
Abstract
Peer-to-Peer Kinship Navigation (P2PKN) employs someone with lived kinship caregiving experience in providing support to others experiencing similar challenges. This study examines if P2PKN improves concrete resource benefits application and enrollment and how it compares to other study groups (peer-to-peer plus innovations, formally trained kinship navigators, and usual child welfare services). Using data from the Children’s Home Network Kinship Navigator randomized control trial, this study compared the application and enrollment data for kinship caregivers in Temporary Assistance for Needy Family (TANF) Child Only Program for different types of kinship care program groups. Study findings revealed that P2PKN excelled at connecting caregivers to concrete resources and had significantly higher TANF application and enrollment rates than other groups.
Keywords
Background
Kinship Care
In 2018, an estimated 2.7 million children lived with kin caregivers, or grandparents, other relatives, or close family friends, because their parents were unable to care for them (The Annie E. Casey Foundation, 2019; U.S. Government Accountability Office [GAO], 2020). Moreover, 4% of all children in the United States (or 2,791,000 children in 2019) lived in households where a grandparent provides that child’s primary care. For kinship caregivers involved with the child welfare system, the type of resources and support they receive can vary based on the availability and accessibility of state resources, policies, and practice manuals that explicitly support placement with relatives and the values and principles of case workers. According to Generations United (2020), for every one child placed in formal kinship care with a relative by the child welfare system, there are 20 children living outside the child welfare system in informal living situations. Traditionally, kinship care has been dichotomized as either “formal” or within the child welfare system, or “informal” or not involved with the child welfare system. Over time, kinship care has emerged as a much more dynamic and complex concept due in part to reform and privatization efforts that have blurred this distinction through the implementation of the Families First Prevention Services Act, an increase in diversion placement into care without entry into the child welfare system (Gupta-Kagan, 2020), and as a reform strategy when public child welfare agencies contract with more private agencies to provide services. Kinship care in the current context is more nuanced and requires a closer examination of the lived experience to understand its concept (Littlewood et al., 2023).
Special attention is needed for kinship caregivers because they typically ask for and receive less support than other caregivers (Kondrat et al., 2015; Littlewood, 2014, 2015). The Annie E. Casey Foundation (2012) found that although kinship caregivers were eligible to apply and receive Temporary Assistance for Needy Family (TANF) Child Only grant, only 12% were receiving it nationwide. This was particularly concerning because TANF is tied to the child and not the caregiver or family income for eligibility, which allows for caregivers to enroll with less barriers. However, kinship caregivers continue to have difficulty obta-ining concrete resources for children in their care. Kinship caregivers often do not receive financial and supportive assistance available, including less than half receiving SNAP (42%) or Medicaid (42%) benefits and less than a quarter receiving child care (17%) and housing support (15%; The Annie E. Casey Foundation, 2012). 1 Another additional resource that has not been adequately utilized by grandparent caregivers, the National Family Caregiver Support Program (NFCSP) in Title III-E of the Older Americans Act, was designed to provide information about and assistance in accessing available services, organization of support groups, and respite care. According to the GAO (2020), although 51 total states are participating, less than half (23 states) spent 1% or more of their FY2016 funds (available through 2018) on older relative caregivers. 2
Although pockets of services and support exist in siloed child welfare and aging systems, these systems do not often work together to help the entire multigenerational, kinship family unit. The child welfare system is focused on the child’s safety, permanency, and well-being. The aging system is focused on providing support to the aging caregiver. To address this need for greater access to coordinated information regarding available resources for the entire kinship family, kinship navigator programs were developed and are currently being designed, implemented, or evaluated in mo-st states and jurisdictions. Kinship navigators connect kinship caregivers with available resources and support in the community, often helping navigate complex systems such as legal, education, child welfare, and others.
