living alone, such as the COVID-19 pandemic, can challenge their ability to maintain well-being. This study employed an interpretative phenomenological analysis to explore how Dutch older adults (≥65 years) living alone maintained their well-being during the COVID-19 pandemic. Between June and October 2021, we conducted 20 semi-structured interviews with older adults living alone in the Netherlands. Participants were recruited through online newsletters and home care and social work institutions. We identified three key themes. The theme “Filling the void of being alone” captures participants’ ongoing search for a sense of connection, and the challenges they faced related to social exclusion. The theme “Navigating challenging situations to maintain well-being” illustrates participants’ struggle with disrupted daily routines and how they tried to regain a sense of control to stay well. Lastly, the theme “Reverberating echoes of the past” conveys how participants’ life histories shaped their responses to the pandemic and the role of acceptance in this process. Overall, our results highlight great individual variability in how older adults living alone maintained their well-being during the COVID-19 pandemic. This underscores the need for interventions and support strategies that accommodate the unique needs of older adults living alone when opportunities for social engagement are limited.
Keywords
Background
Due to advancements in healthcare, improved living conditions, and declining birth rates, the population is ageing in the Netherlands (Statistics Netherlands, 2021). This demographic shift presents challenges for healthcare, affecting the accessibility and quality of care for older adults (Beard et al., 2016). To help older adults remain independent of care for as long as possible, Dutch health policies aim to promote their well-being (Ministry of Health, Welfare and Sport, 2020).
Well-being is understood from both hedonic and eudemonic perspectives as a state where individuals experience happiness, life satisfaction, and a sense of purpose, extending beyond the mere absence of disease (Klausen, 2020; Steptoe et al., 2015). Compared to younger age groups, older adults’ well-being depends to a large degree on their ability to adapt to age-related changes, such as reduced functionality, cognitive decline, and the loss of peers (Klausen, 2020). Consequently, maintaining well-being in later life is not about returning to a previous state of happiness but rather about adjusting to new circumstances through reinterpretation and coping strategies (Klausen, 2020).
An increasing number of older adults in the Netherlands are living alone (Statistics Netherlands, 2024). This trend raises concerns about well-being, as living alone has been associated with increased loneliness, greater functional loss, poorer health, and financial strains (Fernandez-Portero et al., 2023; Gaymu et al., 2012; Ng et al., 2015; Pasanen et al., 2021). These disadvantages often arise from a lack of social support and meaningful interaction, both of which heighten the risk of social isolation (Nicholson, 2012). In turn, social isolation is a significant risk factor that exacerbates negative health outcomes and threatens the well-being of older adults (Holt-Lunstad & Steptoe, 2022).
While often related, it is important to recognize that living alone does not necessarily equate to social isolation (Karakayali & Azizoglu, 2025; Klinenberg, 2016). Qualitative studies have provided important nuances in this regard. For some older adults, living alone fosters a sense of autonomy and self-determination. This enables them to engage in activities that promote their well-being, such as maintaining social connections, pursuing hobbies, and managing daily life independently (Cederbom et al., 2014; Soulières & Charpentier, 2022). However, those facing disadvantages such as financial constraints, health issues, or mobility limitations may struggle to access the resources and support they need to maintain well-being (Soulières & Charpentier, 2022). Altogether, diverse and stable social networks that foster social support and strong connections are beneficial to the well-being of older adults living alone (Djundeva et al., 2019; Fernandez-Portero et al., 2023).
Sudden disruptions to the social environment can interfere with older adults’ ability to stay well (Cederbom et al., 2014; Schafer et al., 2022; Steijvers et al., 2024). A major example of such disruption was the COVID-19 pandemic. To curb the spread of the COVID-19 virus, governments implemented social distancing measures. In the Netherlands, these measures involved keeping a distance of 1.5 m from other people at all times and multiple periods of mandated social isolation. Because older adults were at high risk of adverse health outcomes from infection, they were strongly encouraged to follow these restrictions (Shahid et al., 2020).
The social distancing measures negatively affected older adults’ well-being due to increased loneliness, reduced physical activity, and worsening mental health issues (Besselink et al., 2024; De Pue et al., 2021; Karmann et al., 2024; Lebrasseur et al., 2021; Sepúlveda-Loyola et al., 2020). The risk of adversities in well-being was especially pronounced for older adults living alone, as they faced a sharp decline in in-person contact and greater loneliness than those living with others (Fingerman et al., 2021; Hendriksen et al., 2021). Nonetheless, studies on the lived experiences of people living alone during the pandemic give mixed results. For instance, while some women living alone in Slovakia struggled with loneliness, others engaged in self-reflection and new social strategies (Kamin et al., 2021). In Austria, older adults living alone found daily life and engaging in support systems more challenging but did not view the pandemic itself as a direct threat (Pfabigan et al., 2022). Together, these studies emphasize the individual variability in how people living alone adapted to the isolation imposed by the pandemic.
While most COVID-19 measures were lifted by the end of 2022, future scenarios requiring older adults to self-isolate are not unlikely. For example, due to climate change, extreme weather (e.g., heatwaves and heavy rainfall) is becoming more frequent, often forcing older adults to isolate for safety reasons (Clarke et al., 2015). By reflecting on the pandemic’s impact, strategies can be developed to support older adults living alone in future crises, ensuring their well-being and social connectedness even in times of isolation.
