
Abstract
While family resilience can diminish the risk of negative health outcomes among children in kinship care, less research examines if family resilience shapes positive indicators of development. Given previous studies have reported lower social-emotional competence and school engagement among children in relative care, additional research is needed to understand how kinship families support the flourishing and school engagement of their children. Using data from the 2017–2019 National Survey of Children’s Health, this study examines associations between family resilience and two positive indicators of developmental well-being, child flourishing and school engagement. Analyses showed family resilience was positively associated with child flourishing and school engagement. Findings suggest adapting family resilience interventions to the needs of kinship families may be an effective way of promoting the holistic well-being of children in kinship care.
Kinship care, defined as a caregiving arrangement in which a relative or family friend assumes the primary care of a child in the event of parental incapacity, remains a critical component of the U.S. surrogate parenting landscape. Approximately 2.6 million children in the United States are estimated to be raised in kinship care (Annie E. Casey Foundation, 2022), with most children living in informal kinship care arrangements that are unsupervised by the child welfare system (Berrick & Hernandez, 2016). Among children in foster care, approximately 35% live with a relative, reflecting over 50 years of policy that prioritizes placements with relatives to maintain children’s connections with family, culture, language, and community (Day et al., 2020; U.S. Department of Health and Human Services, 2022).
Despite its ubiquity, children in kinship care generally experience worse social-emotional and lower school engagement compared with children raised by their birth parents (Bramlett et al., 2017; Washington et al., 2021). Many scholars link these outcomes to the deleterious effects of trauma exposure stemming from parental loss or child maltreatment that lead to parental incapacity (Hernández & Berrick, 2019; Xu et al., 2023). The effects of trauma exposure may be further exacerbated by the marked material and psychosocial needs frequently reported by kinship families (Ehrle & Geen, 2002; Hong et al., 2011). In the absence of resources that address the combined effects of these stressors, children in kinship care may struggle to achieve developmental competence (Bethell et al., 2019; Salmela-Aro & Upadyaya, 2020).
Family resilience refers to the capacity for families to weather and grow through adverse circumstances by way of intra- and extra-familial processes that promote mutual support, problem-solving, and resource generation (Ungar, 2016; Walsh, 2016). Among birth parent-led families, family resilience has been linked to improved social-emotional functioning and school engagement among children (Bethell et al., 2019; Herbell et al., 2020; Uddin et al., 2021). Although prior research has linked family resilience to improved health and lower odds of behavioral problems among children living in kinship care (Gómez, 2021), scholars have yet to examine the extent to which family resilience is associated with positive indicators of developmental well-being that provide a more holistic understanding of the well-being of children in kinship care. To better understand the reach of the compensatory effects of family resilience in kinship care, this study uses data from the National Survey of Children’s Health (NSCH) to examine associations between family resilience and two developmental competencies—child flourishing and school engagement—among school-age children living in kinship care.
Literature Review
Child Flourishing and School Engagement
Although developmental competence can be operationalized in several ways, child flourishing and school engagement have lifelong implications for well-being. Child flourishing is defined as a child’s positive sense of self and ability to function well both socially and psychologically (Lippman et al., 2011; Moore & Lippman, 2005; Wolbert et al., 2021). Key traits of child flourishing include an interest in learning, perseverance to complete tasks, and age-appropriate social-emotional regulation (Kwong & Hayes, 2017). Flourishing is largely considered a positive indicator of subjective well-being and is thought to facilitate children’s academic and social-emotional learning (Bethell et al., 2019; Herbell et al., 2020). Previous research in nonkinship populations documents associations between child flourishing and other positive developmental outcomes across the life course, including reduced mental health and behavioral problems in childhood and fewer physical, mental, and social health problems in adulthood (Bethell et al., 2019; Jones et al., 2015; Kwong & Hayes, 2017; Linares et al., 2022; Lippman et al., 2011; Vergunst et al., 2019).
School engagement is conceptualized as a child’s general interest in and dedication to academic pursuits. Indicators of school engagement include homework completion, participation in school activities, and positive attachments with schools and teachers (Fredricks et al., 2004; Jimerson et al., 2003). School engagement also includes cognitive ability and a willingness to put forth effort to learn new skills (Fredricks et al., 2004; Jimerson et al., 2003). Among others, school engagement has emerged as a protective factor against school dropout and student boredom, and is associated with improved educational and employment outcomes in adulthood (Abbott-Chapman et al., 2014; Fredricks et al., 2005; Symonds et al., 2023).