Kinship Navigator Programs
Kinship navigator programs offer information on benefits, services, supports, and programs to kinship caregivers (Cox, 2009; Kondrat et al., 2015; Littlewood, 2014, 2015; Littlewood et al., 2020, 2021; Lutes, Cummings, Littlewood, et al., 2018) and help families learn about and navigate systems of care relevant to their needs, such as legal, child welfare, school, aging, and others. Planning and operating in partnership with kinship caregivers has been a core value for kinship navigation programs and is included in recent federal guidance, Implementing Kinship Navigator Funding in Consolidated Appropriations Act (ACYF-CB-PI-21-05); this federal guidance (ACYF-CB-PL-21-05) was one of the only federal instruction provided to states and other jurisdictions to determine the program components for kinship navigation. Federal requirements for kinship navigator program reimbursement from FFPSA were not widely understood because only a few state FFPSA plans included kinship navigation. This current study seeks to connect the kinship navigation program components to the receipt of needed concrete resources for kinship families.
The kinship navigator context has changed from the first small projects in 2004 in Florida, Ohio, New Jersey, and New York to the first and second rounds of the first federal Fostering Connections Kinship Navigator demonstration projects awarded by the Children’s Bureau in 2009 and 2012, respectively. More recently in 2018 and each subsequent year, Title IV-B funding became available for states to apply to develop, implement, and/or evaluate kinship navigator programs. Some IV-B eligible jurisdictions spent funds that complimented existing local, county, or regional efforts in kinship navigation that include more case management/wraparound types of services (Florida, Delaware, and North Carolina). Other states, tribes, and territories have invested in larger statewide projects that are broader in scope with lighter service touches like information and referral or electronic resource provision (New York, Kansas, and California). Because federal child welfare investment has been the most available resource on a year-to-year basis for kinship navigator programs, most of these programs are situated within the child welfare system, which has a tendency to intimidate some caregivers and silo other programs and services. As more FFPSA plans begin implementation and jurisdictions focus on placing more children in out-of-home care with relatives, the current context for kinship navigation is fertile and dynamic. This current study provides important evidence to connect the kinship navigator program with the receipt of support that improves family well-being.
Kinship caregivers with lived experience can offer critical skills and support to aid kinship caregivers navigate systems of care and connect them to needed resources that promote safe and stable kinship placements. This can be called peer-to-peer kinship navigation (P2PKN), in which a kinship navigator program employs a kinship caregiver with lived experience to provide support to other kinship caregivers.
Peer-to-Peer Kinship Navigation
P2PKN is a type of kinship navigator service designed to provide nonclinical, strengths-based support, using kinship caregivers who are “experientially credentialed” by their own journey (as coined by Davidson et al., 1999). P2PKN can include titles such as peer specialists, peer coaches, peer advocates, or peer support specialists. P2PKN is informed by social learning theory, which explains how people learn from one another through observation, imitation, and modeling. Social learning theory can help explain how peers can be used to encourage desirable behaviors and to facilitate social changes such as helping kinship caregivers access concrete resources.
Integrating peer support into an existing kinship navigator program could provide an exciting opportunity for kinship caregivers involved in community-based programs. It also has the potential to uniquely improve outcomes for caregivers and families by relying on lived experiences. Within the last 25 years, programs including peer support have been found to provide the following benefits: (a) increased self-esteem and confidence (Davidson et al., 1999; Mead & McNeil, 2006; Salzer, 2002); (b) increased sense of control and ability to bring about changes in their lives (Davidson et al., 2012); (c) increased sense of hope and inspiration (Davidson et al., 2006; Ratzlaff et al., 2006); and (d) increased engagement in self-care and wellness (Davidson et al., 2012; Kurtz, 1990; Nelson et al., 2006; Ochocka et al., 2006; Trainor et al., 1997; Yanos et al., 2001).
There is published evidence to support the use of P2PKN as indicated by two kinship navigator demonstration projects. One such program used this approach pairing new relative caregivers (n = 74) with a full-time, paid kinship liaison who identified as a current or former relative caregiver (Denby, 2011). This study found that kinship liaisons are helpful to caregivers and revealed 27 support categories that caregivers found most useful, including: explanation of caregiver rights and responsibilities, referral/connection to community resources, foster care pre-licensing assistance, educational materials, explanation of permanency options, and information & referrals. These liaisons increased caregivers’ knowledge of accessing available services and understanding the permanency process (Denby, 2011).