This study explores how older adults living alone in the Netherlands maintained their well-being during the COVID-19 pandemic. To capture the complexity of their experiences, we used interpretative phenomenological analysis (IPA), which enabled us to explore how personal narratives and contextual factors shaped well-being (Lopez & Willis, 2004; Smith et al., 2022). By closely examining the lived experiences of older adults living alone, this research provides valuable insights that can inform future policies and interventions aimed at promoting older adults’ well-being in circumstances where opportunities for social engagement are limited.
Methods
Design
In this study, we aimed to deepen the understanding of how older adults living alone maintained their well-being during the COVID-19 pandemic through IPA. IPA is a qualitative methodology that emphasizes understanding how individuals make sense of their lived experiences within their unique context (Smith, 2018). IPA is distinguished by its idiographic approach, focusing on the detailed exploration of individual cases before making broader generalizations.
This method allows for an in-depth examination of participants’ personal and subjective experiences, recognizing that their perspectives are shaped by their contexts, backgrounds, and the meanings they attach to their experiences. A key feature of IPA is its use of the double hermeneutic, where the researcher interprets the participants’ interpretation of their own experiences. By integrating both a phenomenological focus on individuals’ lived experiences and an interpretative lens that considers the researcher’s role in understanding those experiences, IPA provides a nuanced approach to exploring complex phenomena such as living alone during the pandemic (Smith et al., 2022).
Sampling Strategy and Recruitment
Participants eligible for the study were older adults, aged ≥65 years, living alone during the COVID-19 pandemic. We used purposive sampling, and participants were excluded if they were unable to verbally communicate in Dutch, lived together with other people, and/or did not match the age requirement.
Participants were recruited between June and September 2021. These were months in which the Dutch society was reopened after a second lockdown, which included three months of strict measures limiting social gatherings (e.g., a curfew and a maximum of one visitor). Recruitment was conducted via online newsletters and (social) media channels, which included information about the study’s purpose and contact details for participants to sign up for an interview via phone or email. To reach participants who were less accessible through an online approach, home care and social work institutions were asked to distribute a paper version of the information letter to eligible clients. The paper version included a sign-up form and a return envelope to mail to the primary researcher.
The researchers and participants initially spoke on the phone. During the call, the researcher explained the study’s purpose and assessed the eligibility of the participant. If the criteria were met and the participant provided verbal consent, an interview appointment was scheduled.
We aimed to sample a group of participants that represented the heterogeneity of community-dwelling older adults who live alone. We considered the sample sufficient when we had interviewed individuals of different ages, residing in both rural and urban areas.
Data Collection
Recruitment and data collection took place simultaneously, meaning that while the first interviews were conducted, participant recruitment continued. The interviews were conducted by two experienced qualitative researchers (DB and FDS). Depending on the participant’s preference, interviews were conducted in person at the participant’s home or via video or phone call. Before the interview, all participants were asked to read and sign an informed consent form. The interviews were conducted in Dutch, lasted approximately one hour and were recorded using an audio device.
To allow participants to tell their stories, we conducted semi-structured interviews. The interviews covered the following topics: changes in well-being and lifestyle, support needs related to maintaining well-being, dealing with challenges to well-being, and advice for staying well.
Conversations began with the question, “Can you describe how you experienced the COVID-19 period?”. Following this initial question, topics from the interview guide were touched upon iteratively rather than linearly. This enabled researchers to focus more thoroughly on the conversation, allowing discussions to be guided by participants’ priorities and concerns. If the participant was hesitant to answer, gave short or tangible answers, or needed more encouragement, the interviewer used prompts.
From the start of data collection, DB and FDS frequently discussed the content of the collected data. If early ideas subsequently reappeared in multiple interviews, the interviewers adjusted their focus in later interviews or adjusted the topic list. An example is the addition of the topic “changes in relationships to family/children” to the topic list.
Once all the data were collected, interviews were transcribed verbatim by a transcription agency. To ensure confidentiality, data were shared via encrypted file transfer. The agency stored the transcripts on password-protected, encrypted servers with access restricted to authorized researchers. Once transcription was completed, the agency deleted all data within 30 days. The principal investigator (DB) securely transferred the data to the researchers’ institutional server, where the data were anonymized and stored in compliance with institutional data protection regulations. Translation to English for reporting was conducted in the final stage of drafting the manuscript and was reviewed by a native English speaker.
Data Analysis
Once all interviews were conducted and transcribed, the software ATLAS.ti 23 was used to assist in the analysis (ATLAS.ti Mac (version 23.4.0), 2023). The analyses were guided by the heuristic framework for analysis described by Smith et al. (2022), which is considered a suitable framework for qualitative research in the field of social, health, and behavioral sciences (Newberry, 2011; Smith et al., 2022). Following the principles of IPA, transcripts were analyzed on a case-by-case basis to explore the personal perspectives of individual cases before moving on to general claims in the form of overarching themes. Through this approach, the convergence and divergence in participants’ experiences were analyzed. This allowed us to identify common patterns as well as unique differences in how participants maintained their well-being during the pandemic.
