
Abstract
Kinship care is the increasingly preferred child placement with a relative when the biological parents are unable to provide care. Program and resource supports must understand how to best meet these caregivers’ needs. Through thematic analysis of existing literature, this study aims to understand how kin caregiver characteristics affect kinship care outcomes. A total of 28 peer-reviewed articles were included in this analysis. Findings indicate that caregiver characteristics, including racial differences, family roles, economic burden, structural supports, and caregiver health, have potentially differential impacts on kinship care and outcomes. Identifying influential caregiver characteristics highlights the importance of adapting policy, programming, and research to support diverse kinship families, rather than viewing them as homogeneous. Incorporation of these characteristic considerations may lead to more effective and impactful supports and improved well-being for all kinship families.
Keywords
More than 2.5 million children in the United States were living in kinship care between 2020 and 2022 (The Annie E. Casey Foundation, 2022). Kinship care occurs in homes where a relative, tribe member or fictive kin is the primary caregiver for a relative’s child (The Annie E. Casey Foundation, 2012). This could be formal care—initiated by the Child and Family Services (CFS) division in the state—or informal care, where the kin caregiver steps into the protective caregiving role without government intervention (Strozier & Krisman, 2007). Kinship caregiving may occur after a report of child abuse or neglect, teenage pregnancy, caregiver substance misuse, incarceration or death of a parent, family crisis, or a parent is unable to care for a child (Xu, Jedwab, et al., 2022). When a child is at risk of home removal, a family caregiver is the preferred placement option (Wheeler & Vollet, 2017).
Kin placement is preferred because of maintained familial bonds and preservation of community networks for the child which may promote positive outcomes (The Annie E. Casey Foundation, 2012). The federal government has begun to systematically provide supports to these kin caregivers through providing funding for Kinship Navigator Programs (KNPs). The Family First Prevention Services Act (FFPSA) of 2018 was federal legislation designed to support states at increasing child safety, well-being and permanency, caregiver well-being, access to services, referral to needed services, and family fulfillment with program outcomes (Wilson et al., 2019).
Research notes kin caregivers often have safer and more secure placements. As documented by Wheeler and Vollet (2017), children in kinship care were less likely than children in a non-relative foster care comparison group to experience abuse or neglect after discharge from placement. Gomez (2021) found, with predominantly older grandmother caregivers, that family resilience led to better child health and caregivers’ physical and mental health. One component of this funding was to sustainably support social service programs aimed to help kin caregivers, by identifying unique needs and proffering probable solutions (Pandey et al., 2019; Rushovich et al., 2017). KNPs were initiated or revised in many states as a part of the FFPSA as a support to kin caregivers. These programs had limited research-based evaluation of impacts though, so FFPSA stipulated services need to have evidence rated by the Title IV-E Prevention Services Clearinghouse (Wilson et al., 2019).
These KNPs must prove successful outcomes in areas including child safety, child permanency, child well-being, and adult well-being. Successful outcomes may be measured in a variety of ways but are broadly defined as follows. Positive child safety outcome indicates the absence of potential or actual threat of danger to the child within the home. Child permanency denotes stability in the home and maintenance of familial relationships. Favorable discharge and permanency outcomes may include a return to birth parent or custody to kin (Wheeler & Vollet, 2017). Child well-being is a multidimensional outcome comprising physical and mental health, social and behavioral skills, emotional functioning, cognitive abilities, and educational progress. Adult well-being for caregivers is all-encompassing and includes physical, mental, and emotional health, parenting practices, economic and housing stability, and family functioning (Wilson et al., 2019). Evaluation guidelines do not encourage the consideration of how these different outcomes may be affected or practically differ by caregiver characteristics.
Research has long asserted the need for understanding how multiple levels within the ecological framework—individual characteristics, caregiver–child attachment, kin family interrelationships, cultural influences, and societal and policy impact—may influence kin child outcomes (Hong et al., 2011). Belsky’s social-contextual model of determinants of parenting suggests that parenting is shaped by historical developmental experiences, social factors, and especially by individual attributes of caregiver and child (Belsky & Jaffee, 2015, p. 42). Specifically, Belsky and Jaffee (2015, p. 42) point out interrelationships between caregiver co-parent relationships, mental health, gender, and neighborhood and child development outcomes. These theoretical complexities are being explored and confirmed in research with ever-increasing diversity of characteristics included, but challenges persist in understanding how these theoretical influences affect kinship child and caregiver outcomes. The role of varying kin characteristic factors is particularly important to understand and incorporate into kinship supports to maximize outcomes for all.