The second program, from the Children’s Home Network, also provides evidence to support P2PKN service. Prior to 2012, peers worked as support group assistants and outreach coordinators for the organization. Once funded by a federal demonstration project (2012-2015), the Children’s Home Network implemented and tested Kinship Interdisciplinary Navigation Technologically-Advanced ModelTM (KIN TECH), which used a randomized control trial to test P2PKN as an innovation to a kinship system of care. KIN TECH found that this type of kinship navigation improved child safety and placement stability and family functioning (Littlewood et al., 2020, 2021; Pandey et al., 2018). This current study is based on lessons learned from previous research and evaluation work with peers who functioned as community health workers, peer support navigators, and kinship navigators.
More recently, Saeteurn et al. (2022) systematically studied the effectiveness of peer parenting programs in child welfare on case outcomes, specifically permanency, time in care, and re-entry postreunification. They found that all the peer parent programs that met their review criteria had a positive impact on reunification rates when compared with nonparticipants. Saeteurn and Colleagues (2022) suggested it is a promising intervention to help support parents and meet child welfare outcomes.
Although there are plenty of benefits to using a peer-to-peer support model, there is not a plethora of published evidence of the effectiveness of these models in the field of kinship navigation. Another program (other than Denby in 2011 & Littlewood et al., in 2020, 2021, 2022, & 2023, discussed earlier) that has peer-reviewed published information is Edgewood’s Center for Children and Families’ Kinship Support Network (KSN) model (Cohen & Cooper, 1999). The KSN model was developed in San Francisco, California, in response to kinship caregiver’s need for trusted community-based information and supports from other caregivers, outside of child welfare. Edgewood hired elderly African American and Latino grandparents from the communities where kinship caregivers lived. Lessons learned (Cohen & Cooper, 1999) from this model informed subsequent peer-navigator work with kinship caregivers, including a kinship navigation national demonstration project in California of four collaborative agencies with navigators having kinship lived experience. Currently in 2022, kinship navigator programs typically employ peer-to-peer kinship navigators, formally trained kinship navigators (social worker or human service-related degreed), and supervisors (degreed social workers providing clinical supervision to staff).
The Importance of Connecting Caregivers to Concrete Resources and Supports
In adverse childhood experiences (ACEs) research, there are five important protective factors proven to mitigate ACEs and contribute to establishing safe and emotionally stable homes; this framework helps to identify necessary strengths and supports for a family, with a focus on factors that protect families from abuse and neglect. One of the five protective factors includes concrete resources and supports, which refer to the direct provision of needed program services to a family including Medicaid expansion, supportive housing, child care, and food and nutrition assistance (i.e., SNAP and WIC programs). In addition to concrete support, economic supports are also helpful to families, such as minimum wage increases, earned income tax credits, child support, and sustained income support. Recent research on economic and concrete supports has shown their impact on child maltreatment rates and child protective service involvement (Anderson et al., 2021). Family income is strongly associated with child maltreatment and child welfare entry. Families living below the poverty line are more than 40 times more likely to enter child welfare than median income families (Raissian & Bullinger, 2017; Rostad et al., 2017). Connecting kinship families to concrete and economic support is an essential function of kinship navigation. Although these resources are so critical to the prevention of child maltreatment and child welfare entry, few studies have examined the ways in which P2PKN connect kinship families with these important resources and supports. Furthermore, the authors were unable to locate any studies which compared the effectiveness of P2PKN with formally trained kinship navigators (FTKNs). This information could play an important role in learning about kinship navigation program implementation.
Current Study
This current study is one of the first studies to use a randomized control trial to demonstrate how the kinship navigator program improves caregiver enrollment and/or receipt of concrete resources, as well as determine which type of kinship navigator is more effective in connecting both informal and formal caregivers to available resources: P2PKN or FTKN. This study will explore the group differences in TANF applications and enrollment specifically among those receiving peer navigation. There are two classifications of peer-to-peer: (a) the peer-to-peer kinship navigator-only model (P2PKN), which provides a peer to the kinship caregiver who has lived experience similar to the kinship caregiver and (b) the peer-to-peer kinship navigator plus model (P2PKN Plus), which provides the peer with lived experiences as well as additional program innovations, including support of an interdisciplinary team and a technological innovation component (see, Littlewood et al., 2020, 2021; Pandey et al., 2018). Specifically, this study will answer the research question: Did peer-to-peer kinship navigation increase the number of TANF benefits applications and enrollments compared with those receiving child welfare services as usual and those receiving services from a formally trained kinship navigator?