The analysis of single cases consisted of three consecutive steps. The first step involved exploratory noting, in which the transcript was analyzed line by line and divided into meaning units, referred to as exploratory notes. The exploratory notes were developed inductively and functioned as a label to depict what the experience was about.
The second step involved a shift from raw data to working primarily with exploratory notes. In this step, experiential statements were developed, involving a concise and comprehensive summary of exploratory notes that described a specific experience and its meaning given to the experience. Doing so, the narrative flow of the transcript was broken up to analyze interwoven connections in the participant’s data. The experiential statements aimed to explain larger segments of the data, sorted into higher-order categories and on a more interpretative and abstract level.
In the last step of the single transcript analysis, experiential statements were moved around and clustered to map and compile interconnections between the statements, referred to as personal experiential themes (PETs). PETs were given a title, describing the core characteristics of the cluster. When all three steps were completed within the single transcript, the analysis moved to the next individual case. This was done until all 20 transcripts were completed.
When all transcripts were analyzed case by case, the analysis progressed to the final phase: the cross-case analysis. The process was started by scanning all PETs of individual cases to seek convergence in participants’ experiences. In doing so, emphasis was laid on both similarities and differences in the unique individual ways participants reflected upon common experiences. This was a dynamic process in which the context and detail of experiences were checked out by going back and forth between PETs, experiential statements, and exploratory notes. The cross-case analysis led to a set of group experiential themes (GETs). GETs are overarching themes that entail a description of convergent and divergent cross-case patterns in the dataset. From now on, we refer to GETs as “overarching themes.”
Rigor and Reflexivity
The research group consisted of seven scientific researchers, all experienced with qualitative research. Three researchers (DB, FDS, and FvdL) are specialized in public health with a focus on the promotion of health and well-being among older adults and people with disabilities. MJS and HJ-W are specialized in health and nutrition among older adults. EJF is specialized in nursing care for older adults, and SJGG is specialized in implementation science and qualitative methods.
The entire research process was guided by methodological principles of openness, questioning our pre-understanding, and adopting a reflexive attitude. With openness, we mean that we emphasized an open stance toward the participants’ lived experiences during the COVID-19 pandemic. To do so, our pre-understandings of the phenomena were questioned repeatedly and documented through writing bracketing notes.
From the start of data collection, DB and FDS met on a biweekly basis. During these meetings, they moved back and forth discussing given parts of the data and the whole. This way, one’s relationship to the data became apparent and was taken into consideration when further interpreting the data. Additionally, while the data analysis progressed, multiple interdisciplinary moments of revision were organized to discuss the data in a broader term and enhance triangulation. During these meetings, exploratory notes, experiential statements, PETs, and overarching themes were discussed and reorganized. This process of querying the data contributed to adopting a reflexive attitude and enhanced the trustworthiness of the study.
Ethical Considerations
Our study was approved by the affiliated board of ethics, Hanze Ethical Review Board, Heac.2021.009. Before the interviews, all participants received an information letter and oral information. All participants provided both verbal and written informed consent prior to the study. As interviews could touch upon distressing life events and memories, DB and FDS always emphasized at the start of the interview that the interviews could be paused or ended at any moment. Moreover, protecting the identity of the participants was one of our primary concerns. Therefore, personal details were deleted from transcripts, and original data were only accessible for DB and FDS. All data, including audiotapes, transcripts, and informed consents, were stored in a secure digital environment of the research institute and will be saved for at least 15 years.
Results
Participant’s Characteristics (N = 20).
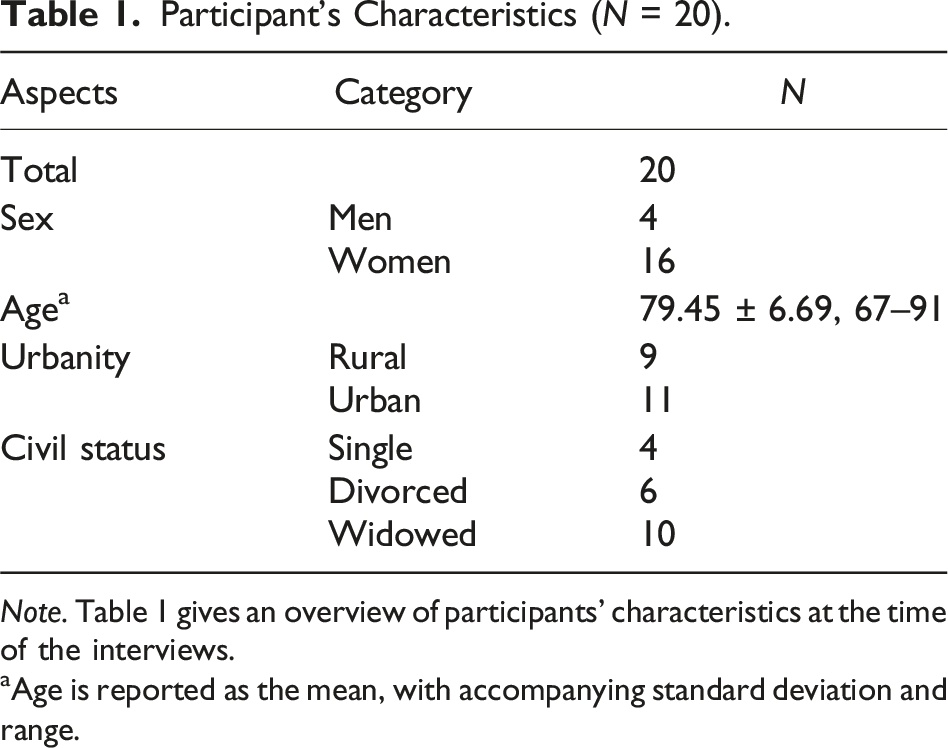
Note. Table 1 gives an overview of participants’ characteristics at the time of the interviews.
aAge is reported as the mean, with accompanying standard deviation and range.