Child Flourishing and School Engagement in Kinship Care
Few studies explicitly examine flourishing among children in kinship care. A related body of literature notes children in kinship care generally experience elevated mental health symptoms compared with those in the care of their birth parents (Bramlett et al., 2017; Lee et al., 2020). These suboptimal outcomes are posited to arise from the experiences of maltreatment, parent–child separation, and trauma that often precede kinship care arrangements (Hernández & Berrick, 2019; Xu et al., 2023). In many instances, these events undermine the opportunity for children to form secure attachments, explore their social environment, and learn how to self-regulate (Tarren-Sweeney, 2013; Xu & Bright, 2018; Xu et al., 2023). Altogether, evidence suggests children in kinship care may not experience the same level of flourishing as those who never experience out-of-home care.
Similarly, children in kinship care tend to have lower school engagement and academic achievement than children who have never experienced out-of-home care (Bramlett et al., 2017; Font, 2014; Nelson et al., 2010; Washington et al., 2021). While the reasons for lower school engagement and academic achievement among children in kinship care are not fully understood, prior research suggests childhood adversity, economic hardship, and lower caregiver educational attainment all contribute to lower school engagement in this population (Font, 2014; Robles et al., 2019; Washington et al., 2021). Given most children in kinship care are in informal care arrangements that go without the financial and service supports of the child welfare system, it is also possible kinship families may struggle to invest in their children’s academic pursuits in light of more pressing unmet needs (Bramlett et al., 2017; Washington et al., 2021).
Family Resilience
Family resilience refers to the capacity for families to navigate adversity by way of transactional intra- and extra-familial processes that promote mutual support, problem-solving, and the generation of instrumental and emotional resources (Ungar, 2016; Walsh, 2016). Walsh’s Family Resilience Model articulates nine processes organized into three broad categories: belief systems (processes that contribute to a unified understanding of stressors within the family unit), organizational processes (processes that reorganize family roles to accommodate new stressors impinging on family well-being), and problem-solving processes (strategies used to effectively communicate and resolve problems; Walsh, 2016). Over time, these processes result in improved understandings of the stressor, new routines, and resource acquisition that lead to a family’s bonadaptation (Patterson, 2002; Walsh, 2016).
An emerging literature suggests that family resilience is associated with fewer intergenerational health and mental health problems in kinship families and improved child welfare-related outcomes (Cavanaugh et al., 2020; Dolbin-MacNab et al., 2021; Gómez, 2021; Schneiderman et al., 2012). While the absence of negative health and child welfare outcomes is certainly an indicator of positive adaptation, understanding influence of kinship family resilience on child outcomes also requires assessment of positive indicators of development and well-being (Masten, 2018; Patterson, 2002). Scholars contend that at any given point in the life course, families face developmental tasks that play fundamental roles in their “successful accomplishment of the nurturance and socialization of the family” (Masten, 2018; Patterson, 2002; Walsh, 2016). Via adaptive resilience processes, it is thought families attain and distribute instrumental and emotional resources that simultaneously impede negative adaptation while promoting well-being (Masten, 2018; Patterson, 2002; Walsh, 2016). Therefore, examining family resilience processes that help kinship families accomplish developmental tasks, such as child flourishing and school engagement, provides an opportunity to (a) understand the reach of the compensatory effects of family resilience within contexts characterized by multiple forms of adversity, and (b) inform the development of kinship navigator and other services that promote the well-being of children in kinship care.
The Current Study
Using a sample of kinship families derived from the NSCH, this study tests whether family resilience is associated with child flourishing and school engagement, over and above the influence of common risk factors such as caregiver health and mental health problems, poverty, and child mental health problems. Based on our theoretical framework and past research, we hypothesize family resilience will be positively associated with both child flourishing and school engagement.