Method
Participants
The sample population included the kinship navigator program groups from the authors’ (Littlewood et al., 2020, 2021; Pandey et al., 2018) original project. For the purpose of this study, kinship navigation provides information, referral, and follow-up services to kin caregivers and links them to critical benefits and services. The intervention includes an intake phone session, weekly phone/in-person intervention for up to 12 weeks, and follow-up postintervention check-ins at 12, 24, and 36 months. In the original sample, 1,551 kinship caregivers were recruited from a community-based kinship navigator program in a large county in the Southeastern United States from 2012 to 2015 and randomly assigned to one of four groups: (a) P2PKN (n = 236; navigation assistance is provided by a person who has experience being a kinship caregiver); (b) P2PKN Plus (n = 255; peer-to-peer kinship navigation is provided with an interdisciplinary team for problem-solving and a shoulder-to-shoulder in-home approach for benefits application with a tablet or laptop); (c) FTKN (n = 858; kinship navigation is provided by trained professionals who don’t have lived experience as a kinship caregiver); and (d) usual care child welfare (n = 202; child welfare services are provided by the community-based child welfare provider in the county). Baseline equivalency was examined for the full sample. Chi squares were performed and found that marital status (χ2 = 38.99, p < .01, with usual care more likely to be single) and length of time caregiving (χ2 = 18.32, p < .05, with usual care more likely to care for children for less than 6 months) were statistically significant by kinship navigator program group indicating these two variables were not equivalent among groups. To address this issue, these two variables were controlled for and held constant. (See original study methods in Littlewood et al., 2020, 2021; Pandey et al., 2018).
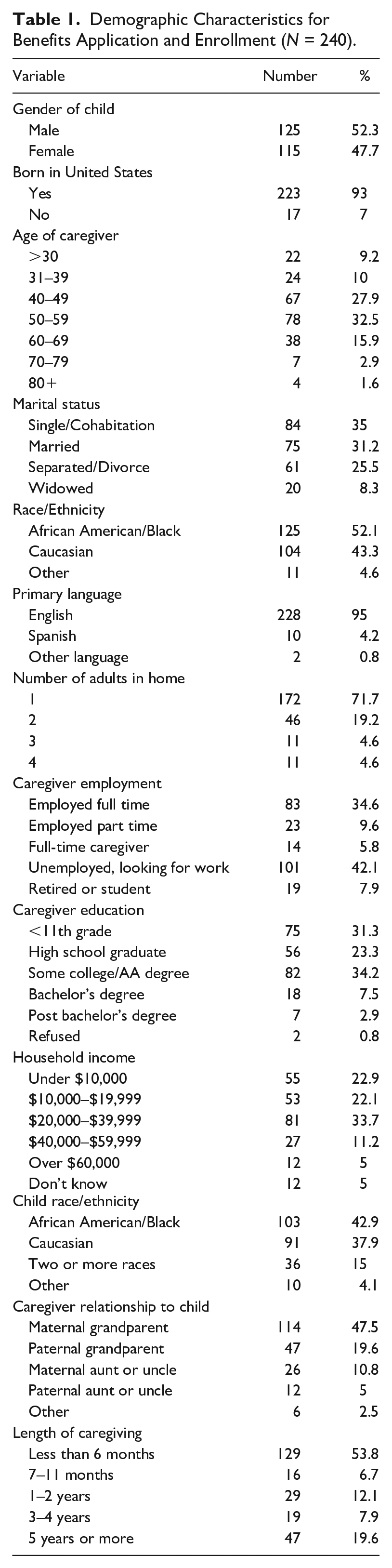
During the time that data agreements were agreed upon for the study between the program and the State Office Department of Children and Families, the TANF data and child welfare outcomes data were maintained by two separate departments and not integrated. In addition, there was concern from the State on the privacy and safety of the data in its current formation. Therefore, data retrieval went through a five-step process: (a) de-identified program data was randomly selected by aggregated group by the researcher; (b) this set was matched with child-level personal identifiable data; (c) the set was provided to a county program representative who managed the matching of TANF records from the State Office for Economic Self Sufficiency and the State Department of Children and Families; (d) this matched data was provided to the program and de-identified; and (e) the research team had program-level data, State financial self-sufficiency data, and State child welfare data for the purposes of testing the hypotheses of this study. Given the challenges regarding acquiring administrative data on TANF application and enrollment, a random sample of 60 kinship caregivers from each of the four groups was utilized for this current study, resulting in a sample size of 240. Selecting 60 caregivers per group would provide a powerful enough effect size to determine a medium effect. Demographic data were collected once the randomized dataset was selected and aggregated. Table 1 shows the distribution of aggregated demographic data. Most caregivers were between the ages of 50 and 59, 52% Black, 42% unemployed, 45% earning <$20,000 family income per year, and grandmothers caring for children less than 6 months. Marital status and length of time caregiving remained statistically significant in the study sample.