We identified three overarching themes that describe how older adults living alone maintained their well-being during the pandemic. These were “Filling the void of being alone,” “Navigating challenging situations to maintain well-being,” and “Reverberating echoes of the past.” The theme “Filling the void of being alone” captures how participants grasped for meaningful connection to stay well and faced challenges related to social exclusion. The theme “Navigating challenging situations to maintain well-being” illustrates how disruption of daily routines unsettled participants and how they regained a sense of control to stay well. Lastly, the theme “Reverberating echoes of the past” delves deeper into how past experiences continued to have an impact on participants’ well-being during the pandemic, and the role of acceptance. Figure 1 gives an overview of overarching themes and how they are related to one another. An overview of the overarching themes and how they are related to another.
Theme 1: Filling the Void of Being Alone
Participants described the pandemic as a silent and solitary time, during which they searched for ways to stay connected with their surroundings and other people despite being alone. Feeling close and connected with others and their surroundings was a prerequisite to maintain their well-being, yet the absence of spontaneous social encounters made this challenging. The sub-themes “Grasping for connection” and “Burdened by social exclusion” illustrate participants’ continuous efforts to find a sense of connection to fill the void of being alone.
Grasping for Connection
Participants described how the social distancing measures affected a sometimes already fragile balance of social connection. This made them increasingly aware of their need for meaningful interactions with others and their surroundings to maintain their well-being, especially because they lived alone. Both participants 6 and 2 related living alone to a heightened vulnerability to social isolation. Participant 6 became painfully aware of her solitude when the pandemic started and described the sudden shift in her social life as “falling into a deep hole”: I’m on my own, so I spent a lot of time at home alone, and for someone who’s always busy and constantly on the go, suddenly being stuck at home was a very deep void. (Participant 6, a 77-year-old woman)
Similarly, for participant 2, staying in touch with other people was a big part of her life. She expressed that without such social interaction, she would be miserable. To prevent this, she actively sought ways to hold onto social ties, forming a pact with her neighbors to create a sense of togetherness despite social distancing rules: I made an agreement […] with my neighbours right away: we all live under one roof, so now we are one household. It’s so much easier that way, being able to at least pop in on one another at any time […] And yes, I more or less followed the guidelines, but if you’re alone and er … you stick to the rules a 100%, you would have become utterly miserable. (Participant 2, a 67-year-old woman)
For participants who had already experienced a shift toward a more solitary lifestyle before the pandemic, declines in their social environment were a familiar process. This was the case for participant 9, who explained how the pandemic did not introduce a new sense of isolation, but rather amplified an existing one. Losing his wife eight years before the start of the pandemic had left him grappling with feelings of social isolation and loneliness. Rather than seeing the restriction as a new source of isolation, he viewed them as a painful reminder of his loss, amplifying the solitude that had already become part of his life: But lonely, yeah, […] I mean, there’s just nothing in it. Eh, you go to bed at night, you’re alone. You get up in the morning. There’s no one saying anything. (Participant 9, an 83-year-old man)
This was similar for participant 8, who reviewed the pandemic as a sharp contrast to a once socially rich life. Having owned a local bookstore for nearly three decades, she was accustomed to daily interaction and a sense of purpose tied to her community presence. The pandemic limited her social life even more and accelerated an ongoing process of isolation that had already begun when she stopped working. The contrast between the past and the present was a painful reminder of what she had lost, making the enforced restrictions feel like an intensification of an already existing decline in social connections: And I must not forget, until two years ago, I owned a bookstore in [names the village] for 29 years, so that was a very different life. But I had to stop that because I could no longer walk there, and I had no other means to get there. Then, I was surrounded by other people every day, so that’s a huge difference. (Participant 8, a 92-year-old woman)
For some participants, the need for connection was not necessarily tied to social interaction with other people but rather to maintaining a sense of presence within a community. For example, participant 18 explained that her sense of connection was found in shared spaces and public activities, such as going to the theatre. The closure of public spaces and communal activities during the pandemic prevented her from engaging in such shared experiences, leaving her frustrated that the government overlooked older adults’ needs when deciding which restrictions to lift: And then, we weren’t allowed to go to a museum. Well, you know, museums are often visited by older people, and well, they certainly don’t go bumping into one another. But they [refers to museums] stayed closed, you know, they just stayed closed. And then, for example, football stadiums were allowed to open, things like that just don’t make sense. (Participant 18, a 75-year-old woman)