Research has already indicated that demographics are a prominent external factor to consider within kinship care programming because kin caregivers are not a homogeneous community (Zinn, 2017). Studies have also indicated that some demographic subgroups are more likely to take part in kinship care (The Annie E. Casey Foundation, 2012). Kinship caregivers are more likely to be of low socioeconomic status (SES), older, less educated, and unemployed compared with families in which at least one parent lives in the home (The Annie E. Casey Foundation, 2012; Geen, 2004). Kinship caregiver demographics have also been demonstrated to vary by custodial arrangements (Strozier & Krisman, 2007). Yet, a systematic review by Lin (2014) found that many interventions were not designed to serve a specific population or with cultural sensitivity.
While data specifically focusing on kin caregiver characteristics is relatively limited to what is presented in this review, we can look to influential trends in broader family data. A systematic review including U.S. studies that explored custodial grandparents found they largely focus exploring immigrant and minority communities, but often in more urban locations (Sadruddin et al., 2019). This review also found that when coming from these urban and economically disadvantaged locations, grandparent caregivers often lack the same parenting resources and are often associated with poorer child physical health outcomes compared with parent caregivers (Sadruddin et al., 2019). Research has also found that a caregiver’s SES, including household income and education status, is a moderating variable between parenting interaction and child outcomes such as academic achievement. Alternatively, parental expectations of achievement are positively associated with child outcomes regardless of race, ethnicity, or SES (Boonk et al., 2018). With recent social disruptions including finances, at-home caregiving burden, isolation, and stress from COVID-19, researchers are identifying the important protective role that family processes might have on family members’ well-being (Prime et al., 2020).
The complex relationships between external factors and kinship family outcomes are theorized, but there exists limited research regarding full consideration of these impacts or their implications for kinship care support programming. By understanding what kinship caregiver characteristics current literature has found to be significant in association with outcomes, kinship program support, policies, and research can begin to tailor development to meet diverse needs. Consequently, this thematic analysis of literature aims to understand how kin caregiver characteristics affect kinship care outcomes.
Method
Selection Strategy
For articles search, the Web of Science database was selected because of its wide acceptance as a major comprehensive data source for social sciences and humanities (Birkle et al., 2020). Search terms included kinship, navigator, programs, caregivers, outcomes, and kinship family characteristics. Appropriate Boolean operators were included in programming search terms to help get a breadth of articles. These terms could appear in titles, abstracts, or papers and only peer-reviewed articles limited to the past 20 years (January 2002 to December 2022). The primary researcher reviewed titles and abstracts, and then ultimately the full article for relevancy to ensure findings explored kin characteristics. Of all articles appearing from this search (n = 66), a mix of qualitative and quantitative peer-reviewed articles (n = 28) were included in NVivo for analysis. Articles not relevant to the research question (n = 38) were excluded from the thematic analysis and reviewed for background and discussion connections.
Thematic Analysis
This review intends to evaluate the research and data specific to formal and informal kinship families and kin caregiving outcomes. Thematic analysis is a qualitative approach used to recognize patterns and interconnectedness in observable phenomena which can be used to evaluate current data and literature on various social issues (Boyatzis, 1998). To further explore the relationship of socio-ecological factors influencing kin outcomes, researchers conducted thematic analysis of literature as described by Joffe and Yardley (2003). Researchers examined findings of selected articles for manifest content codes of caregiver characteristics. These were theoretically driven; codes were deduced aligning with factors in the socio-ecological theory to determine the extent to which these factors are explored and impactful in current literature findings.