Method
Sample
This study analyzes data from the NSCH, an annual survey conducted by the U.S. Census Bureau to gather information about child and caregiver health from a representative, randomly selected sample of U.S. households with children ages 0 to 17 years (U.S. Census Bureau, 2020b). Caregivers responded to questions pertaining to their and the focal child’s health, mental health, family life, and sociodemographic characteristics (see U.S. Census Bureau, 2020b for survey methodology). Survey administrators selected a focal child in the household and the caregiver responded to child-level measures as they pertained to that child. Given the NSCH was not designed to collect data from kinship caregivers, data from 2017, 2018, and 2019 were combined to increase the sample size (U.S. Census Bureau, 2020a). The NSCH did not measure child welfare system involvement. Caregivers and their children were included in the current analytic sample if (a) the primary caregiver was a grandparent, aunt or uncle, other relative, or nonrelative; (b) the child’s secondary caregiver (if available) was also a grandparent, aunt or uncle, other relative, or nonrelative; (c) the household was led by the kinship (respondent) caregiver; (d) the child was of school age (ages 6–17); and (e) had complete data on study variables. Of the total 81,546 families in the data set, 2303 (2.8%) were led by a kinship caregiver and had a school-age focal child. Among these, 274 (11.9%) were missing data on one or more study variables and were excluded from the current sample.
The final analytic sample consists of 2029 children living in kinship care. Children in the current sample were 11.5 years old, on average, and evenly split by assigned sex (50.6% female; Table 1). Children were predominantly white (51.4%) or Black (34%), and approximately 16.6% were Latinx. Over 60% of families earned less than 200% of the federal poverty line. Children in the analytic sample were less likely to be described as some other race alone by their caregivers (relative risk ratio = .09, p < .001) and had lower odds of being Latinx compared with those excluded from the sample (OR = 0.45, p = .03). A greater proportion of kinship families in the sample earned between 200% and 399% of the federal poverty level (FPL; 25.2%, 95% CI = 20.7, 29.7) than those excluded from the sample (11.7%, 95% CI = 4.0, 19.3). These differences should be considered when interpreting results.
Sample Demographic Characteristics (N = 2029).
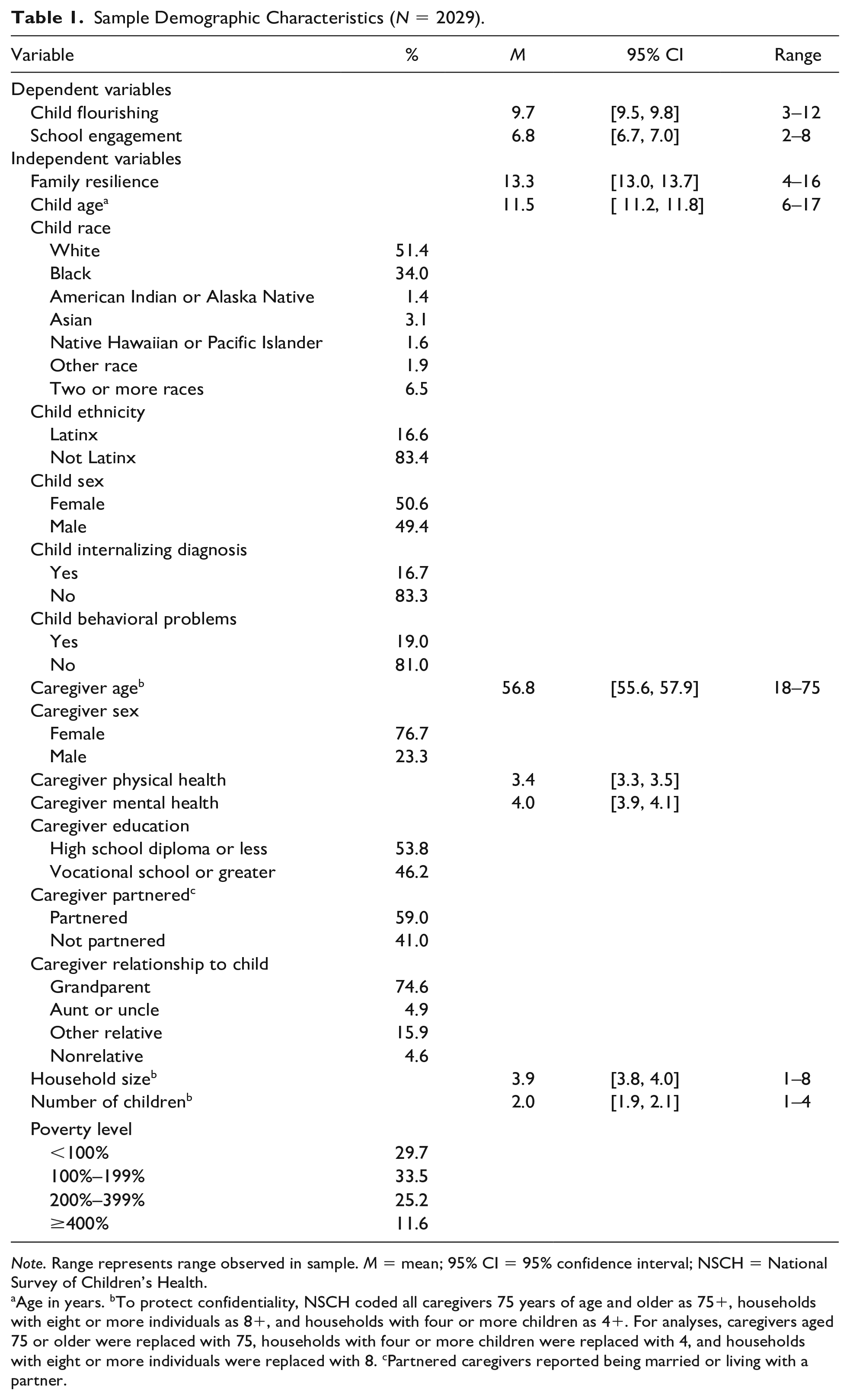
Note. Range represents range observed in sample. M = mean; 95% CI = 95% confidence interval; NSCH = National Survey of Children’s Health.
Age in years. bTo protect confidentiality, NSCH coded all caregivers 75 years of age and older as 75+, households with eight or more individuals as 8+, and households with four or more children as 4+. For analyses, caregivers aged 75 or older were replaced with 75, households with four or more children were replaced with 4, and households with eight or more individuals were replaced with 8. cPartnered caregivers reported being married or living with a partner.