In contrast, participant 3 had gradually embraced solitude as a natural progression of ageing, making the pandemic’s restrictions less impactful on her well-being. She described her needs to stay well had already shifted away from a socially active life, finding contentment in solitary activities: But yes, I’m 88 now, so you don’t need to do as much anymore … I do a lot of puzzles and I follow all kinds of sports, well, almost everything, including football, tennis, the Tour de France, you name it. So I never get bored. (Participant 3, an 88-year-old woman)
On top of the emotional impact of social distancing measures on their well-being, some participants express how the lack of casual, physical touch affected them. As they relied on interaction with friends, family, and community members for affectionate contact, they suddenly faced losses in physical intimacy when restrictive measures prohibited physical touch with people outside of the household. This was exemplified by participant 12, who was very close to her grandchildren, describing how the inability to hug them left her longing for physical closeness: There is a monastery here in [name of city], and they ran an exhibition about skin hunger. […] And then I thought: that’s what I have, skin hunger. When you don’t have anyone around …, because my grandchildren too, I didn’t see them anymore, and I used to cuddle with them and so on. And well, then I thought, yes, I have skin hunger […] I missed that a lot, but yeah. (Participant 12, a 77-year-old woman)
Similarly, participant 2 became acutely aware of the significance of physical touch for her well-being. She reflected on how living alone during the pandemic heightened this awareness and emphasized that older adults without children might have different needs for maintaining well-being compared to those with family support: I'm single, and at one point I realized that I hadn’t touched anyone in over nine months, no one, zilch. And I think that’s something people often forget, especially with older people who end up alone, and those who do have children still have a fair bit of contact; people took grandchildren on their laps all the time and so on. But someone who lives a single life has no physical contact at all. That is quite a problem. (Participant 2, a 67-year-old woman)
Burdened by Social Exclusion
Although participants recognized the importance of the restrictions to prevent infection, the restrictive measures contributed to feelings of social exclusion, amplifying their feelings of disconnection from society. For example, participant 4 reflected on how the stigmatizing language used about older adults in the media during the pandemic negatively impacted her self-worth. She felt the portrayal of the elderly as a burden and felt unacknowledged: Yes, let them [refers to the government] stop talking so much about the elderly, because, um, I do feel that we, the grey-haired, right … Once you have grey hair, it’s almost as if you’re a burden. Yes, it’s always like the elderly cost so much money and so on. And it makes me think: you almost feel like you’re not supposed to be here at all. (Participant 4, an 81-year-old woman)
Participant 9, who already had little contact with his family before the pandemic, experienced not being invited to family birthdays as a rejection. The lack of invitations left him feeling forgotten, undermining his desire to remain connected with his family: But yeah, it’s, it’s really quiet, right? Because there was no one who, who still wanted you at their birthday. […] Not that I would go to every birthday party, but then you still have a bit of contact, right? (Participant 9, an 83-year-old man)
Similarly, participant 8 described how the lack of visitors during the pandemic highlighted her isolation. She expressed how the absence of social interactions led to feelings of sadness and rejection: It saddened me. Yes, I thought: well, am I completely left out now because no one is coming? Not that I would sit and cry for hours, but yeah, I’ve cried sometimes, thinking: darn it, I don’t enjoy this at all. (Participant 8, a 92-year-old woman)
Participant 11 reflected on the lack of reciprocity in social relationships during the pandemic. She suspected this was because people viewed her as self-sufficient and resilient. After all, she was used to being alone. Although she was proud of her independence, the assumption of others frustrated her and made her rethink the value of existing social relationships: And um, people didn’t call me that often. And then I think, why not? Maybe, um, I often have the idea of “Well, she’ll manage.” But I could really use a chat and things like that too. But what eventually happens, and this is actually still happening, is that I say, “Yes, um, look, I won’t keep doing this.” It is all too one-sided. (Participant 11, a 74-year-old woman)
Theme 2: Navigating Challenging Situations to Maintain Well-Being
This theme explores how participants navigated challenges brought by the pandemic to maintain their well-being. The subtheme “Unsettled by the breakdown of daily routines” highlights different ways in which the disruption of daily routines impacted participants’ well-being. The subtheme “Regaining a sense of control” illustrates how participants tried to regain a sense of control to be able to fulfil their needs to stay well.