Articles were initially read to build understanding, and the results section of each article was examined for kin caregivers and family demographics. At the outset, factors were just related to the caregivers’ demographics, including age, race/ethnicity, gender, and SES, but researchers subsequently discussed and added codes related to caregiver health and external support experiences from caregivers as a related socio-ecological theory influence. Codes were assigned to segments of texts within the findings and discussion section. Multiple codes could be assigned if scope of findings crossed multiple characteristics. Researchers then examined coded text for latent level themes. Further inductive categorization from these codes led researchers to split categories into defined themes (see Appendix). The lead researcher reviewed and coded all articles, while co-authors independently reviewed random subsets of articles for reliability. Consensus themes and subthemes were co-developed including examples and counter examples to illuminate conceptual interaction in the socio-ecological model.
Findings
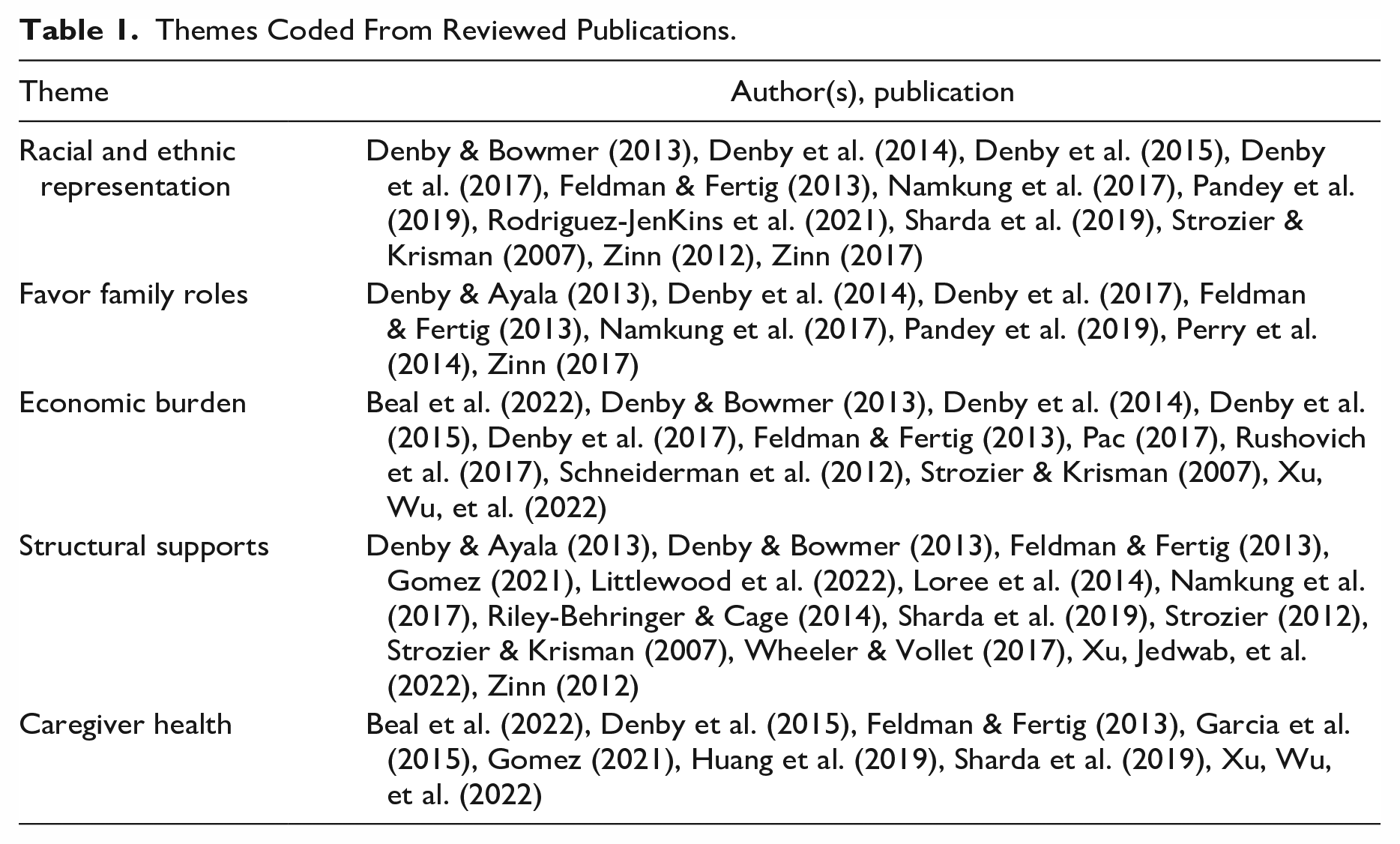
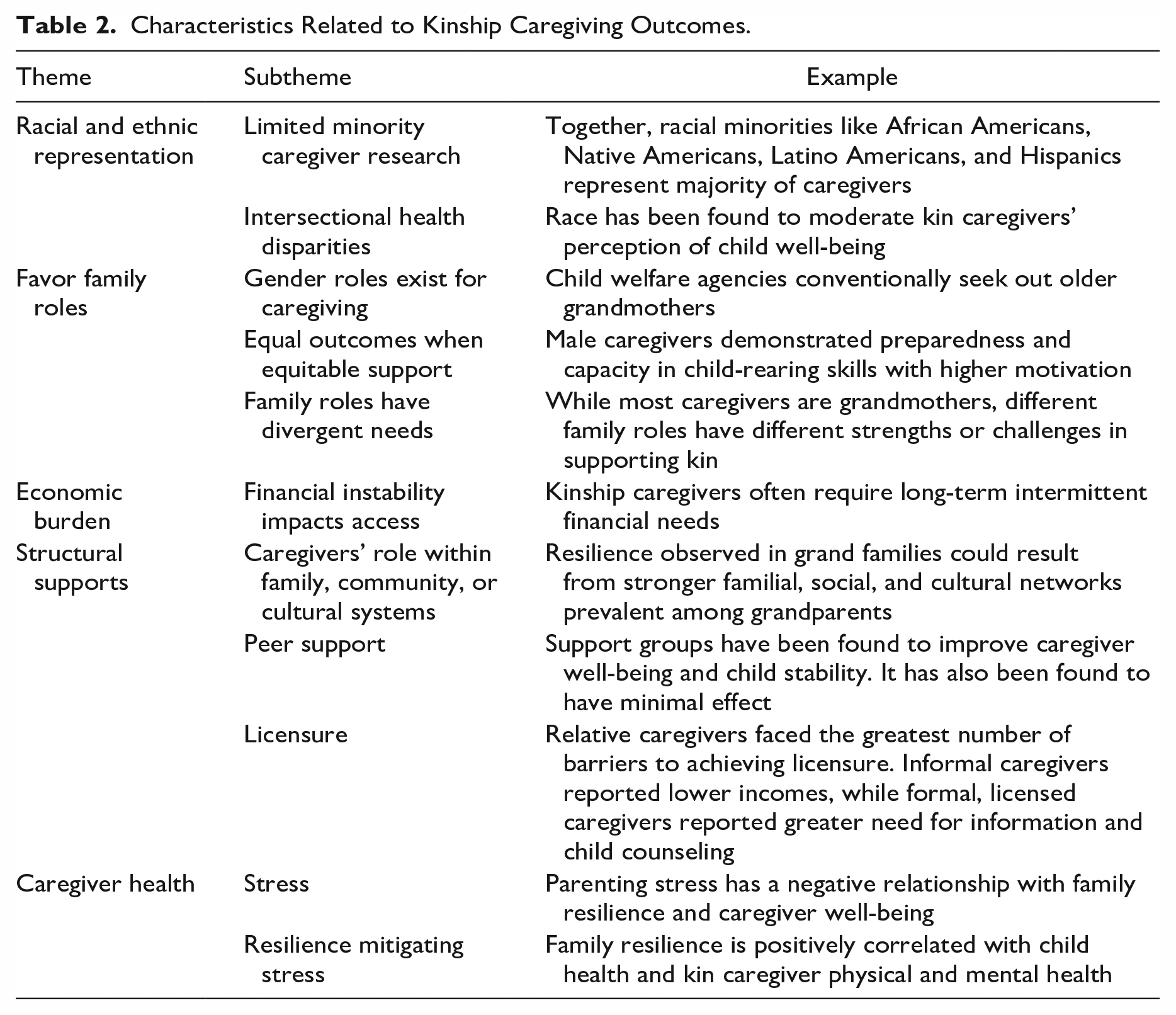
Caregiver characteristics have been explored across numerous kinship research studies. Outlined below are five themes exemplifying kinship caregiver characteristics potentially affecting child and family outcomes, including (a) racial and ethnic representation, (b) favoring family roles, (c) impacts of economic burden, (d) role of structural supports, and (e) caregiver health impacts on child well-being. Articles from which themes were generated are listed in Table 1, and subthemes with examples are identified in Table 2 within each theme description.