Measures
Family Resilience
Kinship family resilience was measured using the NSCH’s family resilience scale (Child and Adolescent Health Measurement Initiative, 2019). This four-item composite measure assessed the frequency in which caregivers engage in intrafamilial processes of mutual support and problem-solving when confronted with challenges. Caregivers used a 4-point scale to indicate whether they engaged in each behavior (1) all of the time, (2) most of the time, (3) some of the time, or (4) none of the time. To facilitate interpretation, scores were reverse coded and summed so that higher scores indicated higher family resilience. Sample scores ranged from 4 to 16. Cronbach’s alpha for the family resilience scale was .90, indicating high internal reliability.
Child Flourishing
Child flourishing was measured using the NSCH’s child flourishing scale (Child and Adolescent Health Measurement Initiative, 2019). This three-item measure assessed children’s curiosity for learning new things, ability to finish self-initiated tasks, and ability to self-regulate when challenged. Caregivers responded on a 4-point scale from 1 (Always) to 4 (Never). To facilitate interpretation, scores were reverse coded and summed so that higher scores represented greater flourishing. Cronbach’s alpha was .76, indicating acceptable internal reliability.
School Engagement
School engagement was measured using the NSCH’s school engagement scale (Child and Adolescent Health Measurement Initiative, 2019). This two-item measure assessed how often children cared about doing well and did their homework. Caregivers responded on a 4-point scale from 1 (Always) to 4 (Never). To facilitate interpretation, scores were reverse coded and summed so that higher scores represented greater school engagement. Sample scores ranged from 2 to 8. Cronbach’s alpha was .84, indicating good internal reliability.
Covariates
We controlled for child-, caregiver-, and family-level covariates that previous research has linked to family resilience, child flourishing, or school engagement. Child-level covariates included age, race, ethnicity (Latinx/not Latinx), assigned sex (female/male), and diagnoses of internalizing (yes/no) and behavioral (yes/no) problems. While reported in the NSCH, we did not include adverse childhood experiences as a covariate given child internalizing and behavioral problems are well-established mediators that link childhood adversity to developmental outcomes later in childhood and adolescence (Robles et al., 2019). To confirm the risk of multicollinearity, we ran unadjusted logistic regressions which showed adverse childhood experience (ACE) scores were highly associated with both internalizing (OR = 1.60, p < .001) and behavioral (OR = 1.50, p < .001) problems. When included in adjusted models, ACE scores were not significantly associated with child flourishing or school engagement, and our results did not change.