Unsettled by the Breakdown of Daily Routines
The pandemic induced disruptions of long-established daily routines that had supported the well-being of participants. This disruption unsettled participants, affecting their emotional and physical well-being. Participant 4 described how a rapid cascade of events during the start of the pandemic affected her emotionally, taking over her daily life: At the start of the pandemic, I kept track of everything. Um, like all the statistics and such. Well, I was working on that for a while, and, oh, I was teary. And emotional. (Participant 4, an 81-year-old woman)
Participant 1, who was used to going to the gym, explained how the breakdown of routines affected his efforts to stay physically fit. Before the pandemic, he had a routine that helped maintain his fitness, but once disrupted, the lack of structure left him less motivated to continue. Even when gyms were reopening, he decided not to return: I used to go to the gym for an hour once a week, just to get some exercise and do a bit of cardio. Then the news came on the radio about the situation becoming alarming […]. And I haven’t gone since. (Participant 1, a 79-year-old man)
This hesitation to re-engage in activities after restrictions eased was also explained by participant 11. For her, a core element that caused hesitation to pick up daily activities was fear for infection. Despite lifted measures, she decided not to go swimming anymore because it did not feel safe: Well, I used to go swimming once or twice a week. So I, also, um, did sports twice a week. Well then, that stopped as well. And er, then later they said, “Well, it’s okay to go again now.” And then I was like, “Yeah, I just don’t trust it.” (Participant 11, a 74-year-old woman)
Nevertheless, the breakdown of daily routines during the pandemic was not necessarily related to restrictive COVID-19 measures. This was exemplified by participant 14, who lost her husband in the first months of the pandemic. While mourning her loss, she did not leave the house as much as she used to. For her, this meant that she performed less physical movement compared to when her husband was still there: If you go out less, of course you move less, but, uh, yeah … Yes, your activity naturally decreases, that’s just how it is. (Participant 14, a 77-year-old woman)
Participant 18 elaborated on the accumulation of multiple factors that led to a decrease in her physical activity during the pandemic. These factors were both pandemic-related stressors and health problems that arose when growing older. While she was confronted with these health problems, she noticed herself moving less: Um, well, uh, I do think I’ve been moving less, but that also has to do with my, um, health condition, because it all got a bit mixed up, you know. (Participant 18, a 75-year-old woman)
Regaining a Sense of Control
Part of navigating challenging situations during the pandemic was looking for ways to regain a sense of control. How participants did this was shaped by personal circumstances.
For some, like participant 2 and participant 7, living alone much of their lives had instilled a strong sense of independence. They viewed decision-making as a personal responsibility, sometimes choosing to bend the rules to prioritize their well-being. Their autonomy allowed them to assess the restrictions critically and act in ways that aligned with their needs to stay well. Participant 7 explained that if the measures affected her daily life too much, she kept control by consciously choosing not to adhere to them: I basically just went my own way. We only encountered the issue that if I visited somewhere, like a couple, they weren’t allowed to return the visit together. Well, then we said “That’s nonsense.” So we still did that back and forth. But no more than two persons here, or me there. Because that doesn’t make any sense. (Participant 7, a 71-year-old woman)
Participant 2 found it important to look for alternative ways to fulfil social needs during times of restrictive measures. For her, adapting to the restrictions meant actively seeking the boundaries of what was permitted, prioritizing emotional well-being over strict adherence to the rules: Find the limit of what is allowed and what is not, and if crossing the limit means you feel less lonely, then do it. Mental health is at least as important as your physical health. (Participant 2, a 67-year-old woman)
In contrast, participant 3 found control in adhering strictly to government guidelines, seeing compliance as part of her duty as a responsible citizen. Her sense of control came from following external guidance rather than redefining boundaries herself: Well, I’ve always followed everything that the government, uh, the discussions and the explanations, yes, I follow all the advice. So, you just follow the advice. Sticking to the rules is the main thing. (Participant 3, an 88-year-old woman)
Some participants experienced an initial loss of control when restrictive measures were implemented. Taking back control was a way to regain agency and foster their well-being. This was done very consciously by participant 13. She described regaining control as a gradual process, first surrendering to uncertainty and later reclaiming her control: I initially just let it all wash over me, thinking it is what it is and I can’t do anything about it, and, um, gradually I tried to get back on my feet. That’s how I looked at it. (Participant 13, an 83-year-old woman)
Another example was given by participant 11, who struggled with disrupted sleep patterns and unhealthy habits when the pandemic started. Eventually, she recognized the need to take control of her behavior to stay well: But what I did do was go to bed early in the evening, and then I’d be awake in the middle of the night. I first would also watch some TV, because I have a television in the bedroom as well. And, uh, then, yes, in the morning I hadn’t slept for hours. So I’d just drink tea and, eh, do things like that. And then I thought, “Well, now you’re really messing up.” (Participant 11, a 74-year-old woman)
For some, the ability to regain control was tied to pre-pandemic experiences of loss. Participant 20, who had lost her husband before the pandemic, had already been through a profound shift in autonomy. She had learned to make decisions independently and navigate life without a partner, which equipped her to approach the restrictions with a similar mindset: Because you’re alone, yes, fortunately I have my children, but because you’re alone, you don’t have the option to consult with your partner whether to go for a walk or do this or that. But when you’re alone, it works differently, you get better at making decisions yourself. (Participant 20, a 91-year-old-woman)
Theme 3: Reverberating Echoes of the Past
Reverberating echoes of the past were apparent across participants’ narratives, with their personal histories shaping how they experienced and reacted to the pandemic. For some, the lessons learned over a lifetime provided strength and resilience, while for others, the pandemic triggered the resurfacing of long-buried emotional distress.