Themes Coded From Reviewed Publications.
Characteristics Related to Kinship Caregiving Outcomes.
Racial and Ethnic Representation
Limited Minority Caregiver Research
Racial minorities such as African Americans, Native Americans, Latino Americans, and Hispanics represent a majority of caregivers (Denby et al., 2014). There is also an overrepresentation of minorities among kinship foster youth (Zinn, 2017). Research has not always recognized how these demographics might affect caregiving; several studies have explored a majority of African American caregivers followed by white caregivers (Denby et al., 2017; Feldman & Fertig, 2013; Zinn, 2012), whereas many others had a higher prevalence of white caregivers (Pandey et al., 2019; Sharda et al., 2019; Strozier & Krisman, 2007).
Intersectional Health Disparities
The influence of culture and ethnicity on perception of child well-being was documented by Denby et al. (2015): European American kinship caregivers reported greater child well-being than did African American and Latino American caregivers. However, there were similarities in stress and strain levels, parenting capacity, and willingness to foster among African American, Latino American, European American, Asian American, and Native American caregivers (Denby et al., 2015). Compared to minority groups, Namkung et al. (2017) found that among sibling caregivers, caregiving took a higher toll on non-Hispanic white caregivers. Possible explanations for these differences include cultural norms and higher marriage rates observed among non-Hispanic white caregivers. This often results in additional responsibilities.
Favor Family Roles
Gender Preferences Exist
Caregivers often identify as female (Denby et al., 2017; Feldman & Fertig, 2013; Namkung et al., 2017; Pandey et al., 2019), which leads to child welfare agencies conventionally seeking out grandmothers for child placement. This practice is questioned by Denby et al. (2014) who found that male caregivers (brother, uncle, grandfather) have a high level of caregiving capabilities and low stress levels. Regardless of caregiver gender, greater placement stability of kin children was observed in maternal families compared to paternal kin needs (Perry et al., 2014).
Caregiving Ability May Not Be Gendered
Although there were no gender differences in caregivers’ stress levels, differences observed between male and female kin caregivers result from sociodemographic variance (Denby et al., 2014). Male caregivers demonstrated preparedness and capacity in child-rearing skills with higher motivation factors leading to a stronger involvement in the kin child’s upbringing (Denby et al., 2014). Male caregivers encountered frustration seeking out community resources just like female caregivers. Isolation and lower levels of social and familial connections is a challenge faced by male caregivers (Denby et al., 2014).
Family Role
Caregivers are often older and identified as grandmothers, but caregivers have divergent experiences based on their family roles. Aunt and uncle kin caregivers often provided kin youth with educational support when compared with other relative caregivers (Zinn, 2017). Grandparents are able to draw from previous parenting experience, but it often occurred in a different social environment the second time around due to more current parenting practices (Pandey et al., 2019; Zinn, 2017).
Sibling caregiving roles have been found to be motivated mostly by protective instincts and perceived threat of negative experiences in child welfare system (Denby & Ayala, 2013). Higher levels of perceived parenting capabilities were positively correlated with likelihood to adopt and kin children with special needs were also found to be more likely to be adopted by sibling (Denby & Ayala, 2013).
Economic Burden
Finances Related to Resource Access
Kinship caregivers often report high levels of unemployment and low income (Denby et al., 2014; Feldman & Fertig, 2013; Strozier & Krisman, 2007). Similarly, caregivers often report inadequate financial resources to care for their children (Rushovich et al., 2017). Interestingly, Pac (2017) found that for formal caregivers increase in stipend did not have significant effect; however, a 1% increase in stipend resulted in a 27-fold decrease in placement disruption for informal kin caregivers. Caregivers report benefiting from long-term support; after kinship navigator case closure, they often need “booster shots” for intermittent and financial needs (Feldman & Fertig, 2013; Strozier & Krisman, 2007). This financial burden appears to continue, even with the influx of resources, but even minimal support could have large impacts on child safety and stability.