Demographic Characteristics for Benefits Application and Enrollment (N = 240).
Measures
The original data included pending court cases from one county; therefore, individual-level data were unavailable for the original sample and subsequently unavailable for the current sample. However, the data-sharing agreement did allow for the tracking of TANF applications and enrollment. Therefore, the current measures for this study include caregiver applications and enrollment in TANF Child Only at baseline, posttest (3–6 months), and follow-up at 12 months of program completion.
Data Analysis
Data were analyzed based on the administrative data coded when kinship caregivers applied and enrolled in TANF Child Only benefits. Descriptive and bivariate tests were performed to determine how the four different kinship navigator groups helped kinship caregivers apply and enroll in benefits. At baseline, no children were receiving TANF Child Only. The follow-up data were used for the current analyses to calculate the average application and enrollment rates (# participants applied/enrolled divided by total number of participants in the group). This allowed enough time for administrative processing of applications and enrollment forms. Analyses of variance (ANOVAs) were performed to compare the average application and enrollment rates for each group. Post hoc tests were performed to compare the means between groups.
Results
Figure 1 shows the average application and enrollment rates for TANF Child Only Benefits at follow-up. This demonstrates that by 12 months after program completion, the kinship navigator group with the highest percentage of applications and enrollments was P2PKN. Usual care child welfare services had the lowest percentage of applications and enrollments completed at 12 months. As indicated by the figure, the P2PKN group had the largest percentage of participants who applied for (72%) and enrolled in (52%) benefits. The next highest percentage of applications and enrollments was in the FTKN group, which saw a little more than 50% of participants applying for benefits yet only 39% enrolling in benefits. The P2PKN Plus group, which added the interdisciplinary team and technological innovation component, had the lowest application (27%) and enrollment (13%) percentages of the kinship navigator program groups. These percentages were similar to the usual care group, with no kinship navigator intervention, which had application <20% (n = 11) and enrollment <10%.
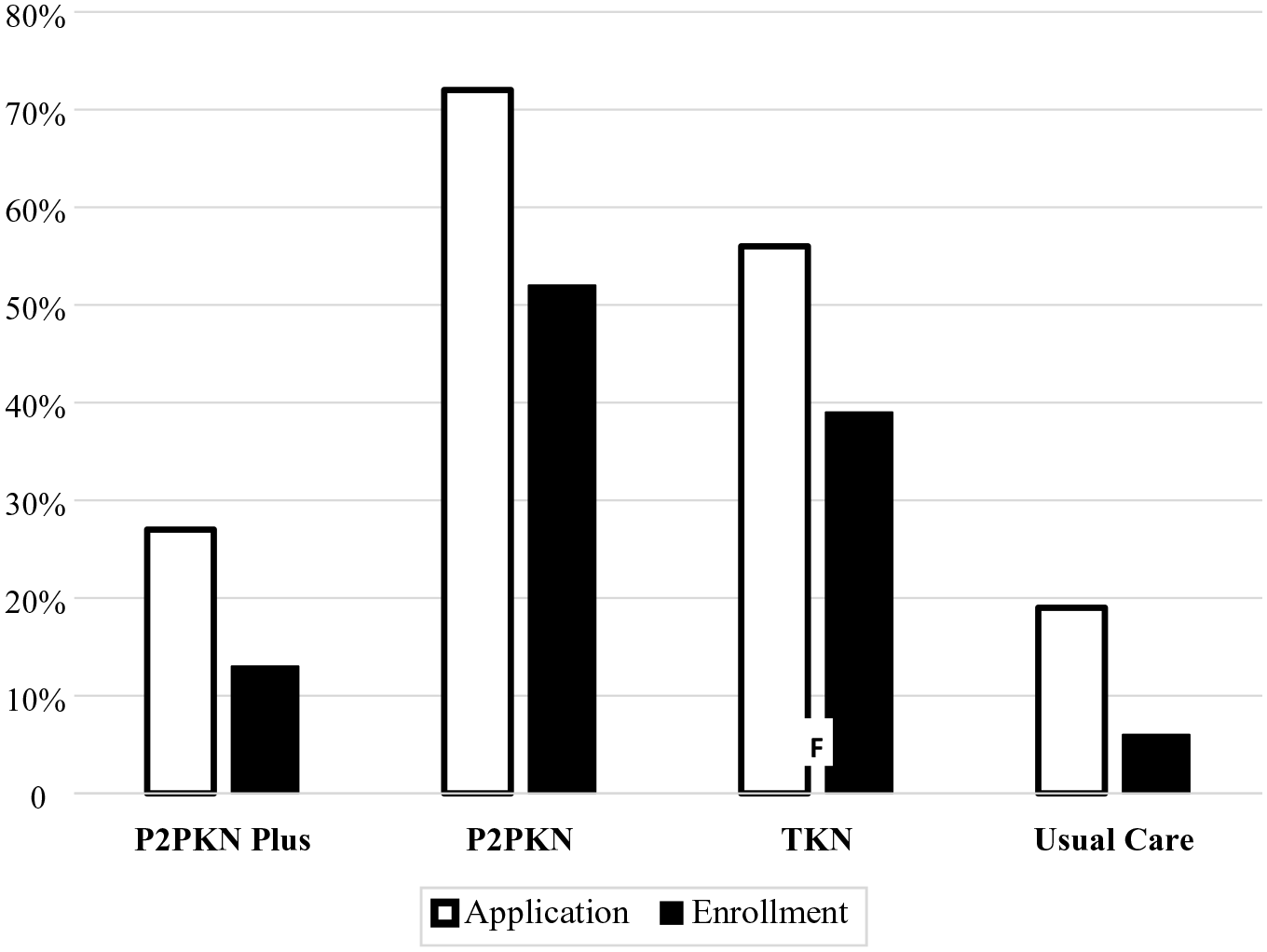
Percentages of participants in TANF Child Only application and enrollment (N = 240).
Using a one-way ANOVA, the different kinship navigator groups were compared on application and enrollment of TANF Child Only benefits. An ANOVA showed that the effect of kinship navigator group on the application was significant, F (3, 236) = 21.54, p < .001, as was the effect on enrollment, F (3, 236) = 15.83, p < .001. Table 2 shows rates for application and enrollment for each kinship navigator group.
A One-Way ANOVA.