Caregiver-level covariates included caregiver age, assigned sex (female/male), global physical health, global mental health, education level (greater than high school education or less), marital status (partnered/single), and relationship to the child (grandparent/other relative). Family-level covariates included household size, number of children, and income as a percentage of the federal poverty level. All covariates were included in both regression models (see section “Analytic Plan” for more information). To protect the confidentiality of respondents, the U.S. Census Bureau does not report caregiver race, ethnicity, or income in public use microdata. As recommended by the U.S. Census Bureau (2020a), income as a percentage of the federal poverty level was imputed using multiple imputation given the high level of missingness across the variables used to create this measure.
Analytic Plan
Analyses were conducted in Stata 17.0 (StataCorp, 2021). Prior to hypothesis testing, we ran a series of weighted linear, logistic, and multinomial regression models to compare the demographic characteristics of children in kinship care with those of children who were in the care of their birth parents. Considering past evidence that grandparents report greater family resilience and may have more parenting experience that might render positive outcomes (Gómez, 2021), we used weighted linear regression (Stata cannot render correlation coefficients using imputed data) to examine bivariate associations between caregiver relationship with the child and our main study variables (family resilience, school engagement, and child flourishing). To test our hypotheses, we fit two weighted multiple linear regression models to examine associations between family resilience and our dependent variables, child flourishing and school engagement, adjusting for the influence of all covariates listed in the “Measures” section. We used the subpop option to render accurate standard error estimates for the kinship sample. Because Stata does not provide an R² for models using imputed survey data, we standardized continuous variables to enable the interpretation of regression coefficients as effect sizes (i.e., standard deviations).
Results
Descriptive Statistics
Consistent with previous studies (Bramlett et al., 2017; Winokur et al., 2018), children in kinship care were significantly more likely to be diagnosed with internalizing (OR = 1.3, p = .004) and behavioral problems (OR = 2.3, p < .001) than those who were not in kinship care. A greater proportion of kinship families lived under the federal poverty line (FPL) compared with the general NSCH sample (29.7% vs. 17.3%) and fewer earned more than 400% of the FPL (11.6% vs. 33.4%). Although average child flourishing and school engagement scores were reasonably high among children in kinship care, they were significantly lower than the child flourishing (β = −0.27, p < .001) and school engagement (β = −0.23, p < .001) scores of children in the care of their birth parents.
Bivariate Associations With Relationship Type