Participant 10 portrayed how she relied on resilience built through earlier hardships in her life. Having previously learned to entertain herself during extended periods of limited social interaction, she approached the pandemic with a sense of acceptance and adaptability. One example she elaborated on was when she was bed-bound due to polio as an eight-year-old. During the pandemic, she benefited from her capability to entertain herself when being alone: And I am incredibly good at being alone because, well, when I had polio, I was 8. Well, then I spent a year alone in bed. There is really no one with you the whole day […] but I never got bored, and I still don’t. (Participant 10, a 76-year-old woman)
Similarly, participant 5, a man who had been single his whole life, explained how past experiences of hardship instilled a mindset that helped him to adjust to the restrictions without feeling overwhelmed. Drawing a parallel between the pandemic to a long, challenging walk, he explained how the lessons learned during these walks provided him with a sense of purpose and the strength to navigate difficult times: Well, I’ve learned from the past, I used to walk a lot, long hikes of 40, 50 kilometres, because that’s what I always used to do. And from those days I’ve taken away the mindset of “turn off your brain and keep your eyes on the horizon.” And then you’ll make it. That’s what life is about after all. (Participant 5, a 79-year-old man)
In contrast, other participants were confronted with memories from their past that affected their well-being negatively. This was portrayed by participant 16, who had experienced the Second World War as a small child. While she was only three years old when it ended, she retained memories of the wartime oppression, which were evoked by the isolation and restrictive measures during the pandemic. Unlike those who leaned on life lessons, she struggled with the echoes of past suffering: What affects me is just the unfairness of it all, or the meanness towards people, fellow human beings. And especially as an older person who has experienced a fair bit of the Second World War, it’s like reliving that time. (Participant 16, a 79-year-old woman)
Despite these differences, there was a common theme of acceptance among participants. Whether through past resilience or forced adaptation, many recognized the necessity of accepting what could not be changed. This was portrayed by participant 2: Sometimes that makes you a bit sad, thinking “Hey, that’s not possible for a while …” but apart from that, I could just move past it fairly quickly. At a certain point, I said, “Yes, that’s just how it is for now.” (Participant 2, a 67-year-old woman)
Participants’ ability to accept difficult situations stemmed from a lifetime of managing various stressors and adapting to changes. This was exemplified by participant 10, who used acceptance to reduce suffering. She explained how people should not expect a life without hardship, as this is part of life. Through this attitude, she was able to find contentment in the challenges brought by the pandemic: Don’t complain about what you can’t do. Be happy with what you can do, because there’s still so much possible. But a lot of people are indeed reminiscing: “Yes, back then I could do this, and why is this happening to me?” We never said that here, even though we’ve been through enough misery. But then I would say, why shouldn’t we experience some hardship? Everyone experiences hardship, right? It’s a part of life. (Participant 10, a 76-year-old woman)
Discussion
This study aimed to deepen the understanding of how older adults living alone maintained their well-being during the COVID-19 pandemic in the Netherlands. Our analysis identified three overarching themes. The first theme illustrates participants’ ongoing search for a sense of connection to fill the void of being alone. The second theme illustrates participants’ shared struggle with disrupted daily routines and how they tried to regain a sense of control to stay well. The third theme conveys how participants’ life histories shaped their responses to the pandemic, with some drawing strength from past hardships while others faced resurfacing traumas. The acceptance of life’s challenges played an important role and was a common feature in maintaining participants’ well-being.
Participants’ narratives highlighted a profound need to feel connected to and be recognized by society to maintain their well-being. Their need for connectedness was deeply rooted in experiencing a sense of belonging, which is fundamental to the well-being of older adults (Cramm & Nieboer, 2015; Flett & Heisel, 2021; Jarrett et al., 2022; Martin Mau & Klausen, 2022; Tiilikainen et al., 2021; Whitehead & Torossian, 2020). The deprivation in physical and social contact during the pandemic affected older adults’ sense of belonging regardless of living situation (Derrer-Merk et al., 2024). Notably, the activities that fostered meaningful connections among our participants did not always require direct social interaction. Consistent with previous research, our findings suggest that experiences of meaningful connection also involve passive community engagement, such as being in public spaces (Duppen et al., 2020; Levasseur et al., 2010; Sirén et al., 2023). Our findings highlight that, in future situations requiring social distancing, the well-being of older adults living alone can be supported through strategies that facilitate non-physical forms of connection.
An important finding was participants’ reluctance to resume out-of-home activities even after COVID-19 restrictions were lifted. This hesitation stemmed from ongoing fears and shifting social dynamics, aligning with previous research (Finlay et al., 2024; Krendl & Perry, 2021). While the oldest old, individuals with chronic diseases, and those living alone were particularly vulnerable to reduced out-of-home activities early in the pandemic, less is known about whether these declines persisted over time and how they may have shaped long-term behavioral patterns (Finlay et al., 2024). Nonetheless, engagement in out-of-home activities is crucial role for older adults’ well-being, helping to reduce the risks of cognitive decline, depression, loneliness, sarcopenia, and chronic disease (Niedzwiedz et al., 2016; Saraiva et al., 2021; Townsend et al., 2021; Yu, 2025). Therefore, our finding that these reductions persisted beyond the lifting of COVID-19 restrictions raises concerns about the pandemic’s lasting impact. Taken together, our results suggest that the effects of social distancing measures extend beyond infection prevention, potentially leading to declines in community engagement among older adults living alone (Finlay et al., 2024; Smith et al., 2020; Valérie-Anne et al., 2024).