Despite facing stress and financial struggles, Denby et al. (2017) found that kinship families could achieve positive outcomes with adequate familial and social support. Lower income status has been associated with a deeper connection to the child and higher sense of caregiver self-efficacy. Caregivers reported not only limited financial incomes but also high willingness and competence to parent (Denby & Bowmer, 2013). Lower educational levels correlated with higher family functioning and perception of better child outcomes (Denby et al., 2014, 2017). Despite economic challenges, navigating financial burdens may be associated with resilience factors.
COVID-19 Impacts
Kin caregivers’ resources were also affected by societal stressors such as COVID-19. Non-relative foster and kinship caregivers stated comparable levels of distress for themselves and kin youth including societal and financial strain during the COVID-19 pandemic (Beal et al., 2022). Job loss resulting from the COVID-19 pandemic was felt by kinship families as they had higher financial needs and spent more time with kin children—during the lockdown—leading to higher levels of parental stress and mental distress (Xu, Wu, et al., 2022). As this is a relatively recent impact, future research may further highlight the role COVID-19 has had on caregiver economic status and ability to access resources.
Structural Support
Systemic Roles of Caregivers
Roles within a family, community, and culture may also affect the support caregivers need or receive. Despite the involvement of many biological parents in the lives of their children in kinship care, difficult relationships are often reported between kin caregivers and biological parents (Feldman & Fertig, 2013). An investigation by Zinn (2012) characterized various types of kinship families: “parenting grandparent families” live near the children’s biological parents while “empty-nest grandparent families” live farther away from children’s biological parents and are less likely to have non-foster children and other adults living in the household. Kin children in parenting grandparent families had low risks of disruption while empty-nest grandparents’ placement had adoption as a more likely result (Zinn, 2012). Youth living with grandparents were more likely to have fewer prior placements while youth living with siblings reported significantly higher levels of social connections (Zinn, 2017). Reported social and familial support were found to be lower among sibling caregivers (Denby & Ayala, 2013).
Zinn (2012) suggested that increased child stability could occur despite lower competence in parenting capacity resulting from differences in kinship families’ type. Higher scores in motivation and sustainability influences were found among unmarried caregivers (Wheeler & Vollet, 2017). Increasing caregiver age has also been found to be associated with hazard of disruption and negatively related to the hazards of reunification with birth parent and adoption. Caregivers of child-rearing age are more likely to devote time and resources to caregiving compared with older or very young caregivers, for example, grandparents or siblings (Zinn, 2012).
Denby and Bowmer (2013) suggest that family connection and social participation may be responsible for the high level of strength observed among rural caregivers. Nonetheless, it does not moderate the relationship between parental stress and well-being. More disorganized neighborhoods have a lower potential to offer social support. Xu, Jedwab, et al. (2022) observed a correlation between neighborhood disorder and children’s internalizing and externalizing behavioral issues.
Evidence also suggests that caregivers from various racial backgrounds enjoy similar levels of social support (Denby et al., 2015). Therefore, race does not seem to moderate social support among kinship caregivers. Strozier (2012) recommends sustained efforts in understanding how support group affects informal kinship caregivers and creates a good measure of kinship effectiveness. Gomez (2021) also suggests better well-being outcomes for kinship families that seek social support from household members. Among sibling caregivers, Namkung et al. (2017) found that caregiving took a significant toll on non-Hispanic white caregivers more than those from minority groups. The role of sibling caregivers is growing, but as with other subgroups of caregivers, there is limited understanding of information and support outreach services to meet their special needs (Namkung et al., 2017).