Unadjusted linear regression models revealed relationship type was not significantly associated with family resilience or child flourishing. There was a marginally significant association between relation to the child and school engagement (β = 0.24, p = .05). Compared with the child raised by other relatives, children raised by their grandparents had school engagement scores that were 0.24 standard deviations higher.
Associations With Developmental Outcomes
Controlling for covariates, family resilience was positively associated with child flourishing (β = 0.15, p< .001; Table 2). For each standard deviation increase in family resilience, caregiver-reported child flourishing increased by 0.15 standard deviations.
Multiple Linear Regression Analyses for Associations Between Family Resilience, Child Flourishing, and School Engagement (N = 2029).
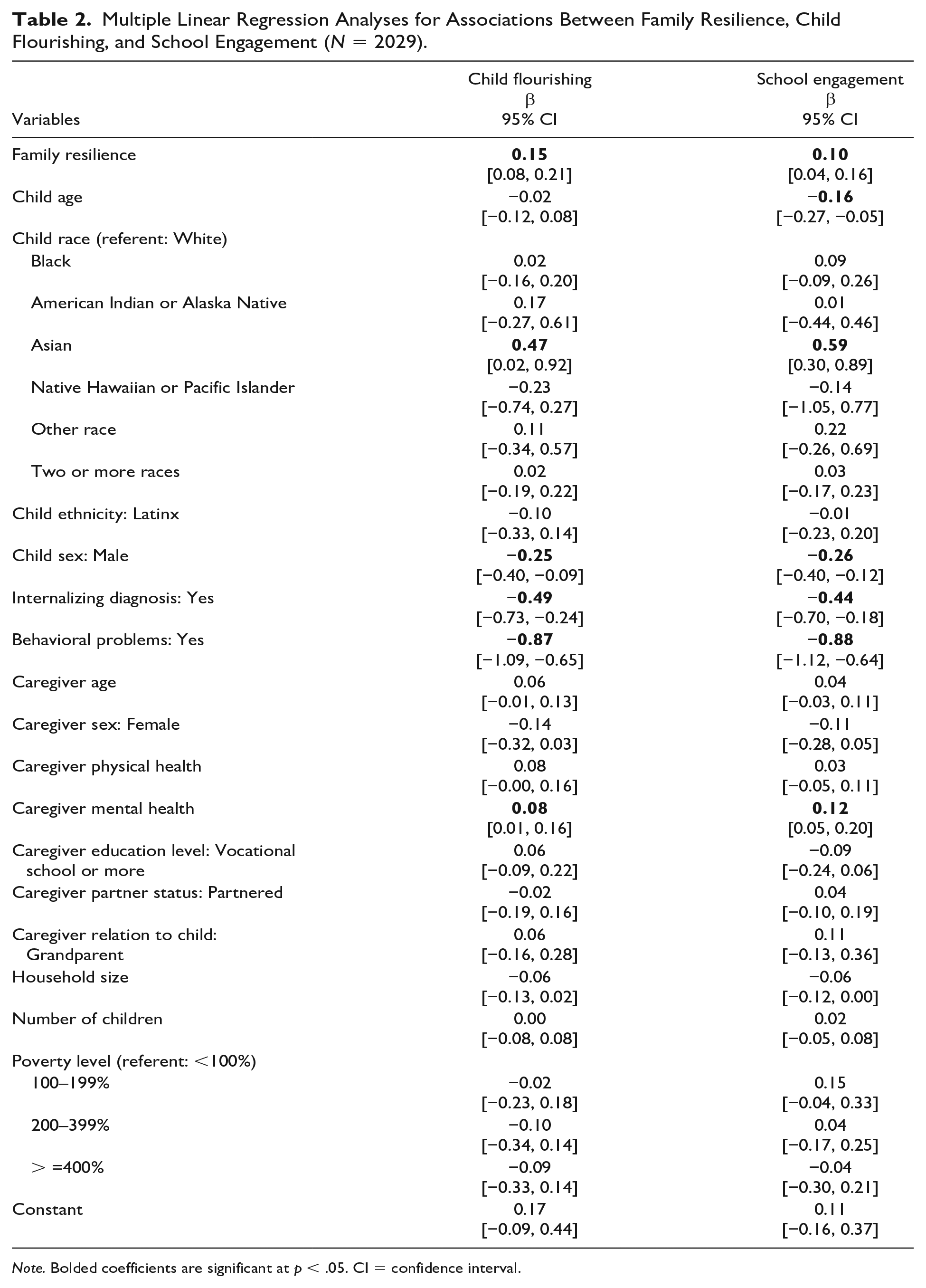
Note. Bolded coefficients are significant at p < .05. CI = confidence interval.
Net other variables, family resilience was also positively associated with caregiver-reported school engagement (β = 0.10, p = .002). For each standard deviation increase in family resilience, school engagement increased by 0.10 standard deviations.
Covariates
There were several significant associations between covariates and our outcomes. In the child flourishing model, being assigned male at birth was negatively associated with flourishing scores (β = −0.25, p = .002), as were child internalizing (β = −0.49, p < .001) and behavioral problems (β = −0.87, p < .001). Caregiver mental health (β = 0.08, p = .03) and Asian racial identity (β = 0.47, p = .04) were positively associated with child flourishing. In the school engagement model, child age (β = −0.16, p = .004) and being assigned male at birth (β = −0.26, p < .001) were negatively associated with school engagement. Once more, child internalizing (β = −0.44, p = .001) and behavioral problems (β = −0.88, p < .001) were negatively associated with school engagement. Asian racial identity was associated with higher school engagement scores (β = 0.59, p < .001). No other covariates were associated with our outcomes.
Discussion
Study findings suggest that, even in the presence of mental health problems and poverty, family resilience plays a compensatory role in promoting child flourishing and school engagement among children living in kinship care. These findings are consistent with previous studies reporting promotive relationships between family resilience and intergenerational health and mental health outcomes in kinship families (Cavanaugh et al., 2020; Gómez, 2021), and is the first to extend this line of inquiry to positive indicators of well-being among children in kinship care (Masten, 2018; Patterson, 2002). The reasons behind these main effects are not wholly understood. As it pertains to the current outcomes, there are likely mediating factors that connect family resilience to child flourishing and school engagement, such as positive parenting behaviors and school climate. Future research is needed to elucidate the role of these potential mechanisms and points of intervention.