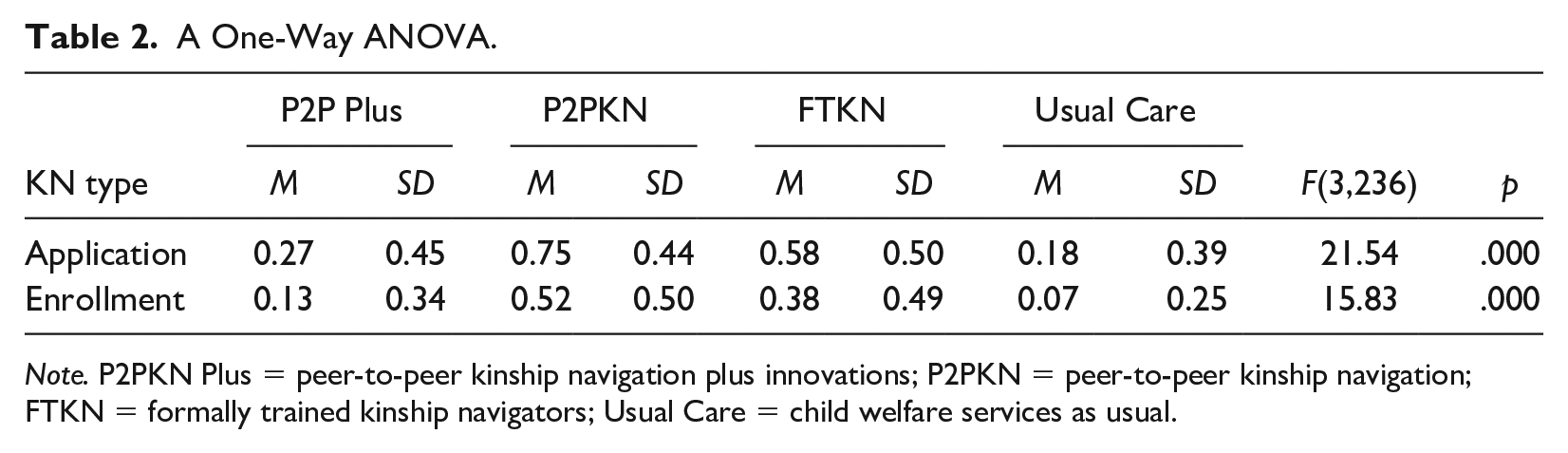
Note. P2PKN Plus = peer-to-peer kinship navigation plus innovations; P2PKN = peer-to-peer kinship navigation; FTKN = formally trained kinship navigators; Usual Care = child welfare services as usual.
Tests of the four a priori hypotheses of differences in application and enrollment for every four groups were conducted using Bonferroni-adjusted alpha levels of .0083 per test (.05/6). Results of the post hoc with Bonferroni adjustment indicated that application rate and enrollment rate were significantly lower in the usual care child welfare group (M = 0.08, SD = 0.08 and M = 0.06, SD = 0.07) than were those in both the P2PKN (M = 0.57, SD = 0.08, F[3, 57] = 8.90, p < .001 and M = 0.45, SD = 0.08, F[3, 57] = 8.90, p < .001) and in the FTKN (M = 0.40, SD = 0.08, F[3, 57] = 10.22, p < .001 and M = 0.32, SD = 0.08, F[3, 57] = 10.22, p = .000) groups. The pairwise comparison for both application and enrollment of the usual care with the P2PKN Plus were non-significant.
Discussion
Benefits Outcomes for the P2PKN Model
Usual care had the lowest application rate (19%, n = 11) and enrollment rate (6%, n = 4); the enrollment rate is below the benchmark (12%) in the United States (The Annie E. Casey Foundation, 2012). This could be influenced by high caseloads, turnover rates, and burden for child welfare workers as noted by Salloum et al. (2015). If workers are addressing crises, it can be difficult to take the time and help with application and enrollment for programs, especially if those individuals are not dedicated to kinship caregivers only.
The caregivers in the P2PKN group, however, had the highest rates of application and enrollment in TANF Child Only grants. The P2PKN group utilizes peers as navigators who may be more sensitive to the financial hardships that come with caregiving. They may use this empathy to advocate and champion others who have gone through similar experiences. In reviewing the implementation results, the differences could also stem from the workload attributed to peers compared with formally trained navigators. Peer navigators spent less time on paperwork and more time on the family support plan compared with FTKNs, which could contribute to the differences. More research is necessary to connect the type of kinship navigator to specific kinship caregiver outcomes.