Peer Support
Caregivers who attended support groups experienced significantly higher social support than those caregivers who did not participate in support groups (Strozier, 2012). In addition, attendance may result in an increase in formal social supports (such as parent groups, social clubs, church members, family physicians, school or day-care, professional helpers, and agencies) compared with informal support (such as spouse’s parents, relatives, spouse’s relatives, spouse, friends, spouse’s friends, and children). Littlewood et al. (2022) emphasize that children whose caregivers received peer-to-peer navigation services and kinship navigation with innovation were more likely to remain in the home for up to 3 years post-intervention and less prone to a substantiated report of abuse or neglect compared with kin children whose caregivers received usual care services. Alternatively, Sharda et al. (2019) found that social support did not moderate the association between parenting stress and caregiver well-being, indicating further need to explore factors and pathways for peer support leading to well-being.
Licensure
Caregivers face different challenges based on their licensure route chosen for caregiving. Relative caregivers face a greater number of barriers to achieving licensure compared with their non-relative foster caregiver counterparts (Riley-Behringer & Cage, 2014). Formal kinship caregivers stressed a higher need for kin child counseling compared with informal caregivers. Alternatively, informal kinship caregivers reported a slightly higher need for health care, childcare, support groups, and legal services (Strozier & Krisman, 2007). As it is a less accessible population to research, there is relatively little information exploring informal caregiver needs and outcomes (Strozier, 2012).
Caregiver Health
Stress Impacting Care
Previous research indicates that parenting stress is negatively associated with caregiver well-being (Sharda et al., 2019). In a study that measured the impact of enhanced kinship navigator services by Feldman and Fertig (2013), it was found that 22% of kin caregivers caring for children less than 12 years had a stress score above the 90th percentile on the Parenting Stress Index. Garcia et al. (2015) found that kinship caregivers were more depressed compared with their foster care counterparts. However, kin children experienced significantly lower internalizing problems with caregivers within the “never depressed category.” Similar to populations at large that have seen increasing demand and limited availability for mental health care in recent years, Beal et al. (2022) reported that about half of caregivers in this study experienced barriers to accessing mental health services during the pandemic.
Generally, high levels of stress appear across demographics too. Between rural and non-rural kinship caregivers, Denby et al. (2015) found no statistically significant differences in stress and strain levels. Xu, Wu, et al. (2022) found that grandparent kinship caregivers’ mental health and parenting stress mediated or moderated caregiving behaviors and child outcomes such as engaging in corporal punishment, neglectful behaviors, sexual abuse, and child internalizing problems.
Protective Resilience
Gomez (2021) studied the relationship between family resilience and outcomes in kinship care. Family resilience was observed to be negatively correlated with parental stress and positively associated with higher ratings of caregiver mental and overall health. Resilience in kinship grandparents was reported at a higher level compared with other relative caregivers (Gomez, 2021). As discussed by Denby et al. (2017), caregivers with a lower level of stress and strain perceived a high level of child well-being. Caregivers’ mental health may play a protective buffering role in children’s behavioral problems (Xu, Jedwab, et al., 2022).
Discussion
Many people who have caregiver responsibilities are often without adequate support due to limited knowledge of or access to available resources. It has been proven that these families are able to achieve positive outcomes if equipped with the right tools and aid (The Annie E. Casey Foundation, 2012). Our findings indicate that caregivers face challenges in universally achieving these positive outcomes, at least in part due to their characteristics and demographics. This includes racial and ethnic representation in research informing outreach, favoring particular family roles as caregivers, compounded economic burden, access and engagement with societal supports, and caregivers’ health status impacting outcomes. These characteristics may influence assumptions program providers make about their target audience as well as guide potential barriers or enablers caregivers might encounter in receiving support. Without exploring the influences pre and post KNP service, providers may miss opportunities for adaptation to meet contextual factors such as community resources, historical or current trauma, economic conditions, or social trends (McLaughlin & Jordan, 2015).
Racial and Ethnic Representation
This disproportional overrepresentation of minorities is a call for concern and highlights the need to evaluate enhanced navigation services tailored for these marginalized populations. These same populations often face health and economic inequities. There remains a high level of distrust between kinship caregivers and the government, with many reporting feeling judged by caseworkers from child welfare agencies as well as perpetuation and unresolved historical trauma in racial and cultural communities affecting kinship families as well (Rodriguez-JenKins et al., 2021). Findings from Rushovich et al. (2017) suggest that having a dedicated navigator outside the child welfare system can help rebuild trust and openness. Additional research should aim to ensure representative samples and consider opportunities for tailoring programming to meet unique racial or ethnically diverse kin caregiver needs.