Several covariates had stronger relationships with our outcomes than family resilience, reinforcing conceptual understandings of adaptation as a confluence of risk and protective factors (Masten, 2018; Ungar, 2016). Of particular note, internalizing and behavioral problems were strongly associated with child flourishing and school engagement, which underscores that even in the presence of adaptive family responses to crises, mental health challenges have far-reaching impacts on the well-being of children in kinship care (Bramlett et al., 2017). Nevertheless, mental health service access among informal kinship families is limited, which leaves the majority of children in kinship care without adequate mental health supports (Hong et al., 2011; Xu & Bright, 2018). As the child welfare field continues to invest in prevention, special attention should be paid to programs and policies that bring mental health resources to informal kinship families, whose efforts undeniably prevent entry into foster care.
Limitations
This study is not without limitations. We cannot infer causality from our cross-sectional analyses. Because kinship families are not the population of focus of the NSCH, we cannot assume that the current sample is representative of all kinship families in the United States. Similarly, the survey did not collect any information concerning past or present child welfare involvement among these families. Given formal kinship caregivers have access to greater financial and instrumental support compared with informal caregivers (Berrick & Hernandez, 2016; Lin, 2018), additional research is needed to understand how kinship family involvement in the child welfare system influences family resilience. Our study relies on self-reported data from caregivers, which may be prone to social desirability and common source biases. Future research may increase validity by incorporating data from children, teachers, and other caregivers. The current measure of family resilience is broad and does not prompt caregivers to report on their families’ responses to specific crises. Considering family resilience processes are context- and stressor-specific (Masten, 2018; Walsh, 2016), future research would benefit from more selective sampling criteria that examines adaptive responses to specific hardships (e.g., financial strain, parental substance abuse, child behavioral health concerns). We could not access information about the validation of the NSCH’s measures of family resilience, child flourishing, and school engagement. Nevertheless, the adequate internal reliability of these scales in the current sample along with the NSCH listing these items as composite measures of family resilience, child flourishing, and school engagement in their codebooks assuage validity concerns to some extent.
Implications for Practice, Policy, and Research
Limitations notwithstanding, our findings speak to the potential to intervene on family resilience to improve the well-being of children in kinship care. In addition to child-family team meetings that promote family-wide communication and planning around child welfare cases, there is potential to adapt existing family resilience interventions to the needs of kinship families. The FOCUS Family Resilience and Weaving Healthy Families Programs have shown promising effects in promoting positive parenting, social functioning, and intergenerational psychological well-being among military-involved and American Indian families, respectively (McKinley et al., 2023; Saltzman, 2016). Given both interventions are designed to be administered in community-based settings, they can be implemented within kinship navigator programs that are accessible to all kinship families, which may address the resource gap between formal and informal kinship families (Beltran & Epstein, 2013; Berrick & Hernandez, 2016). Moreover, the family-wide focus of these interventions may be especially appealing to Black, American Indian, and Latinx kinship families that often engage in collective caregiving (Barrio & Hughes, 2000; Sahota, 2019; Scannapieco & Jackson, 1996).
As it pertains to research, there remains a need to understand how existing services, including kinship navigator programs, promote family resilience, child flourishing, and school engagement. As of this writing, four kinship navigator programs have achieved the rating of “promising” or “supported” on the Title IV-E Prevention Services Clearinghouse (Title IV-E Prevention Services Clearinghouse, 2023). The extent of this evidence, however, revolves around child welfare outcomes such as time spent in out-of-home care, placement stability, and permanency. Given family resilience processes and indicators of child well-being likely play a role in shaping placement stability, permanency, and other child welfare outcomes, expanding the evaluation of evidence to these and other relevant outcomes (e.g., child and caregiver mental health, parenting stress) may advance efforts to (a) build the evidence base around practices that provide critical extra-familial support to kinship caregivers and their children, and (b) increase the number of reimbursable services under the Family First Prevention Services Act.
Conclusion
This study provides an initial examination of the relationships between family resilience and positive indicators of developmental well-being among children in kinship care. Although children in kinship care experienced greater mental health challenges and lower flourishing and school engagement scores than those in the care of their birth parents, our findings highlight family resilience as a potential lever that positively shapes developmental outcomes. While additional research is needed to understand the extent to which kinship family resilience can be feasibly bolstered by existing interventions and services, our findings provide a foundation for future research aiming to understand how child welfare and other service systems can better support the development and well-being of children in kinship care.
Footnotes
Disposition editors: Angelique Day and Cristina Mogro-Wilson
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.