Finally, given that kinship caregivers typically do better with one-on-one assistance with technology (Strozier et al., 2004), it was surprising that the P2PKN Plus group did not excel in applications and enrollments. In fact, according to the results this group did not significantly differ from the usual care group and had far fewer caregivers apply for and enroll in TANF Child Only, even when they were the only group to bring a Wi-Fi enabled laptop into the home of a kinship caregiver to work shoulder to shoulder with them to complete applications and other forms. When Littlewood et al. (2023) detailed the implementation of this program, they found that peer navigators were less likely than traditionally trained kinship navigators to perform a variety of tasks. They were more comfortable focusing on concrete resources and less likely to perform more specialized tasks, such as professional referrals and evaluation/assessment-type activities. These differences could possibly explain why peer navigators who worked in the plus model had lower application and enrollment rates than the peer navigators in the P2PKN-only model; peers in the P2PNK-only model were allowed to perform less tasks. This could potentially allow them more time to discuss and engage with caregivers on application and enrollment. In addition, in reviewing the results of the implementation study, it was noted that neither the FTKNs nor the P2PKNs engaged in the One-e-App, the Web-based portal designed to assist navigators in working with kinship caregivers or the interdisciplinary team. Future research could explore what specific technological interventions provide the most support to kinship caregivers.
Limitations
This study reports several limitations. First, a threat to the internal validity of this study is identified because we did not have access to personally identifiable information for the children returning to care because they were active cases and had open court records. Because of practical and ethical issues, it is very difficult to determine different patterns of care by demographics, which would have been performed if we had access to this information. As a result, children in this study who had different patterns of care could have been systematically different, which could have accounted for some or all of the results. Another threat to the internal validity of the study is that we were unable to precisely capture the length of stay or dosage. Patterns of movement through the different programs and length of stay could have been highly correlated. As such, we cannot rule out the possibility that the differences observed were simply related to longer lengths of stay, rather than due to the intervention received. Although random assignment was used, there is still concern that this study was unable to examine potential differences in groups at baseline, including placement histories, number of siblings placed together, and special needs of the children placed—all of which could have a significant impact on outcomes of interest. This information was not made available to the authors and presents a limitation to the application of these findings. Despite the limitations, this study presents some of the first results to compare P2PKN and FTKN programs for connecting kinship families to concrete resources.
Conclusion
The results of this study highlight the important considerations regarding how well P2PKN connects kinship caregivers to community resources and supports compared with formally trained navigators. This study promotes the importance of using peer navigators to help connect kinship families with concrete support, which has been a focus of timely programmatic and engagement strategies for leveraging economic support to promote child and family well-being and prevent maltreatment (Weiner et al., 2021). This study provides initial evidence suggesting that peer navigators are a good investment for child welfare to promote lived experience and connect kinship caregivers to needed support and resources, specifically financial assistance. It is also worth noting that P2PKNs are a highly successful workforce resource for connecting kinship caregivers to TANF Child Only applications and enrolling caregivers in the-se benefits. Prior to this study, the national average of kinship enrollment in TANF Child Only grants was 12%, while at follow-up for this study’s P2PKN program, more than half of caregivers were enrolled. This finding suggests that P2PKNs are useful for kinship caregivers who struggle to connect to benefits. Given these promising results, future studies could qualitatively explore the barriers and facilitators that exist for P2PKN implementation and also look at the role of technology in assisting in application and enrollment. This could aid in the improvement of existing P2PKN implementation, as well as provide information about the feasibility of implementation for organizations considering a new P2PKN program.
Recommendations for Practice
Given the importance of peer navigators for kinship navigator programs, there are some considerations that could help inform future practice with kinship families. As the child welfare system has been challenged with retaining a skilled workforce (Sedivy et al., 2020), adding P2PKN to their practice could provide an effective supplement or alternative to child welfare organizations that are working hard to promote kin-first placements. Employing P2PKN could potentially lighten the caseload for case managers who may be too overburdened to spend the time necessary with kin families to understand the nuances of enrollment requirements. Furthermore, implementing P2PKN programs could help to support the U.S. DHHS Administration for Children and Families (2022) strategic goal to use whole-family, community-based strategies to increase financial stability and economic mobility. According to the Capacity Building Center for States (2022), working in partnership with youth and families to center their lived expertise throughout planning and implementation can help agencies capitalize on the potential of the Family First Prevention Services Act and move further upstream toward primary prevention. Finally, providing opportunities for peers to work alongside formally trained kinship navigators and organizational staff, including leadership, can help the entire workforce learn how to better support kin families and connect them to needed community resources and supports.
Footnotes
Disposition editors: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Juvenile Welfare Board of Pinellas County, Children’s Board of Hillsborough County, U.S. Department of Health and Human Services. Children’s Bureau.