To a large extent, the meaning participants assigned to living alone shaped how they maintained their well-being during the pandemic. Those who actively chose to live alone or had been doing so for a long time related their living situation to a source of self-reliance and personal agency. Their appreciation of living alone aligns with coping strategies tied to autonomy, empowering individuals to take control over their circumstances (Karakayali & Azizoglu, 2025; Klinenberg, 2016; Soulières & Charpentier, 2022). In contrast, participants who were adjusting to living alone found solitude difficult, regardless of the pandemic. Their strategies focused more on managing feelings of loneliness, seeking external support, and adapting to the absence of a shared daily life, rather than leveraging solitude as an opportunity for self-determination (Dzando et al., 2025; van den Hoonaard, 2009). The varying ways participants perceived and coped with living alone, particularly in the context of significant life transitions, emphasize that pathways to maintaining well-being for older adults living alone are rooted in their personal histories.
Our findings imply that in future comparable crises, public health strategies should foster a balance between protection against infection and strategies to keep older adults living alone engaged in meaningful connections. Such strategies should leave room for the diversity in the needs of older adults living alone. For example, those accustomed to living alone may benefit more from programs that promote social engagement. In contrast, those still adjusting to living alone may need more emotional and instrumental support. Moreover, our study implies that older adults living alone may require extra support and encouragement to re-engage in out-of-home activities that enhance their well-being, as we found that a return to normalcy did not occur automatically after measures were lifted. Lastly, participants described their well-being as the result of lifelong learning. Although this study centered on the pandemic, it suggests that maintaining well-being requires more than short-term crisis measures. Our findings underscore the need for promoting well-being as a fundamental component of public health efforts, integrating programs and interventions that strengthen meaningful connections, foster social inclusion, and enhance individuals’ sense of control. Importantly, such public health approaches must be adaptable to meet the diverse needs of older adults living alone.
Our study possesses several strengths that enhance both its scientific rigor and practical relevance. First, the involvement of experienced qualitative researchers, along with the diverse backgrounds of our research team, enriched the analytical process and fostered a comprehensive, multi-perspective approach to data interpretation (Smith et al., 2022). Second, the use of IPA allowed us to capture both the unique and common experiences of participants as they navigated the challenges of maintaining their well-being during the pandemic. This approach facilitated the identification of diverse yet overlapping patterns in the data, providing deeper insights into the complex dynamics of their experiences.
This study merits several limitations that should be considered when interpreting the findings. First, our research provides a “snapshot” of the experiences of older adults at a specific point in time during the pandemic. This cross-sectional approach restricts our understanding of how their experiences and coping mechanisms may have evolved. However, we believe that the timing of the interviews offered participants a valuable opportunity to reflect on their experiences more meaningfully, having had time to process them (Smith et al., 2022). Another limitation is the potential for bias stemming from the sensitive nature of the topics discussed, such as loneliness and loss. To foster a safe environment for these discussions, we ensured confidentiality and privacy, employed empathetic and active listening techniques, and made it clear that participants could skip questions or end the interview at any time. We believe these strategies encouraged participants to share their thoughts and feelings openly, thereby mitigating potential biases in the data. Another limitation of our study is the homogeneity of the study sample, which may not have captured the full range of experiences across diverse demographic groups of older adults. However, in IPA, sample homogeneity is crucial for ensuring a focused exploration of lived experiences. This approach enables a deeper examination of shared experiences within a specific context, while still addressing individual nuances (Smith et al., 2022). As IPA prioritizes depth over generalizability, we considered a more homogeneous sample valuable for exploring the complexity of maintaining well-being during the COVID-19 pandemic among older adults living alone. Lastly, our different modes of interviewing (being face to face and via video calls) each had their potential limitations. While face-to-face interviews offer a more personal connection and the ability to observe non-verbal cues, video calls might limit non-verbal cues and privacy (Lobe et al., 2022). However, participants in both formats were equally engaged and provided detailed responses. Therefore, we believe the interview mode did not affect data richness or introduce adversities.
In conclusion, our study reveals how social distancing measures during the pandemic created a void between participants’ desire for meaningful connections and the limited opportunities available to meet these needs. Key aspects of maintaining well-being included staying connected, experiencing social inclusion, and regaining a sense of control. Additionally, participants’ life histories significantly shaped how they navigated the challenges of maintaining well-being. Overall, our results highlight great individual variability in how older adults living alone maintained their well-being during the pandemic. This advocates for interventions and support strategies that leave room for the unique needs of older adults living alone when opportunities for social engagement are limited.
Footnotes
Acknowledgments
We would like to thank the (social) care professionals that helped us to recruit participants for the study. Furthermore, we extend our sincere gratitude to all the participants who generously shared their time, experiences, and insights for this study. Lastly, we thank the native English speaker for their assistance and contributions in refining the translation of the quotes.
Author Contributions
D. Besselink designed the study, collected and analyzed the data, and drafted the manuscript. F. D. Schaap co-designed the study, collected data, and contributed to data analysis. F. van der Lucht assisted in study design and data analysis. S. J. Geelen and M. J. Sealy contributed to data analysis. H. Jager-Wittenaar and E. J. Finnema assisted in the study design and data analysis. All authors participated in drafting the manuscript and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed a receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Nationaal Regieorgaan Praktijkgericht Onderzoek SIA (SIA.COV.01.001).