Favor Family Role
Findings support that different family roles may benefit from different supports to achieve equitable outcomes. While females are currently the preferred or most common caregivers, these gender preference in kinship caregiving should be reconsidered accounting for more influential factors. As discussed by Denby et al. (2014), male kin caregivers represent an untapped social capital within the child welfare system and with adequate support they could help fill the gaps of foster home shortages. Further research should consider whether navigator programs benefit from considering resources in relation to familial role of the caregiver.
Economic Burden
While financial instability is universally associated with kin caregiving families, caregiver characteristics are associated with greater or less challenge in accessing resources to reduce economic inequity. Navigating economic uncertainty may grow resilient and protective factors for kin caregivers. Most likely benefit from financial assistance, but some assistance is out of reach. Foster care licensure currently improves access to financial resources for caregivers. The Older Americans Act only provides financial aid to caregivers above age 60, whereas empirical evidence exists that many caregivers are below 60 years old (Strozier & Krisman, 2007; Zinn, 2012). The age requirement for assistance should be replaced with other metrics that adequately signify need. Relative caregivers also face more financial difficulty and challenges accessing primary care for their kin child (Schneiderman et al., 2012). There may be opportunities to reduce inequity by considering what factors that put kin families at risk of greater challenges in accessing these supports.
Structural Support
Identification and navigation of interpersonal supports are often protective factors for caregivers (Strozier, 2012). At times, these supports are already in place for kin caregivers, but when they are not, research indicates it can be more difficult for some caregivers to connect with these protective supports. The relative ease of organizing support groups and the low financial requirements compared with other kinship interventions make it an attractive form of kinship support. They can increase informal and formal social support for kinship caregivers across diverse backgrounds (Strozier, 2012).
The use of computer software to provide caregiver support (reading and parenting skills) was explored by Loree et al. (2014), which yielded promising results. With recent increases in technology adoption and self-efficacy, future internet or computer-based intervention services can be made available and accessible to caregivers. More research should specifically explore impactful support strategies, needs, and strengths of informal caregiver families (Strozier, 2012).
Caregiver Health
Stress is ubiquitous for kin caregivers and research indicates it is potentially affecting care outcomes. Similar to other parenting populations, resilience to these negative outcomes is also occurring, especially when caregivers have structural supports (Huang et al., 2019). In addition to the varying mental and physical health challenges faced by kin caregivers, barriers to mental health resources remain prevalent for this population (Beal et al., 2022; Garcia et al., 2015). Higher incomes were found to be positively correlated with improved caregiver well-being (Gomez, 2021). Research and evaluation should consider the impacts of extended-duration services for kin caregivers as well as engagement that could reduce caregiver stress, increase access to resources, and build family resilience.
Limitations
This review is limited by the scope of currently published research as well as the individual limitations of studies represented. While we can consider the potential mechanisms by which these factors may be contributing to outcomes, we cannot generalize across kinship caregiving populations. A strength of this study is that it allows us to highlight the important nature of diversity in kinship families influencing both research and practice into the future. As kinship programs and support are developed and evaluated, they should further consider how these characteristics may be contributing to their research questions and outcomes.
Implications for Research and Practice
Literature supports the hypothesis that kin caregiver characteristics influence kinship outcomes. This review faced limitations in translation as the body of research with diverse kin caregiver characteristics is small. Future research should continue to highlight and explore these protective and risk factors while simultaneously evaluating programs that can meet unique and heterogeneous needs of kin families. Caseworkers, navigators, kinship support agencies, funders, and policymakers must continue to evaluate the impacts of support strategies considering diverse caregiver characteristics. By growing our knowledge of the complex characteristics affecting inequities, evidence-based programming can identify the most impactful opportunities for reducing disparities in kinship caregiver and kin youth outcomes.
Footnotes
Appendix
Disposition editors: Angelique Day and Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Montana Department of Public Health and Human Services (grant number 20213IVEE0001).